Clinical characteristics and outcomes among pediatric patients hospitalized with pandemic influenza A/H1N1 2009 infection
Article information
Abstract
Purpose
The purpose of this article is to describe the clinical and epidemiologic features and outcomes among children hospitalized with pandemic influenza A/H1N1 2009 infection.
Methods
We retrospectively reviewed the charts of hospitalized pediatric patients (<18 years) diagnosed with pandemic influenza A/H1N1 2009 infection by reverse-transcriptase polymerase chain reaction at a tertiary hospital in Seoul, Korea, between September 2009 and February 2010.
Results
A total of 72 children were hospitalized with pandemic influenza A/H1N1 2009 infection (median age, 6.0 years; range, 2 months to 18 years). A total of 40% had at least 1 underlying medical condition, including asthma (17%), malignancies (19%), and heart diseases (17%). Of the 72 patients, 54 (76%) children admitted with H1N1 infection showed radiographic alterations compatible with pneumonia. There was no significant difference in pre-existing conditions between pandemic influenza A/H1N1 infected patients with or without pneumonia. Children with pandemic influenza A/H1N1 pneumonia were more likely to have a lower lymphocyte ratio (P=0.02), higher platelet count (P=0.02), and higher level of serum glucose (P=0.003), and more commonly presented with dyspnea than did those without pneumonia (P=0.04).
Conclusion
No significant differences in age, sex, or presence of preexisting conditions were found between children hospitalized with pandemic influenza A/H1N1 H1N1 influenza infection with pneumonia and those without pneumonia. Higher leukocyte count, higher glucose level, and a lower lymphocyte ratio were associated with the development of pandemic A/H1N1 2009 influenza pneumonia.
Introduction
The pandemic influenza A/H1N1 viral infection was first identified in March 20091); this virus was antigenically and genetically unrelated to human seasonal influenza viruses, but genetically related to viruses known to circulate in swine2). The world experienced its first wave of pandemic influenza A/H1N1 activity in the spring of 2009, followed by a second wave in the fall, peaking at the end of October. An early report on 18 hospitalized patients who were victims of the initial outbreak in Mexico showed that the pandemic H1N1 2009 virus caused severe illness and death in previously healthy young to middle-aged individuals; it has since been noted that the majority of patients continue to experience mild illness1).
There have been a few reports of H1N1 characteristics and outcomes among children hospitalized with pandemic influenza A/H1N1 2009 viral infection3,4). Although children are considered to be more vulnerable to pandemic influenza pneumonia, few reports describe the characteristics of this pneumonia in pediatric patients5,6). This study describes the clinical and epidemiologic features of the viral infection among pediatric patients hospitalized with pandemic influenza A/H1N1 pneumonia from September 2009 to February 2010 at a tertiary medical center in Korea.
Materials and methods
We reviewed the medical charts and radiologic and laboratory findings of all children admitted to Asan Children's Hospital in Korea between September 2009 and February 2010; the hospital is a tertiary, academic medical center.
We included children with pandemic influenza H1N1 confirmed by reverse-transcription polymerase chain reaction (RT-PCR). The clinical criteria for a diagnosis of H1N1 pneumonia in the hospitalized pediatric patients was based on abnormal breath sound such as crackle, rale, or rhonchi and opacities found on the chest radiography at admission. The chest radiographs were reviewed by two radiologists, and final decisions on the findings were reached by consensus.
Clinical characteristics were compared between patients with pandemic A/H1N1 pneumonia and those with pandemic A/H1N1 infection and between children less than 5 years and those older than 5 years. Patients who were admitted because of pandemic influenza A/H1N1 infection were also subcategorized by clinical outcome as those requiring respiratory support by nasal cannula, those requiring mechanical ventilation, and those requiring admission to the intensive care urnit (ICU).
1. Microbiological studies
Nasopharyngeal swab specimens (Flexible Minitip 503CS01 Flock Swabs, Diagnostic Hybrids, Athens, OH, USA) were collected at admission. Specimens were placed in 3 Ml Universal Transport Medium (Diagnostic Hybrids) and kept at 2 to 4℃. RT-PCR testing was done in accordance with published guidelines from the U.S. Centers for Disease Control and Prevention.
2. Statistical analysis
We compared data between patients with pandemic H1N1 pneumonia and those with pandemic H1N1 infection without pneumonia. Logistic regression was used to identify the characteristics of the children in each group. The Fisher's exact test was used to compare categorical variables. Statistical analysis was performed with the SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). A P value of less than 0.05 indicated a significant difference.
