Sleep problems in children and adolescents at pediatric clinics
Article information
Abstract
Purpose
To investigate the frequency of childhood sleep problems at pediatric clinics in Seoul and Gyeonggi provinces.
Methods
Children (n=936) and their parents who visited 5 primary and 1 secondary pediatric outpatient clinics were invited to complete a Pediatric Sleep Questionnaire.
Results
Among patients, 901 (96.3%) answered questionnaires in sufficient detail for evaluation. The participant's mean age was 4.35±3.02 years (range, 0–18 years). The male to female ratio was 1:0.93 (466 boys, 435 girls). Habitual snoring (>3 day/week) was reported in 16.9% of the participants. The prevalence of habitual snoring in children <2 years and those between 2–5 years was 9% and 18%, respectively. Sleep disordered breathing was found in 15.1% (106 of 700) of children >2 years. Insomnia was reported in 13.2% of children. The prevalence of sleepwalking, night terrors, and bruxism, is 1.6%, 19%, and 21.1%, respectively. Snoring was associated with increased incidence of sleepwalking, night terrors, and bruxism. Age was associated with insomnia and habitual snoring (P<0.05). Insomnia was more prevalent in younger (21%) than in older children (6%). Snoring was more frequent in both preschool (34%) and school-aged children (33%). The frequency of sleep disordered breathing and insomnia did not vary significantly with gender. However, snoring was more prevalent in boys.
Conclusion
Sleep problems are frequent among children in Korea. Children with snoring have an increased risk of sleepwalking, night terror, and bruxism. Primary clinicians should consider children's sleep habits to improve their health.
Introduction
Although the biological function of sleep is still largely unknown, sleep is seen as an important part of the healing process and is considered essential to life in the physical, neurological, and emotional areas. There are short- and long-term effects on life in sleep deprivation. The short-term effects include poor attention and concentration, reduced quality of life, low productivity and an increased absence in class or work, while long-term effects include higher morbidity and mortality due to car accidents, coronary artery disease, heart failure, hypertension, obesity, type-2 diabetes, stroke, depression, memory loss, and decreased immune function1).
Sleep problems in children and adolescents cause serious conditions, medically and psychologically2). Severe sleep breathing disorders may lead to left ventricular hypertrophy, arrhythmia, cardiac pulmonary syndrome, heart failure, growth failure, and death345). Sleep apnea and other sleep disorders can lead to depression, attention deficit and hyperactivity disorder, cognitive disorders, learning disabilities, and emotional instability678).
According to a recent study, the prevalence of sleep-related diseases in children and adolescents was determined to be approximately 43%, the rate of insomnia was determined to be 5%–20%, the rate of obstructive sleep apnea was determined to be 1%–3%, the frequency of snoring was determined to be 5%–27%, and the rate of parasomnias was determined to be 14%–37%9). In Korea, snoring, bruxism, and enuresis have been reported to occur in 16.5%–26.7%, 13.2%, and 8.7%, respectively101112).
Despite the high incidence and considerable impact of sleep problems in the lives of children and adolescents, sleep problems are not of major concern among parents and doctors. Furthermore, there are only a few studies regarding the prevalence of sleep disorders in Korea101112).
In this study, we used the Pediatric Sleep Questionnaire (PSQ) to examine the prevalence of sleep disorders in Korean children and adolescents (Appendix). The PSQ focused on snoring and sleep disordered breathing (SDB). This questionnaire was employed to overcome the practical difficulties in asking patients about sleep problems in an outpatient setting21314).
Materials and methods
1. Study participant
The PSQ was explained to and completed by 936 patients and caregivers who visited a pediatric outpatient clinic of a secondary hospital or one of 5 private pediatric clinics around the Seoul and Gyeonggi areas from July to October of 2009.
2. Method
1) Questionnaire
The PSQ, which contains 31 questions, was translated and used. Questions 1–23 are composed of items related to snoring, SDB, daytime sleepiness, and daytime behavior problems. These questions consisted of items that were proven to be valid by conducting surveys on patients with sleep breathing disorders with an apnea-hypopnea index (Apnea Hypopnea Index) of 5 or greater in polysomnography studies. With the appropriate SDB value being 0.33, SDB can be diagnosed in cases where at least 8 of the 23 questions were answered “yes.” The sensitivity was 0.81 and the specificity was 0.87 when diagnosing SDB using the questionnaire. Among those in the validation study, 85% of patients diagnosed using polysomnography were diagnosed with SDB213). Notably, the Korean version of the PSQ used in this study was not validated.
Other questions related to sleepwalking (question 24), night terrors (question 25), bruxism (question 26), and insomnia (questions 27-31).
2) Diagnosis
If a patient answered with yes to more than eight of questions 1–23, then they were classified as SDB. Similarly, an answer of “yes” to questions 24, 25, 26, or 2 of questions 27–31 were indicative of sleepwalking, night terrors, bruxism, or insomnia, respectively. Snoring for more than 3 days a week (2 questions) was classified as habitual snoring2).
In the PSQ, SDB has been validated in children older than 2 years old. Therefore, in this study, SDB was diagnosed in children older than 2 years of age, as defined in the study by Chervin et al.13).
Furthermore, enuresis was analyzed only in ages over 5 years, depending on the definition.
3) Prevalence and risk factors
Based on the information given in response to the questionnaire, the incidence of night terrors, bruxism, SDB, and insomnia were examined. Due to the difference in sleep patterns of children and adults and the variations by age, sleep patterns that were studied were divided into 4 age groups: 0–1, 2–5, 6–12, and 13–18 years of age.
In adults, there is a clear difference between the sexes in the incidence of snoring. We studied whether this is also the case in children and whether sex differences are present in the prevalence of other sleep problems, such as sleepwalking, night terrors, bruxism, SDB, and insomnia.
Obesity, a known risk factor of SDB, was also closely examined in this study. Lastly, we analyzed the interconnections of each disease.
4) Statistics
Statistical analysis was performed using IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA). Associations were analyzed using a chi-square test and logistic regression analysis. P values less than 0.05 were considered significant.
Results
1. Characteristics of participants
Of the 936 survey participants, 901 were analyzed. The mean age (standard deviation, SD) was 4.35±3.02, and the ratio of male to female participants was 1:0.93 (466 male, 435 female). The 35 excluded surveys included questionnaires without responses or a lack of basic information, such as sex or age.
Among 901 survey participants were 201 infants (0–1 year old), 477 preschool children (2–5 years old), 206 school-age children (6–12 years old) and 17 adolescents (13–18 years old). Six hundred two surveys were completed by children and guardians who used primary hospitals and 299 surveys were completed by children and guardians who used secondary hospital. There were younger subjects in the primary hospitals; however, there were no sex differences (Table 1).

