Hypercalciuria and febrile convulsion in children under 5 years old
Article information

Abstract
Purpose
The association between hypercalciuria and febrile convulsion is controversial. The present study aimed to investigate the statistical association between hypercalciuria and childhood febrile convulsions.
Methods
Overall, 160 children aged 6 months to 5 years, including 80 children with febrile convulsion and 80 febrile children without convulsion (comparison group), were recruited. All laboratory tests, including 24-hour urine calcium, were undertaken in an academic clinical laboratory.
Results
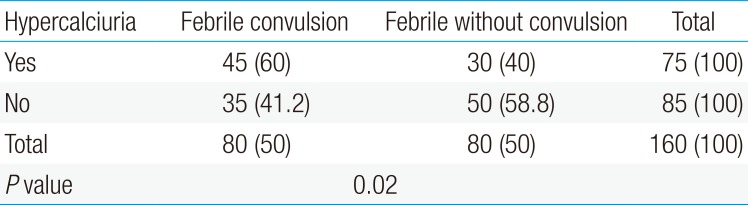
Forty-five children of the febrile convulsion group (60%) and 30 of the comparison group (40%) had hypercalciuria. There was a significant difference between the 2 groups (P=0.02).
Conclusion
Our results indicated that there is a statistical association between convulsion and hypercalciuria in children. Since we found this association with a cross-sectional assessment, further studies, especially prospective and controlled designs, are needed.
Introduction
Febrile convulsion is the most common type of seizures in childhood.1) The prevalence rate of febrile convulsion in Iran has been reported 8.8% among children aged 13–60 months.2) By definition, seizures with fever higher than 38.5℃ at the age of 6 months to 5 years in the absence of underlying brain disease and brain infection is called febrile convulsion.3) Previous studies have mentioned several factors such as genetic, familial history of febrile convulsion, history of hospitalization after birth, low birth weight, maternal smoking during pregnancy and changes in trace elements as risk factors for febrile convulsions.4567)
Calcium ion (Ca) via relative depolarization of neurons sheath and activation of voltagedependent sodium channels are involved in the pathophysiology of seizure.8) Hypocalcemia (Ca <8.5 mEq/L) makes the muscle skips, paresthesia of face and extremities, spasms, stridor, and seizures. Hypercalciuria is the most common cause of kidney stones. It occurs in 2 pathologic and idiopathic modes.1) Hypercalciuria was defined as calcium excretion higher than 4 mg/kg/day.9)
Variety of pathological conditions affects the calcium excretion via urine. One of the idiopathic hypercalciuria is renal which causes a negative calcium balance leading to calciopenic state. In these children fever increases the respiratory rate and causes respiratory alkalosis and hypocalcaemia affecting the pathophysiology of febrile seizures.10)
Since the results of various studies on the relationship between Hypercalciuria and febrile convulsion is controversial,51112) the present study aimed to investigate the relationship between hypercalciuria and febrile convulsion in children aged between six months to 5 years.
Materials and methods
It was a retrospective cross-sectional study in 2 groups including children with febrile convulsion and febrile children without convulsion. Febrile convulsion group consisted of 80 children with a first episode of febrile convulsion and comparative group was 80 febrile children without seizure. The comparative group was children with diseases such as upper and lower respiratory infection, gastroenteritis, and other common disease. Children of 2 groups were patients who referred to the pediatric emergency ward in Be'sat hospital, Sanandaj, Kurdistan province in northwest of Iran during a year from September 2010 to September 2011. Inclusion criteria included children aged 6 months to 5 years with generalized tonic or generalized tonic-clonic seizure and temperature of at least 38.5℃. Children with history of neurologic epilepsy, previous febrile convulsion, seizure attack more than twice a day or 15 minutes, preexisting neurologic abnormalities, developmental delay, a central nervous system infection or having any other chronic diseases were excluded from the study.
The laboratory tests including PH, PCO2, HCO3, sodium (Na), potassium (K), calcium (Ca), blood urea nitrogen (BUN), creatinine (Cr), serum/Ca, urine/Ca, and 24-hour urine calcium were examined for both groups.
A checklist containing demographic and clinical information such as age, sex, history of urinary stone, familial history of febrile convulsion was completed for all participants.
This study was approved by the Kurdistan University of Medical Science Ethical Committee (IR.MUK.REC.1390.43). An informed consent was obtained from parents of children.
Statistical analyses were performed with IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA) using raw scores. Fisher exact test was used for the analysis of categorical data, and Student t test for continuous variables with normal distribution. Multivariate logistic regression was used for adjusting the odds ratios (ORs) according to subject's age and sex. An OR with a 95% confidence interval was used to test differences within groups. In all analyses, P values of <0.05 were taken to indicate statistical significance.
Results
Overall 160 children including 100 male and 60 female patients in 2 groups were recruited. The mean age and standard deviation of studied children in each group, with and without febrile convulsion, was 26.1±15.1 months and 27.6±17.5 months, respectively. There were no significant differences between 2 groups in terms of age (P=0.5) and sex (P=0.6).
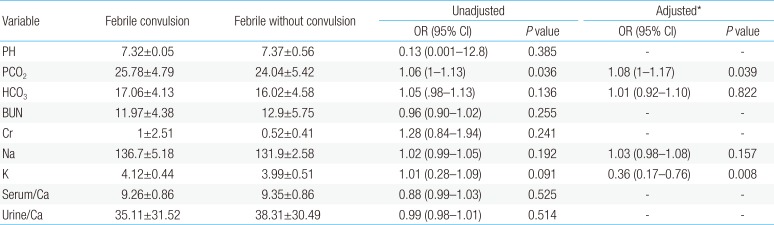
Proportions of hypercalciuria existence in each studied groups were shown in Table 1. Hypercalciuria was found in 45 children with febrile convulsions (60%) and 30 children (40%) in febrile without convulsion group (P=0.02). The laboratory data of children with febrile convulsions are shown in Table 2. PCO2 (P=0.039) and K (P=0.008) were higher in febrile convulsion group. Other indexes had no significant differences between the 2 groups.

