The relationship between eosinophilia and bronchopulmonary dysplasia in premature infants at less than 34 weeks' gestation
Article information
Abstract
Purpose
Eosinophilia is common in premature infants, and its incidence increases with a shorter gestation period. We investigated the clinical significance of eosinophilia in premature infants born at <34 weeks gestation.
Methods
We analyzed the medical records of premature infants born at <34 weeks gestation who were admitted to the neonatal intensive care unit at Ewha Womans University Mokdong Hospital between January 2003 and September 2010. Eosinophilia was defined as an eosinophil percentage of >3% of the total leukocytes. Perinatal parameters and clinical parameters were also analyzed.
Results
Of the 261 infants born at <34 weeks gestation, 22.4% demonstrated eosinophilia at birth. The eosinophil percentage peaked in the fourth postnatal week at 7.5%. The incidence of severe eosinophilia increased after birth up to the fourth postnatal week when 8.8% of all patients had severe eosinophilia. Severity of eosinophilia was positively correlated with a lower gestational age, birth weight, and Apgar score. Respiratory distress syndrome, bronchopulmonary dysplasia, nephrocalcinosis, intraventricular hemorrhage, and sepsis were associated with a higher eosinophil percentage. The eosinophil percentage was significantly higher in infants with bronchopulmonary dysplasia from the first postnatal week and the percentage was the highest in the fourth postnatal week, with the maximal difference being 4.1% (P<0.001).
Conclusion
Eosinophilia is common in premature infants and reaches peak incidence and severity in the fourth postnatal week. The eosinophil percentage was significantly higher in bronchopulmonary dysplasia patients from the first postnatal week. Severe eosinophilia was significantly associated with the incidence of bronchopulmonary dysplasia even after adjusting for other variables.
Introduction
Eosinophils normally account for 1%-3% of the peripheral blood leukocytes and primarily dwell in tissues1). Eosinophilia can be defined as an eosinophil count of more than 3% of the total leukocytes2). Eosinophilia is commonly found in neonates, particularly in premature infants and its incidence increases with immaturity3). Although the causes and pathogenesis of eosinophilia have not been clearly determined yet, many efforts are being made to investigate the conditions associated with eosinophilia, such as the maintenance of anabolic state, antigen exposure due to disease, infection, or parenteral nutrition4,5,6).
In particular, eosinophilia frequently occurs in premature infants with bronchopulmonary dysplasia (BPD). Previous studies have compared the higher eosinophil counts in the fourth week of life in BPD patient groups with those in groups without BPD7,8). The pathophysiology of BPD is multifactorial and needs further investigation; however inflammation remains an important characteristic of lung injury leading to BPD9).
Therefore, in this study, we investigated the clinical significance of eosinophilia in premature infants at less than 34 weeks' gestation by evaluating the incidence and severity of eosinophilia. Furthermore, we evaluated the association between eosinophilia and clinical conditions of the premature infants, such as gestational age (GA), birth weight, gender, and complications commonly seen in premature infants. In particular, the relationship between eosinophilia and BPD was thoroughly investigated.
Materials and methods
The medical records of premature infants at less than 34 weeks GA, who were admitted to the neonatal intensive care unit at Ewha Womans University Mokdong Hospital between January 2003 and September 2010, were analyzed retrospectively. Patients with congenital malformation, who had expired, or who were transferred within the first week of life were excluded. A total of 276 very low birth weight (VLBW) infants were admitted, and 261 VLBW infants were eligible.
A complete blood count with differential was checked weekly up to eight weeks of life. Eosinophilia was defined as the mean eosinophil percentage more than 3% of the total leukocytes2). Eosinophilia was further subclassified according to severity with the highest eosinophil percentage during the admission period; mild eosinophilia was 3%-10% of the total leukocytes, moderate eosinophilia was 10%-20%, and severe eosinophilia was more than 20%.