Results
1. Patient characteristics
In our institution, 11,662 pediatric patients (all under 18 years of age) were tested for pandemic influenza A/H1N1 2009 from September 2009 to February 2010 (Table 1). Among them, 5,367 patients (46%) tested positive; 72 of the 5,367 patients were admitted to the hospital, and 54 of these 72 patients had pandemic influenza A/H1N1 pneumonia confirmed by means of RT-PCR (Table 2). The epidemic curve of pediatric patients hospitalized with pandemic influenza A/H1N1 with or without pneumonia in Korea is shown in Fig. 1. Of these 72 patients, 54 (75%) were male. The median age was 6.0 years. Fig. 2 shows the age distribution of children hospitalized with pandemic H1N1 pneumonia or pandemic H1N1 infection alone. Of the 18 children without pneumonia, 17 were diagnosed with upper respiratory infection and the remaining 1 patient was diagnosed with Kawasaki disease.
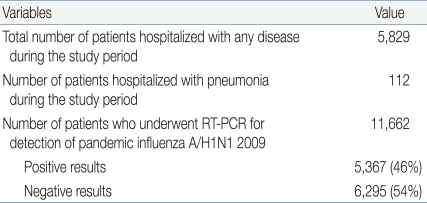
Analyses of Patient Variables from September 2009 to February 2010
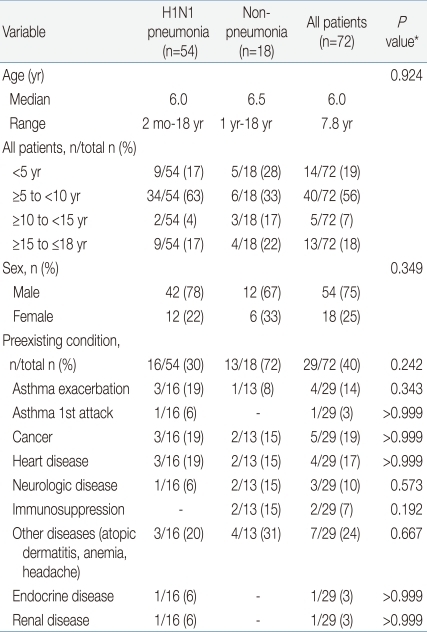
Epidemiologic Features, Preexisting Conditions, Clinical Symptoms in Children Hospitalized with 2009 H1N1 Influenza
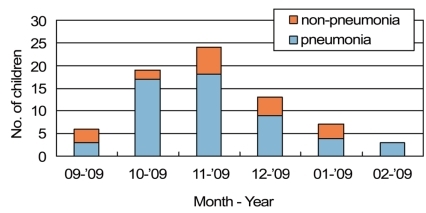
Seasonal pattern of hospitalization of children for pandemic H1N1 influenza with or without pneumonia.
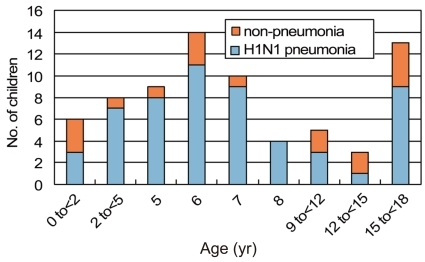
Age distribution of children hospitalized for pandemic H1N1 influenza with or without pneumonia.
2. Preexisting medical conditions
A total of 40% of patients had at least 1 preexisting medical condition: 30% and 72% in the H1N1 pneumonia group and the group without pneumonia (P=0.24), respectively. In the H1N1 pneumonia group, asthma was the most common medical condition (25%), and the children presented with exacerbation of asthma or a first attack.
3. Clinical features
Fever (temperature above 37.8℃) and cough were the most common presentations at admission in both groups (Table 3). The next most common symptom was dyspnea in the pandemic H1N1 pneumonia group (n=35, 65%), and rhinorrhea (n=7, 39%) in the group without pneumonia. Nausea and vomiting were more common in the group without pneumonia (22% for both symptoms) compared with the pandemic pneumonia group (6% and 9%, respectively); however, this difference was not significant. Sputum was a more common symptom in children older than 5 years than those aged less than 5 years.

Clinical Symptoms in Children Hospitalized with 2009 H1N1 Pneumonia or without Pneumonia
4. Laboratory tests on admission
Children with pandemic H1N1 pneumonia were more likely to have a lower lymphocyte ratio (P=0.02), higher platelet counts (P=0.02), and a higher level of serum glucose (P=0.003) than those without pneumonia (Table 4).
