Epidemiology of Kawasaki disease in infants 3 months of age and younger
Article information
Abstract
Purpose
This study investigated the epidemiology of Kawasaki disease (KD) in infants ≤3-month-old.
Methods
To study the epidemiology of KD in Korea, data for 27,851 KD patients were collected on a 3-year basis between 2000 and 2008 in a retrospective survey. From this, data for 609 KD patients ≤3-month-old were analyzed and compared with the data for KD patients >3-month-old.
Results
The 609 KD patients ≤3-month-old (385 males and 224 females) constituted 2.2% of the KD patients. They included 25 infants <1-month-old, 198 infants ≤1- to 2-month-old, and 386 infants >2- and 3-months-old. The ratio of males to females was 1.72:1. The incidence of coronary artery (CA) dilatation (19.9% vs. 18.7%) and CA aneurysms (3.4% vs. 2.6%) detected by echocardiography did not differ significantly between patients with KD younger and older than 3-month-old.
Conclusion
Compared with the data for the KD patients >3-month-old, the data for the 609 patients ≤3-month-old did not show a significantly higher incidence of CA dilatation or CA aneurysms.
Introduction
Kawasaki disease (KD) is an acute febrile illness, predominantly affecting children younger than 5 years of age. Since its first description in 1967 by Dr. Tomisaku Kawasaki1), KD has become recognized as the leading cause of acquired heart disease in children in developed nations.
The peak age incidence of KD is from 6 months to 2 years of life2,3), and it is rare in infants ≤3 months of age4,5). Consequently, this survey, which was conducted in 2011 and targeted KD patients who were admitted between 2000 and 2008, will present recent epidemiologic features for infants ≤3 months of age.
Materials and methods
1. Time and method of investigation
This epidemiological study of KD in Korea was carried out under the purview of the Korean Pediatric Heart Association and the Korean Kawasaki Disease Study Group. Data were collected retrospectively in a questionnaire administered to KD patients newly diagnosed within the 9-year period from January 2000 to December 2008 in all hospitals that have pediatric residency programs6-11).
The 101 general hospitals in Korea were approved as pediatric resident training hospitals by the Korean Hospital Association, and most of the KD patients were admitted to these hospitals. Hence, both mail and internet based questionnaires were sent to these hospitals in January of 2003, 2006, and 2009. The survey format included the diagnostic criteria for KD itself and coronary artery (CA) lesions, and the items in the questionnaire included age, sex, age at onset, sibling case, recurrent case, echocardiography findings, coronary angiography findings, myocardial infarction case, death case, and number of KD patients among all hospitalized pediatric patients.
From this 9-year survey9-11), data for 609 KD patients ≤3 months of age were analyzed and compared with those of KD patients >3 months of age in terms of the epidemiological findings and findings regarding CA lesions.
2. Diagnostic criteria for Kawasaki disease and CA lesions
The diagnosis of KD was based on the clinical features, which included a fever for at least 5 days and four of the following five signs: bilateral conjunctival injections; oral mucosal changes, such as an injected pharynx, dry cracked lips, or a strawberry tongue; changes in the hands and feet, such as redness and swelling in the acute phase, and periungual desquamation in the subacute phase; rash, primarily on the trunk, that may be maculopapular, erythema multiforme, or scarlatiniform; and cervical lymph nodes greater than 1.5 cm in diameter.
Patients with CA dilatation or a CA aneurysm were also included. Normal ranges for CA size defined according to age or body weight were used. In children younger than 5 years of age, an internal lumen diameter (ILD) ≤3.0 mm is considered normal, and in children aged 5 years or older, an ILD ≤4.0 mm is considered normal11). In three groups of children, that is, those weighing <12.5, 12.5 to 27.5, and >27.5 kg, the normal ranges of ILD were ≤2.5, 2.5 to 3.0, and 3.0 to 5.0 mm, respectively12). If the ILD of the CA segment is enlarged less than 1.5 times the upper normal limit, it is defined as dilatation, and if the ILD is enlarged 1.5 times or more, it is defined as an aneurysm.