Perinatal data and clinical parameters of the patients, such as gender, GA, body weight at birth, Apgar score, and history of any complications-necrotizing enterocolitis (NEC), sepsis, respiratory distress syndrome (RDS), BPD, pulmonary hemorrhage, intraventricular hemorrhage (IVH), pneumothorax, and nephrocalcinosis-were analyzed retrospectively. The perinatal histories (e.g., use of antenatal steroids and magnesium, presence of gestational diabetes, pregnancy-induced hypertension, preterm rupture of membrane, vaginal infection, and chorioamnioitis) of the mothers were also analyzed retrospectively.
RDS was clinically diagnosed in premature infants with respiratory difficulties-tachypnea (>60 breaths/min), chest retractions, cyanosis etc.-and characteristic chest radiographic appearances (uniform reticulogranular pattern and peripheral air bronchograms). BPD was defined as persistent oxygen dependency until up to 28 days of life and the severity of BPD was graded according to the Jobe classification10). NEC was diagnosed and categorized into stages of disease progression based on Bell's staging11). The presence of IVH and nephrocalcinosis was diagnosed by brain and abdomen ultrasonography, respectively. The diagnosis of sepsis was based on positive blood culture results and clinical signs of infection (e.g., recurrent apnea, tachycardia and/or bradycardia, unstable body temperature.).
All the data were statistically analyzed using SAS ver. 9.1 (SAS Institue Inc., Cary, NC, USA). Continuous variables were compared among groups using the Kruskdal-Wallis test (two groups) and analysis of variance (ANOVA; more than two groups). Categorical variables were compared using the chi-square test and Fisher