Single-center experience of the Korean-Developmental Screening Test for infants and children
Article information
Abstract
Purpose
We investigated the number of test takers of the Korean-Developmental Screening Test (K-DST) in a single children's hospital within a year, according to age, referral rate, and follow-up percentage.
Methods
For this study, 4,062 children who visited and received K-DST at Woorisoa Children's Hospital between January and December 2015 were enrolled. Seven test sets were used according to the Korean National Health Screening Program for infants and children in the following age groups: 4 to 6, 9 to 12, 18 to 24, 30 to 36, 42 to 48, 54 to 60, and 66 to 71 months. The results of the K-DST were categorized into 4 groups as follows: further evaluation (<−2 standard deviation [−2SD]), follow-up test (−2SD to −1SD), peer level (−1SD to 1SD), and high level (>1SD).
Results
The test participants' population and follow-up population were concentrated before the age of 24 months (2,532, 62.3%). The children most commonly referred for further evaluation were those in the 30- to 41-month age group. A mismatch was found between the results of the K-DST and the additional questions. Most of the infants and children with suspicious developmental delays showed catch-up development in their follow-up tests (43 of 55, 78.2%).
Conclusion
The use of K-DST should be encouraged, especially among children aged over 24 months. Multiple-choice question format for the additional questions is recommended to avoid confusion. We suggest a nationwide study to evaluate and revise the K-DST.
Introduction
With an aging Korean society coupled with low-birth rate, the country realizes the importance of providing an environment that fosters healthy birth and development of children as well as facilitating the well-being of the people of the nation123456). The government also realizes that earlier detection of developmental delays among infants and children is critical for a better prognosis and earlier rehabilitation therapy2789). To achieve this purpose, the government has started a national health screening program for infants and children in Korea since 20072345). Korean-Ages and Stages Questionnaires (K-ASQ)10) and Denver Developmental Screening Test II (DDST II) were used for evaluating developmental status34). However, these 2 tests had certain specific problems such as unsuitable questions for Korean environments, limited age groups and test categories, no use for web version due to a copyright and low validity259111213).
Korean Developmental Screening Test (K-DST) for infants and children is a recent screening test designed to suit the needs of Korean infants and children214). The National health screening program has been using this test questionnaire since September 2014. As compared with the previous tests, K-DST has no test-skipped age; for national health screening program for infants and children (0-71 months old) and has compensated some inappropriate questions related to problem-solving and personal social section. Finally, all test results are stored and managed in the National Health Insurance Service web server, which allow parents and clinicians to look all serial data when needed15). The aim of this study is to evaluate the status of the K-DST in investigating data including the number of test takers by age groups, actual referral and follow-up percentage to check the usefulness of this test in primary clinics.
Materials and methods
1. Study populations
All infants and children visiting the Woorisoa Children's Hospital for the National Health Screening Test from January to December 2015 were included in the study.
2. Study design
The National Health Screening Tests are conducted on infants and children in Korea who visited the clinic a total 7 times, that is, when they turn 4–6, 9–12, 18–24, 30–36, 42–48, 54–60, and 66–71 months of age. The K-DST questionnaire sets are administered at intervals of two months from 4–5 to 22–23 months, 3 months from 24–26 to 33–35 months, and 6 months from 36–41 to 66–71 months15). The participants take the test papers according to their corrected age at the time of their clinic visit. We did not conduct K-DST to 4–6 months of age group infants because of the current national health screening policy. The policy states that the first trial of K-DST starts from 9 months of corrected age7). They visited and received physical examinations and nutritional education only.
The K-DST has 6 sections and additional questions. Gross motor, fine motor, cognition, communication, social interaction, and self-control are the 6 sections. Additional questions are designed to take into account clinically important diseases, such as cerebral palsy, language delay, and autism spectrum disorders15). According to the K-DST manual, there are 4 categorized groups; the further evaluation, the follow-up test, the peer-level, and the high-level groups. Children who scored below −1 standard deviation (−1SD) are categorized as the follow-up test group, and they need short-term check-ups for re-evaluation. Children with a score between −1SD and 1SD are the peer-level group, and a group of children who scored above 1SD is the high-level group. The manual suggests that test participants with any positive additional questions should be referred for further evaluation15). According to the manual, we referred some cases of the further evaluation group or the follow-up test on K-DST results, or of the positive additional questions.
3. Statistics
We reviewed the chart retrospectively and described the quantitative data of the discrete variables as frequencies with percentile. We used the IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA) for data processing.
4. Ethnics statement
The study was approved by the Institutional Review Board of Korea University Guro Hospital (approval number: KUGH16176-001).