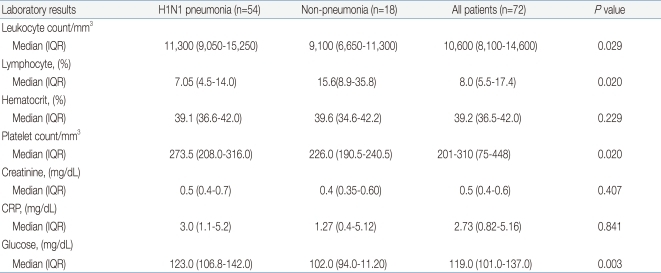
Results of Laboratory Tests in Children Hospitalized with Pandemic Influenza A/H1N1 2009 Pneumonia or without Pneumonia
5. Radiographic evaluation
Chest radiography was performed in all children admitted with pandemic influenza A/H1N1 infection; 54 children (75%) had findings consistent with pneumonia. On an average, the initial chest radiographs for all patients (n=72) were obtained 1.2 days (range, 0 to 7 days) after the onset of clinical symptoms. In the pandemic H1N1 pneumonia group, initial chest radiography revealed unilateral abnormalities in 37%, bronchopneumonial pattern in 57% (n=31), consolidation patterns in 43% (n=20), and mixed patterns in 6% (n=3) (Table 5). The chest computed tomography scans obtained for 11 of these patients showed bilaterally distributed lung parenchymal lesions that had peribronchial ground-glass opacities (n=7), patchy consolidations (n=5), and interstitial thickening (n=1). The mediastinal and perihilar lymph nodes were detected in 1 patient, pleural effusion was noted in 3 patients, and pneumomediastinum was detected in 2 patients.
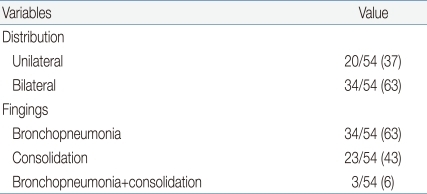
Distribution and Radiologic Findings in the H1N1 Pneumonia Group
6. Severity of illness and outcomes
Oxygen supplementation was provided to 67% of the children hospitalized with pandemic H1N1 pneumonia, and to 6% of children without pneumonia. Three patients were admitted to the ICU. Of the 3 pediatric patients who required mechanical ventilation, 2 were male, and the sole female had a preexisting hematologic malignancy, and hers was the only death in this study. This patient had a 2-day history of fever, cough, and sputum. Her initial laboratory results were as follows: leukocyte count 3,300/mm3, platelet count 75,000/mm3, aspartate aminotransferase 400 IU/L, alanine aminotransferase 305 IU/L, lactate dehydrogenase 977 IU/L, C-reactive protein 0.82 mg/dL, and creatine kinase 24 IU/L. She received oseltamivir (150 mg twice a day), amatadine (100 mg twice a day), azithromycin, ceftazidime and vancomycin until her death on hospital day 17. She remained positive for influenza A RNA as assessed by RT-PCR 2 days after administration of antiviral medication; no other viral pathogens were cultured and amplified by PCR when bronchoalveolar lavage (BAL) and sputum samples were taken, and bacterial cultures from the same specimens showed no growth. Complications in this patient included hypovolemic shock and respiratory failure.
7. Treatment
All pediatric patients suspected having pandemic H1N1 infection were administered oseltamivir before the results of the H1N1 RT-PCR were known. The median time from the onset of symptoms to the initiation of antiviral therapy was 1.1 days (range, 0 to 5 days) in the pneumonia group and 1.7 days (range, 0 to 7 days) in the group without pneumonia; this difference was not significant (P=0.24). Antibiotics were administered to 94% of patients in the pandemic H1N1 pneumonia group, and to 61% of those without pneumonia. Oseltamivir resistance does not performed in all patients.
Discussion
Children admitted to a tertiary hospital in Korea with pandemic influenza A/H1N1 2009 infection during the second wave of the pandemic showed a wide spectrum of disease, ranging from upper respiratory infection alone to severe illness and death.
The chest radiography findings on admission were consistent with those for pneumonia in 54 (75%) of the pediatric patients hospitalized with pandemic influenza A/H1N1 2009 infection. However, no significant differences were observed between the pandemic influenza A/H1N1 2009 pneumonia group and the pandemic influenza A/H1N1 2009 infection group with respect to age, sex, or the presence of preexisting conditions. In addition, no significant differences were observed between these groups with respect to the time between the onset of symptoms and the initiation of oseltamivir therapy (pneumonia group: mean period, 1.1 days; non-pneumonia group: mean period, 1.7 days). The patients from the pandemic influenza A/H1N1 2009 pneumonia group had higher leukocyte counts, higher glucose levels and lower lymphocyte ratios than did the patients from the group without pneumonia.