exact test. PROC MIXED (SAS Institue Inc., Cary, NC, USA) was used to evaluate the difference between the BPD and control groups' eosinophil percentages over time time. Logistic regression analysis was also conducted to evaluate the association of eosinophilia with BPD. A level of P <0.05 was considered statistically significant.
Results
1. Change in the eosinophil percentage after birth
The clinical data of 261 patients were analyzed during the study. The general characteristics of the patients enrolled in this study are shown in Table 1. The mean GA of the patients was 30.6 weeks (24.2-34.0 weeks), the mean birth weight was 1,550 g (460-2,760 g), and the mean initial leukocyte count was 11,870/µL (3,000-63,500/µL).
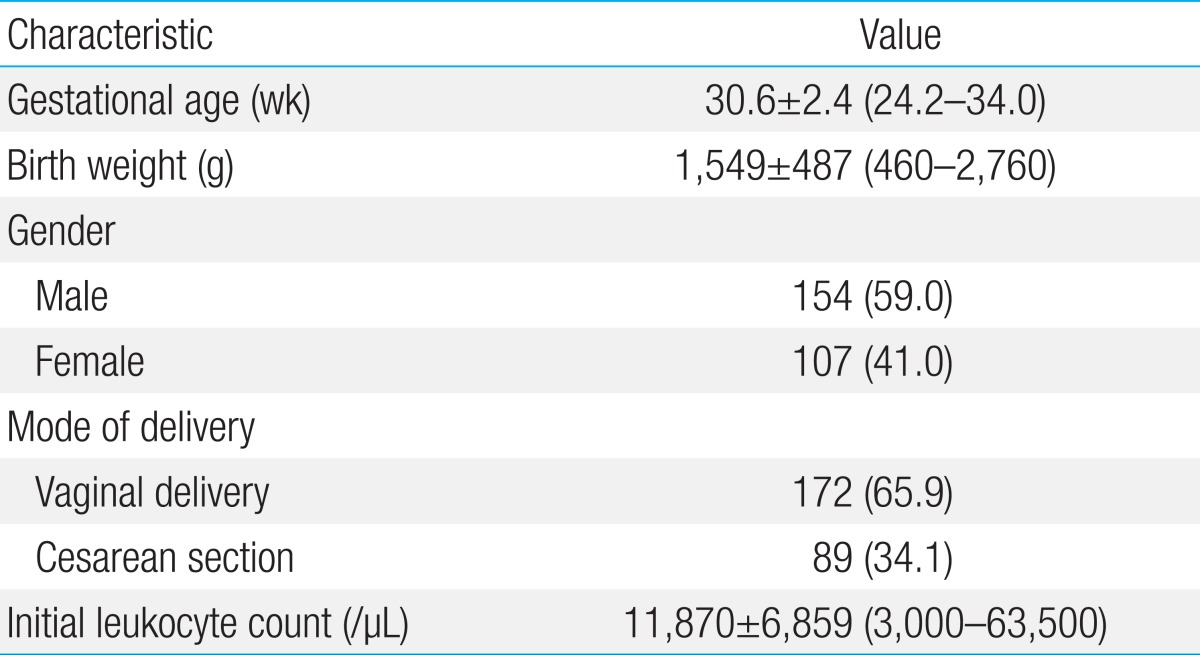
Patient characteristics (n=261)
The change in the eosinophil percentage at each postnatal age is plotted in Fig. 1. The eosinophil percentage was lowest at postnatal days 0-3 (1.4%), and began increasing at postnatal days 4-7. The eosinophil percentage reached its peak in the fourth postnatal week (7.5%) and subsequently began decreasing.(ANOVA, P<0.0001)
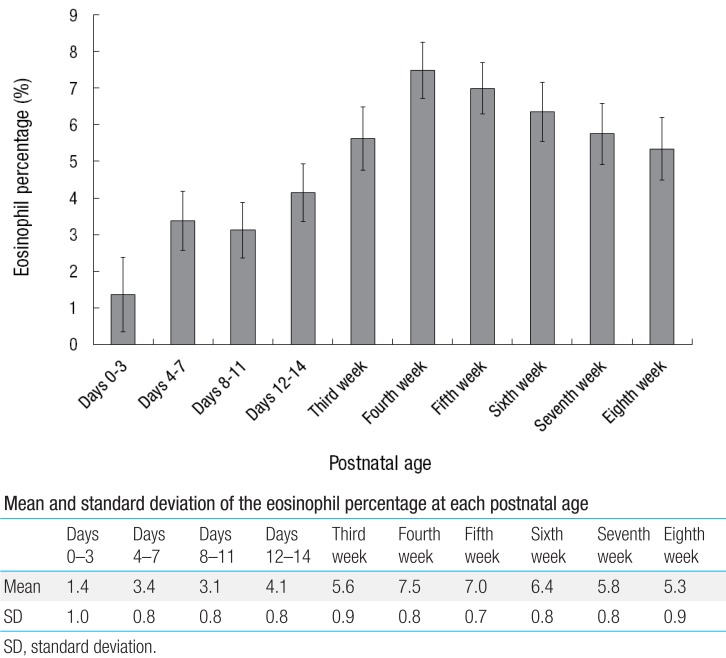
Changes in the mean eosinophil percentage at each postnatal age.
Further subgroup analysis of the severity of eosinophilia was also conducted. Fig. 2 presents the distribution of the subgroups of eosinophilia at each postnatal age. 22.4% of the infants demonstrated eosinophilia at birth. The incidence of eosinophilia increased after birth until it reached its peak in the fourth postnatal week (88.9%), and decreased gradually afterwards (ANOVA, P<0.0001).
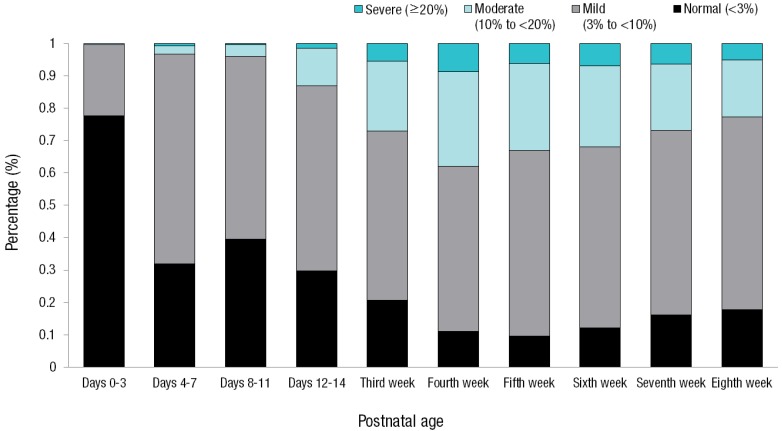
Eosinophilia severity distribution (%) by each postnatal age.