Results
1. Study population
Total sample cases were 4,062 out of which 2,081 (51.2%) were male and 1,981 (48.8%) were female (Table 1). The sex distributions were almost similar in each group. The numbers of each segmental group were approximately similar with the range of 200 to 400. The largest number of test group was the 18- to 24-month-old age group, 929 (22.9%). The number of test participants' increased until 118- to 24-month-old age group, and then declined. The total number of K-DST takers was 3,308, because 754 out of 4,062 cases were the members of 4- to 6-month-old group who did not take K-DST. Twenty children had been already in rehabilitation therapy.

Number of cases according to age and sex (n=4,062)
2. Follow-up cases
The total number of follow-up cases was 264 (Table 2). The 4- to 6-month-old age group had the largest follow-up cases, that is, a total of 196 cases (74.2%), followed by 10- to 11-month-old age group with 22 cases (8.3%). Most children took follow-up tests before the age of 22-23 months (225 cases, 85.2%). Among the follow-up cases, 3 people were receiving rehabilitation therapy.

Number of follow-up test takers in 1 year according to age group (n=264)
3. Results of K-DST
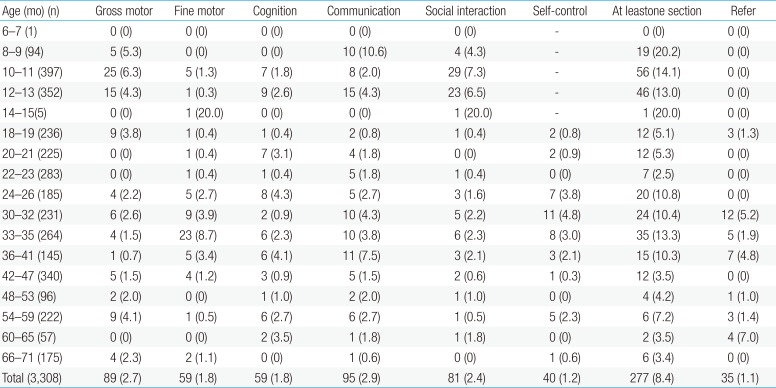
The percentage of each section according to the 4 developmental levels was similar. The percentages of each section of the “Further evaluation” group were around 2% in general (Table 3). The average percentage of the high developmental level was about 40%.

Results of the Korean-Development Screening Test for Infants and Children
4. The number of referrals
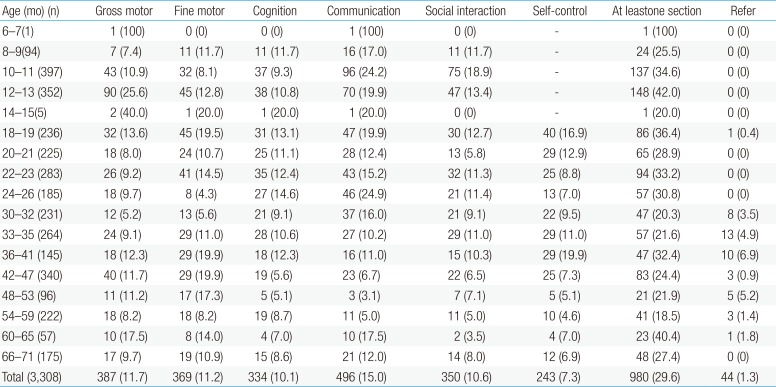
The distribution of further evaluation cases had 2 peak points, 10- to 11-month-old age group (56 cases) and 33- to 35-month-old age group (35 cases) (Table 4A). With respect to sections, communication section had the largest number of cases, 95 (2.9%), followed by gross motor section, 89 (2.7%). The distribution of follow-up test cases also had 2 peak points, 12-13 months (148 cases) and 42-47 months (83 cases) (Table 4B). The follow-up test group had the largest number of cases on communication, 496 (15.0%), followed by fine motor, 412 (12.5%). Total referral rates among positive cases in at least 1 section were 11% for further evaluation group and 4.5% for the follow-up test group. Both level of groups had no referral under the age of 18-19 months, and both groups had concentrated number of referral between the age of 30-32 months and 36-41 months. In the fine motor section of further evaluation level, 37 was the largest number of cases in this concentrated zone, followed by the communication section with 31 cases. Both communication and self-control sections of the follow-up test group had the largest population with 80 cases each.