Some reports have suggested that children less than 5 years old are at the highest risk of seasonal influenza-associated hospitalizations7-9); in our study, pediatric patients aged 5 to 18 years accounted for 83% of patients in the pandemic H1N1 pneumonia group and 72% of those in the pandemic H1N1 group without pneumonia (Table 2). In a study on patients hospitalized with 2009 H1N1 influenza in the United States, the study population included a greater proportion of children older than 5 years (29%) than of children younger than 5 years (15%)10). Children aged less than 5 years were hospitalized more frequently because of either different admission criteria or diagnostic method for pneumonia in each hospital. Therefore, we cannot definitely conclude that children aged less than 5 years are at the highest risk for influenza-associated hospitalization. The median duration of viral shedding, as determined by positive RT-PCR results, was 2.0 days for children younger than 5 years and 3.81 days for children older than 5 years (P=0.59). The reason for this age distribution and for the difference in the duration of viral shedding for each age group is uncertain; however, these findings may be related to the higher possibilities of contact with and of repeated or prolonged exposure to this virus in the case of children older than 5 years at schools.
Approximately one-quarter to one-half of patients with pandemic influenza A/H1N1 2009 viral infection who were hospitalized or who died had no reported coexisting medical conditions10-13). In our study, 40% of pediatric patients with pandemic H1N1 infection had preexisting conditions. However, there was no significant difference between patients in the pandemic H1N1 pneumonia group and those in the group without pneumonia. The pandemic influenza A/H1N1 2009 virus causes pneumonia regardless of preexisting medical conditions; this may be because the virus has a strong affinity for the lower respiratory tract and the affected population did not have antibodies specific to this virus1,2,14).
In our study, dyspnea was the only clinical feature at presentation that differed significantly between patients in the pandemic H1N1 pneumonia group and those in the group without pneumonia. Because we considered shortness of breath or breathing discomfort to be indicative of dyspnea, there was no significant difference in respiratory rates between the groups.
The risk factors for pandemic influenza A/H1N1 pneumonia are still unclear; however, a significantly greater number of the patients with pneumonia presented with higher leukocyte counts, higher glucose levels and lower lymphocyte ratios than did the patients without pneumonia. In a few studies, patients admitted with pandemic influenza A/H1N1 infection showed increased serum concentrations of lactate dehydrogenase and creatinine kinase1,15). In our study, the presence of pandemic H1N1 pneumonia did not affect these levels, but the level of glucose was elevated in the pandemic H1N1 pneumonia group, compared with the group without pneumonia. The most likely explanation for this may be the stress effect of H1N1 infection complicated by pneumonia.
The radiographs for patients with pandemic influenza A/H1N1 pneumonia showed prominent peribronchial marking with hyperinflation, similar to that observed in other common viral respiratory infections16). In contrast, the radiographs for children with a more severe clinical course of pandemic influenza A/H1N1 infection typically show a bilateral symmetrical distribution pattern of areas of consolidation that are often associated with ground-glass opacification. In this study, the patients (n=6) who were admitted to the ICU or required mechanical ventilation had bilateral symmetric distribution of consolidation or ground-glass opacities.
The rate of bacterial or other viral co-infection was 4.2%; 1 patient was co-infected with respiratory syncytial virus and mycoplasma in the pandemic influenza A/H1N1 pneumonia group, and 2 patients with adenovirus and streptococcal pneumonia, in the pandemic influenza A/H1N1 group without pneumonia. We could not find any relationship between co-infections and the severity of disease; these 3 patients did not need any oxygen supplementation and were not admitted to the ICU.
A study performed between May and July 2009 showed that the hospitalization rate for pandemic influenza A/H1N1 among children was twice that for 2008 seasonal influenza in the same population. Moreover, the death rate was 10 times the rate associated with seasonal influenza for the same population in 20074,17). In contrast to the findings of these studies, the results of another study reported that the overall hospital mortality rates for all age groups was 1.1% and that for children was 0.24% in Japan18). In our study, the death rate due to pandemic influenza A/H1N1 2009 was low (1.4%), although there is some limitation due to small sample size. These differences may be partially due to the recommendation, which was put forth in September 2009 in Korea, that empirical therapy with oseltamivir be administered to patients with influenza-like symptoms-especially to children at high-risk and children who were hospitalized; the differences may also exist because the other studies included both pediatric and adult patients.
Our study includes a limited number of cases and was of short duration. The need for hospitalization due to pandemic influenza A/H1N1 2009 infection was decided by several attending physicians without any objective indications. The availability of hospital or ICU beds may have influenced assessment of the severity of disease. This study cannot represent the full spectrum of pandemic influenza A/H1N1 2009 influenza infections because it was performed at a tertiary hospital.
In conclusion, hospitalization with pandemic H1N1 influenza infection affected children without any significant differences in age, sex, or the presence of preexisting conditions between the pandemic H1N1 pneumonia group and those without pneumonia. A higher leukocyte count, higher glucose level and a lower lymphocyte ratio together with dyspnea were associated with the development of pandemic influenza A/H1N1 2009 influenza pneumonia.
Acknowledgement
The authors thank all the patients involved in this report and all the pediatricians and hospital staff involved in their care.