In total, 22.0% of the patients had mild eosinophilia (3%-10%), 0.4% had moderate eosinophilia (10%-20%), and none of the patients had severe eosinophilia (>20%) at birth. The differences between the distributions at each postnatal age were statistically significant (P <0.001). The incidence of eosinophilia began increasing at postnatal days 4-7 (68.2%), and most of the cases at that point of time were mild eosinophilia (64.9%). The distribution of moderate and severe eosinophilia began increasing at postnatal days 8-11 until it reached its peak in the fourth postnatal week (moderate eosinophilia, 29.2%; severe eosinophilia, 8.8%). The distribution then showed a tendency to decrease subsequently.
2. Eosinophilia and the patients' characteristics
The general and clinical characteristics of the patients were compared according to the severity of eosinophilia. Table 2 shows the relationship between the severity of eosinophilia and the general characteristics of the patients enrolled in this study. GA, body weight, and Apgar score at birth all had a statistically significant relationship with the severity of eosinophilia. Infants' gender had no significant relationship with the severity of eosinophilia.
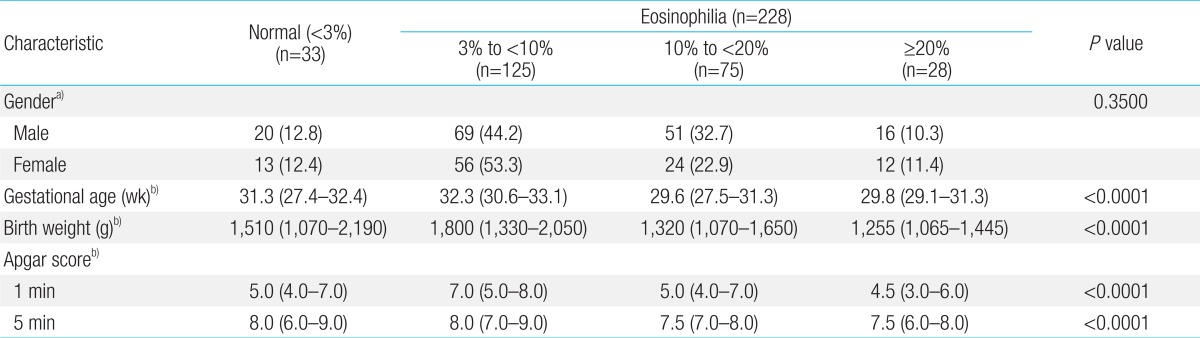
Severity of eosinophila by gender, gestational age, birth weight, and Apgar score
Table 3 shows the relationship between the severity of eosinophilia and the clinical characteristics of the patients. The presence of RDS, BPD, nephrocalcinosis, IVH, and sepsis was found to be significantly associated with higher eosinophil percentage. Retinopathy of prematurity, pulmonary hemorrhage, NEC, and pneumothorax showed no significant association with eosinophilia. Treatments such as total parenteral nutrition (TPN), antibiotics, blood transfusion, and ventilator treatment showed a significant association with eosinophilia (Kruskal-Wallis test, P<0.05).

Severity of eosinophilia and clinical characteristics of patients
3. Eosinophila and BPD
We further analyzed the correlation between eosinophilia and BPD in detail. Table 4 shows the sensitivity, specificity, positive predictive value and negative predictive value of the eosinophil percentage in predicting BPD in premature infants. Sensitivity was highest for postnatal days 8-11 (82.0%), and the area under the ROC curve was the largest in the third postnatal week (0.65).