Results of the “needs further evaluation” group

Results of the follow-up test group
5. Additional questions
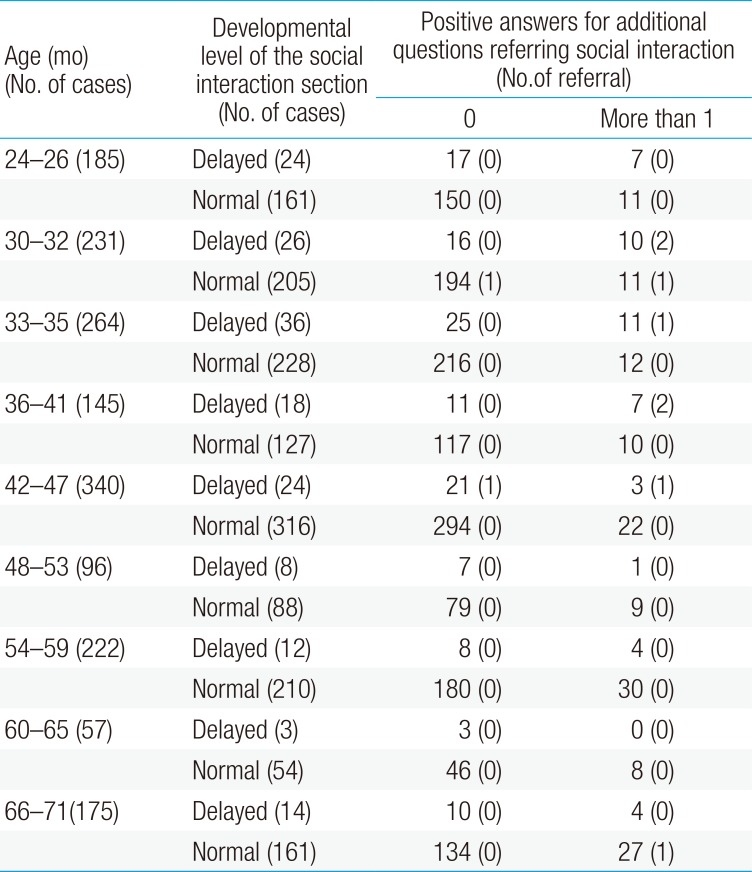
We compared the results between the social interaction section and questions regarding social interaction among the additional questions (Table 5). The number of cases with positive additional questions in the Below -1 SD (the further evaluation group and the follow-up test group) group was only 47 out of 165 cases (28.5%). Additionally, only 1 out of 140 cases, in the Above -1SD (the peer-level group and the high-level group) group with positive additional questions, was referred. Among all 187 cases with positive additional questions, 2 children were already in treatment.

Comparison of numbers between the social interaction levels and additional questions in the K-DST
6. K-DST results of follow-up cases
Among the total follow-up cases (Table 2), 197 cases had their first time visit in their 4- to 6-month-old age group. Only 67 cases had taken 2 serial tests. There were 16 cases in a “Above -1SD to Below -1SD” group, whose first K-DST results were Above -1SD but the following test results became Below -1SD (Fig. 1). The fine motor section had the largest case numbers (10) on “Above -1SD to Below -1SD” group. Not a single case was referred because all cases on their following study were the follow-up test levels. There were a total of 43 cases whose previous K-DST results indicated suspicious developmental delay and then scored higher in follow-up study. Communication section had the largest number of cases (12). Considering that one child scored below -1SD in multiple sections, total 38 out of 67 follow-up cases scored below -1SD on at least one of the K-DST sections. A more in-depth analysis of each section revealed that 3 children on gross motor were diagnosed as suspicious delayed group on the second test, and their scores were between -2SD and -1SD in the follow-up test group. Ten children were diagnosed as suspicious delayed group, and their scores were between -2SD and -1SD. Only three cases of the further evaluation level in both serial tests were sent to special clinics.
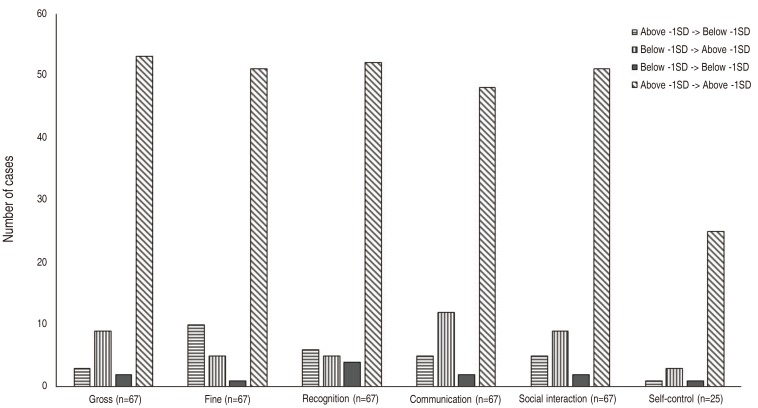
Follow-up data of the K-DST scores. The numbers of infants and children show that the follow-up results were different, either normalized or newly screened as delayed, from the previous results. n, number of cases; K-DST, Korean-Development Screening Test for Infants and Children; Below -1SD: the further evaluation group + the follow-up test group, Above -1SD: the peer-level + the high-level.