Comparison of hypercalciuria between children with and without febrile convulsion

Comparison of serum and urine levels of some indexes between the 2 groups
Discussion
The main objective of the present study was to investigate the association between hypercalciuria and febrile convulsion in children less than 5 years old. The highest prevalence of hypercalciuria was observed among children with febrile convulsion compared to febrile children without convulsion. There were no significant differences between the 2 groups in terms of HCO3-PH- BUN- Ca- Na and K which is similar to Mohammadi in Iran.13)
The hypercalciuria rate observed in the present study was not consisted with the latest published reports might be due to an adequate sample size in the present study. It has been reported that the prevalence of hypercalciuria in children without convulsion were 37.8% which is similar to the present study.14) There was a significant association between hypercalciuria and febrile convulsion. The exact pathogenesis of relationship between febrile seizures with hypercalciuria is not clear. But its possible mechanism it could be that respiratory alkalosis due to increased body temperature increases body PH, which in turn reduces the production of ionized calcium. So in a child with hypocalcemic hypercalciuria, this mechanism can cause seizures.5) In present study, although it was not significant, but the mean of serum Ca was lower in children with febrile convulsion. We cannot interpret without cautions; this study had not sufficient evidence for confirming causality between hypercalciuria and febrile convulsion, but our results showed the association between these 2 occurrences.
The main limitation of the present study was the lack of evaluation of other laboratory tests related to hypercalciuria such as parathyroid hormone, ionized calcium.
Our results indicated that there is statistical association between convulsion and hypercalciuria in children. Since we found this association with a cross-sectional assessment it needs further studies especially prospective and controlled designs.
Acknowledgments
This study was funded by Kurdistan University of Medical Science.
Notes
Conflicts of interest: No potential conflict of interest relevant to this article was reported.