Sensitivity and specificity of eosinophil counts in predicting bronchopulmonary dysplasia in premature infants
The change in the eosinophil percentage at each postnatal age from birth until the eighth week for the BPD and control (patients without BPD) groups are plotted in Fig. 3. In general, the eosinophil percentage of the BPD group was higher than that of the control group from the first week of life (postnatal days 4-7), and reached its maximal difference in the fourth week of life (4.1%) even after adjusting for GA and gender (P<0.001). As shown in Table 5, severe eosinophilia had a significant association with the incidence of BPD even after adjusting for other variables (P<0.01; odds ratio, 7.23; 95% confidence interval, 1.02-51.10). On the other hand, eosinophilia had no significant association with other complications such as sepsis, RDS, IVH, and nephrocalcinosis after adjusting for other variables (logistic regression, P>0.05).
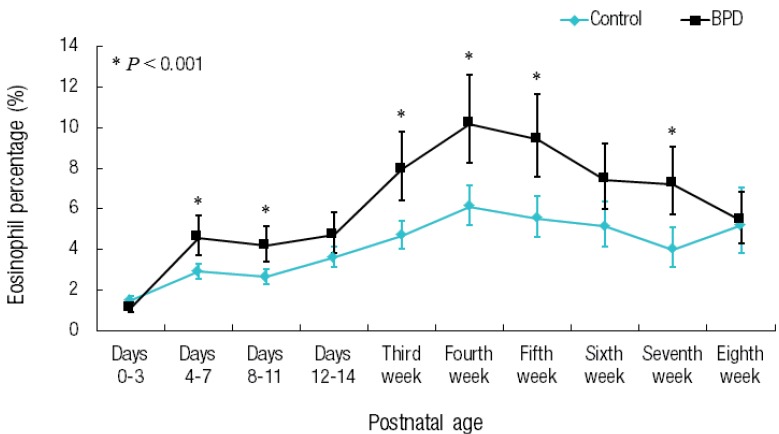
Changes in the eosinophil percentage at each postnatal age (from birth to 8 weeks after birth) in the bronchopulmonary and control groups. The eosinophil percentage was adjusted by gestational age and gender.
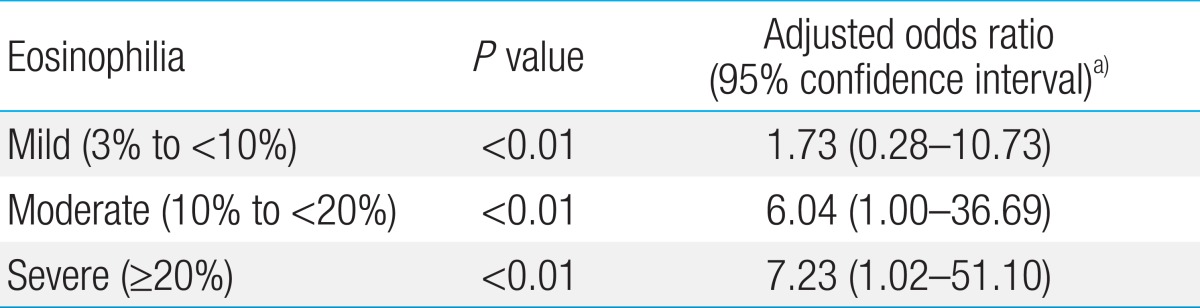
Association of eosinophilia with bronchopulmonary dysplasia using logistic regression analyses
Discussion
The eosinophil percentage begins to increase significantly at the first week of life in the BPD group compared with the control group (patients without BPD). The eosinophil percentage increases until it reaches its maximum value at the fourth postnatal week. The sensitivity of the eosinophil percentage in predicting BPD was highest for postnatal days 8-11.
Eosinophilia is particularly common in premature infants and increases with immaturity. In previous studies, the incidence of eosinophilia in premature infants and hospitalized term infants ranged from 14% to 76%3,7,8,12,13). Another recent study on eosinophilia among premature infants reported an incidence of 50 %14). In our study, the incidence of eosinophilia in premature infants at less than 34 weeks' gestation ranged from 22.4% to 88.9 % which was consistent with the results of previous studies.