Discussion
With growing realization of the importance to invest in people's welfare and a conducive environment for nurturing children, the Korean government is increasingly putting emphasis on developmental delay prevention and life-long health care1345). Some of the developmental delays could catch up to an almost normal status with early rehabilitation programs36789). Early detection of developmental delay needs comprehensive judgements of medical history, developmental status evaluation, physical and neurological examination along with a developmental screening test346789). The developmental screening test is especially very important in early diagnosis of developmental delay3678915). The Korean government launched the Korea National Health Screening Program for Infants and Children on November 20071234591415). Since then, every infants and children visits the primary clinic and receives serial developmental screening tests from 4 months to 71 months of age, at least before starting with elementary school1234915).
The original screening tools were K-ASQ and DDST II. K-ASQ is a modified version of Ages and Stage Questionnaires-II designed in America and is more convenient than DDST II; therefore, most clinicians used K-ASQ as a screening tool35915). However, this tool could not exactly reflect Korean culture and infant care environments. Also, several questions related to problem-solving and personal-social sections were inappropriate3). The same questions were included in questionnaires in different age groups5). This caused a high false-negative rate, especially in the 60-month-old age group9). Therefore, the difficulty levels of some questionswere not suitable for suspicious developmental delay detection59). This strongly indicated the modification of questionnaires. The last test age was 60 months and children had a 1-year gap before entering elementary schools9). To compensate the insufficiency, a new screening tool, K-DST was designed in 2014, and this tool was suitable for Korean infants and children123914).
The study population by aging group, over 800 cases took the test in aging groups from 4-6 to 118- to 24-month-old age groups. The study participation rate started to drop from 30- to 36-month-old age group. According to the national statistic data between 2012 and 2014, the participation of the screening test started dropped from 42- to 48-month-old group (71.2%)16). This drop rate of the test participant number seems to be related to the referral rate since the first referred case appeared at the age of 18 months. Many referred cases seemed to stay at the tertiary hospitals for follow-ups.
Children usually catch up with the peer level as time goes by. Therefore, the follow-up data is very important for evaluation of their precise developmental status. Most cases of delayed group scored higher on their follow-up tests (Fig. 1). All cases of “normal to delayed” group on their follow-up study were the follow-up test levels.
In the additional question section, the screening test questions related to cerebral palsy, language delay, and autism spectrum disorders were very important and the clinicians needed to pay attention to the answers of the questions15). We found that the actual referral rate was low (3.7%) in positive additional questions, although, the manual suggested to refer all positive additional question cases for further evaluation despite normal K-DST level. Twenty cases among delayed group were already receiving rehabilitation therapy, and this could be one of the reasons for the low referral rate. Another reason could be the answer choices. Parents could answer the questions only in a “yes or no.” Therefore, the parents would answer a “yes” if their child performed the action once or twice. This could be the reason for high positive rate for the “peer” and “high-level” groups.Therefore, multiple choices for the additional questions are necessary to improve the accuracy.
The limitation of our study was inability to evaluate the referral cases against the final results. This may be correlated with the low revisiting rate of referred cases (3 of 31, 9.7%). The parents of the referral cases choose tertiary hospital for their children's evaluation. The primary clinician could only know the results of the further evaluation tests only when their parents notified directly. This inaccessibility would get solved with the extended web service to feed information about the test results.
When children between 4 to 6 months of age visited the primary clinic for the first time, they only received physical examination and nutrition and health education. This is because the government had previously decided the first K-DST stage as nine to twelve months in chronological age, whereas the K-DST actually uses corrected age. Therefore, any 9-month-old preterm birth infants were required to take the test questionnaire that was meant for 4- to 5-month-old infants or 6- to 7-month-old infants. Since preterm infants visit preterm clinics in a tertiary hospital regularly, many primary clinics do not need to see the questionnaires. The clinicians can use the questionnaires for 4 to 5 and 6 to 7 months age for evaluation of full-term infants under 8 months old with suspicious developmental delay. For earlier detection of developmental delay, we should expand the national developmental screening program to younger infants and children.
In conclusion, we should encourage the use of K-DST, especially among children who are more than 24 months old. Multiple-choice question formats for the additional questions are recommended to avoid confusion. We suggest a nation-wide study to evaluate and revise the K-DST.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.