3. Statistical analysis
To evaluate the trends in the data during the period 2000 to 2008, we analyzed the data for each year in terms of the ratio of males to females, sibling cases, and prevalence of CA lesions using the χ2 test for trend (Mantel-Haenszel χ2). Statistical analyses were performed using SAS ver. 6.12 (SAS Institute Inc., Cary, NC, USA), and a P value <0.05 was considered statistically significant. The Ethics Board of The Catholic University of Korea Uijongbu St. Mary's Hospital approved this survey.
Results
A total of 27,851 KD patients were reported for the 9 years: 9,150 in 2000 to 20029), 9,662 in 2003 to 200510), and 9,039 in 2006 to 200811). There were 609 KD patients ≤3 months of age (385 males, 224 females), which constituted 2.2% of all KD patients. The ratio of males to females was 1.72:1, showing a predilection for boys. They included 25 patients age ≤1 month, 198 age 1 to 2 months, and 386 age 2 to 3 months. There was no prevalence of KD in siblings. Of the total, 1.1% (7/609) had recurrences.
Echocardiography was carried out during hospitalization and follow-up in 95.7% of the patients ≤3 months of age (583/609), and CA lesions were observed in 19.9% of the cases (116/583), including CA dilatation in 105 cases (18.0%) and CA aneurysms in 20 cases (3.4%). Of these 583, 96 cases (16.4%) had pure CA dilatation, 11 cases (1.8%) had a CA aneurysm only, and 9 cases (1.5%) had both CA dilatation and a CA aneurysm.
Comparison of the echocardiographic findings with regard to gender in the KD patients ≤3 months of age showed a higher prevalence of CA dilatation and CA aneurysms in male KD patients than in female KD patients, but the difference was not significant (P>0.05) (Table 1).
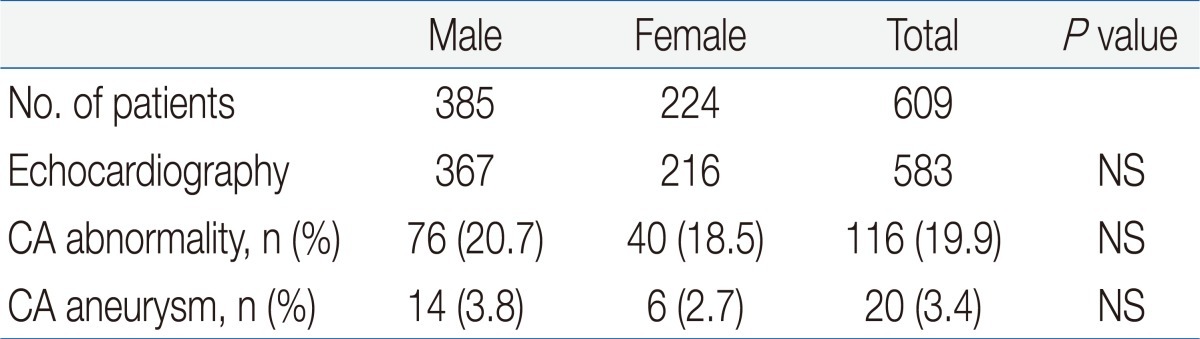
Comparison of Echocardiographic Findings between Male and Female Kawasaki Disease Patients 3 Months of Age and Younger
We compared the ratio of males to females, recurrence cases, and CA lesions between KD patients ≤3 months of age and KD patients >3 months of age. There was no significant difference in the prevalence of CA dilatation or CA aneurysms between the two groups (P>0.05). Specifically, there was no significantly higher prevalence of CA dilatation or CA aneurysms in KD patients ≤3 months of age than in KD patients >3 months of age (19.9% vs. 18.7%, P>0.05 or 3.4% vs. 2.6%, P>0.05, respectively) (Table 2). However, there was a significantly higher prevalence of recurrence cases (1.1% vs. 2.4%, P<0.05). There were no reports of myocardial infarction or death.