The mean eosinophil percentage and distribution of subgroups according to the severity of eosinophilia were evaluated at each postnatal age. Both the mean eosinophil percentage (7.5%) and the distribution of severe eosinophilia (8.8%) were highest in the fourth postnatal week. This result is similar to the results of other studies where eosinophilia was most common at postnatal days 19-25 in premature infants15). Juul et al.3) also reported that eosinophilia in premature infants at less than 30 weeks' gestation reached its peak in the third postnatal week.
In premature infants, the incidence of eosinophilia increases with low GA and small birth weight4). This study further showed that low GA, body weight and 1- and 5-minute Apgar scores at birth had a statistical significant relationship with the severity of eosinophilia. Eosinophilia is also known to be related with to a family history of allergic diseases16). However, we could not collect our patients' detailed family histories of allergic diseases, which is a limitation of our study.
Eosinophilia in premature infants is reported to be associated with certain complications such as sepsis, RDS, BPD, and NEC3,17). The results of this study also showed that BPD, RDS, IVH, sepsis, and nephrocalcinosis were significantly associated with higher eosinophil percentages. TPN infusion, antibiotic treatment, blood transfusion, and ventilator treatment were also significantly associated with higher eosinophil percentages. Those treatments are known to contribute to changes in eosinophil levels in premature infants3,6,17). However, it was impossible to control all of these factors' individual contributions, which is another limitation of this retrospective study.
Our results also indicated that the eosinophil percentage was significantly higher in infants with BPD from the first week of life and reached its maximal difference from those without BDP in the fourth week of life. Moreover, a higher degree of eosinophilia was associated with the incidence of BPD even after adjusting for other factors related to BPD. In Yen et al.18)'s study, the eosinophil count in the first week of life was higher in infants with BPD, but it decreased from the second week of life and remained low until the sixth week. However, the eosinophil percentage of BPD infants in our study was steadily higher from the first week of life until the seventh week. Moreover, Yen et al.18) did not adjust for other factors such as GA and gender, but our study showed a significant difference, even after adjusting for them.
The results of the previous studies on the role of eosinophils in the pathogenesis of BPD are consistent with the results of this study. Eosinophil granules contain eosinophil cationic protein (ECP), eosinophil peroxidase, eosinophil-derived neurotoxin, and various cytokines and lipid mediators generated after cellular activation18). These products and cytokines may cause lung injury19). Raghavender and Smith12) showed that ECP levels in tracheal aspirates of 11 premature infants in whom BPD subsequently developed were higher during the first week of life (and continued to increase subsequently) than that of eight premature and eight term infants without BPD. Brostrom et al.7) reported that eosinophil counts and ECP levels were higher in BPD infants than those in RDS infants and healthy premature infants at the age of four weeks. They also demonstrated that eosinophils play a potential role in the pathogenesis of BPD and are activated in BPD infants by reporting increased ECP levels and decreased EG2 and CD9 levels in BPD patients7). However, many BPD patients receive steroid treatment to prevent or arrest the progress of BPD, and some studies have reported that the use of steroids is associated with a decreased eosinophil count7,12,20). This study did not consider the effects of steroid treatment on eosinophil count changes and this aspect would need to be investigated further.
The sensitivity of the eosinophil percentage in predicting BPD was significantly higher for postnatal days 4-7. However, the area under the receiver operating characteristic curve was smaller than 0.80 making it difficult to define the cutoff value, which is a limitation of this study.
The mean eosinophil percentage instead of eosinophil counts was used in this study. Nevertheless, the total eosinophil count and eosinophil percentage were strongly correlated with each other in reflecting changes in the eosinophil level according to the presence of BPD.
In conclusion, eosinophilia is common in premature infants and reaches its peak in the fourth week of life. The incidence of eosinophilia in our study was higher in infants with low GA, birth weight, and Apgar scores. Infants with RDS, BPD, IVH, nephrocalcinosis, and sepsis were also significantly associated with higher eosinophil percentages. In particular, the eosinophil percentage was significantly higher in BPD patients from the first week of life. Moreover, severe eosinophilia had a significant association with the incidence of BPD even after adjusting for other variables.
Notes
No potential conflict of interest relevant to this article was reported.