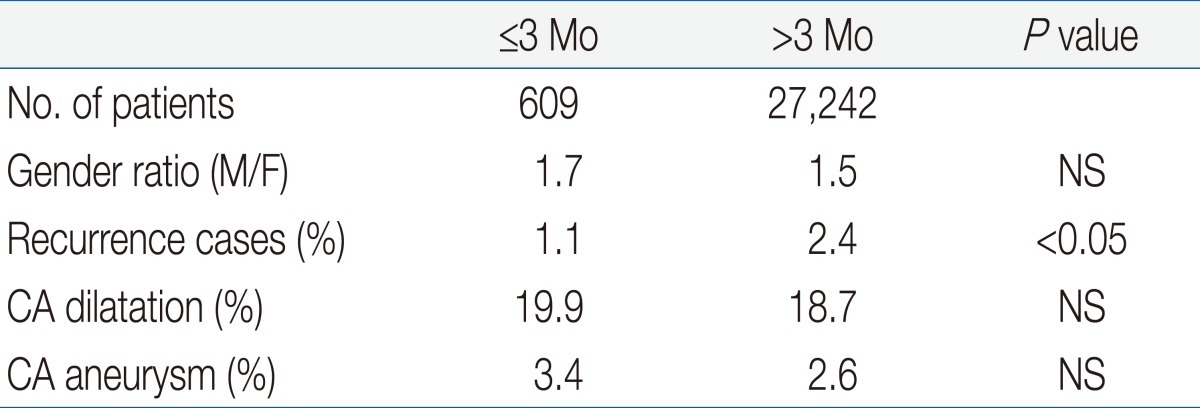
Comparison between Kawasaki Disease Patients 3 Months of Age and Younger
Discussion
Kawasaki disease (KD) predominantly affects children younger than 5 years of age, which accounts for 80% of the cases, and the peak age of onset is 6 to 24 months of age, which includes approximately 50% of all KD patients2,3). The latest nationwide epidemiological survey11) also revealed that KD occurred predominantly in children <5 years of age (87.0%), as compared with all KD patients. There is a very low incidence reported in KD patients ≤3 months of age13-15) or KD patients >8 years of age16,17), and few cases of KD patients in the neonatal period have been reported13,14).
The presumptive explanations for this phenomenon are the protective effect of passive immunity transmitted from the mothers and the lower possibility of exposure to unknown pathogens floating in the air because the infants live indoors. Relative to KD patients ≤3 months of age, a higher incidence of CA lesions in KD patients ≤6 months of age was reported because of the rare incidence and incomplete clinical manifestations as compared with KD patients >6 months of age4,5,18). The proportion of KD patients ≤6 months of age in relation to all KD patients is approximately 10%4,5,18,19), which is similar to the 11.2% from Japan19), and 7.7% from Korea20). In addition, the incidence of KD patients ≤3 months of age was 1.7% in Japan13) and 2.2% in Korea.
Our comparison of the incidence of CA lesions between KD patients ≤3 months of age and KD patients >3 months of age found no significantly higher prevalence of CA dilatation or CA aneurysms (19.9% vs. 18.7% or 3.4% vs. 2.6%, respectively). We speculate that the reasons for this unexpected result are first, the very small number of KD patients ≤3 months of age among all KD patients. Second, most pediatricians use the redness at the site of Bacillus Calmette-Guerin (BCG) inoculation as an important tool for diagnosing incomplete KD, because, almost all neonate receive BCG immunization in Korea. Third, the majority of pediatricians have a high index of suspicion for incomplete KD, and, early diagnosis can reduce the incidence of incomplete KD in Korea. However, we could not compare our data with the other data because, there has been no nationwide epidemiological study comparing the incidence of CA lesions between KD patients ≤3 months of age and KD patients >3 months of age.
Therefore, a diagnostic approach with a high index of suspicion for very young infants who have a high fever with no definite clinical manifestations of KD is crucial to prevent CA lesions.