Demographic variables according to age group
2. Prevalence
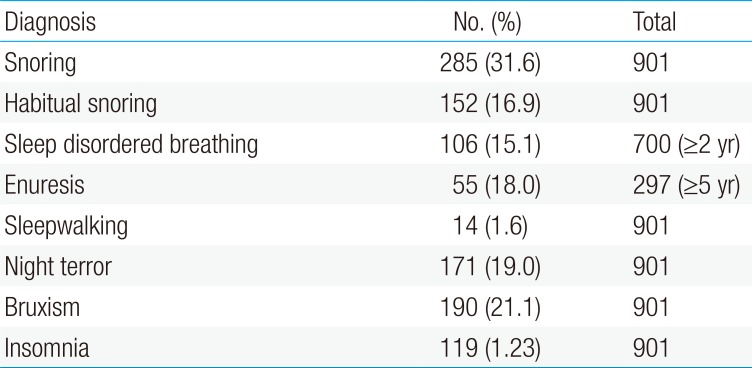
Among study subjects, the rate of SDB and insomnia was 15.1 % (106 patients) and 13.2% (119 patients), respectively (Table 2).

Prevalence of sleep disorders by Korean version of Pediatric Sleep Questionnaire survey
The rate of snoring, habitual snoring (snoring more than 3 days a week), sleepwalking, night terrors, bruxism, and enuresis among children was 31.6% (285 patients), 16.9% (152 patients), 1.6% (14 patients), 19% (171 patients), 21.1% (190 patients), and 18% (55 patients), respectively.
3. Risk factors
1) Age
There were statistically significant differences of age in the incidence of insomnia, habitual snoring, night terrors, and bruxism (Table 3). The incidence of insomnia was higher in younger children.

Prevalence of sleep problems according to age
2) Sex
SDB and insomnia had no correlations with sex (P=0.44 and P=0.88, respectively). In addition, there was no significant difference in the relationship between sleepwalking, night terrors, and bruxism (Table 4). The frequency of snoring was higher in boys (P=0.01); however, there was no difference due to sex in habitual snoring.

Rates of sleep problems according to sex
3) Health care system
There was no difference in the incidence of snoring, SDB, and insomnia between the primary and secondary hospitals (Table 5).

Prevalence of sleep problems between the primary and secondary health care system
4) Obesity
Among children, 12.0% (108 patients) were obese. Among these obese patients, 42.6% (46 of 108 patients) snored, which was greater than the rate of snoring among nonobese patients (30.4% [239 of 785 patients], P=0.01). Likewise, obese patients showed a significantly higher incidence of SDB (26.9%, 21 of 78 patients) than did those patients who were not obese (17.0%, 106 of 621 patients) (P=0.00).
5) Correlations of snoring and other sleep problems
There was a significant difference in the rate of bruxism, night terror, and SDB between the 3 groups of snoring (habitual snoring, snoring occasionally, and nonsnoring). However, there were no significant differences in the frequency of enuresis and insomnia (Table 6).

The coexistence of sleep problems according to snoring frequency
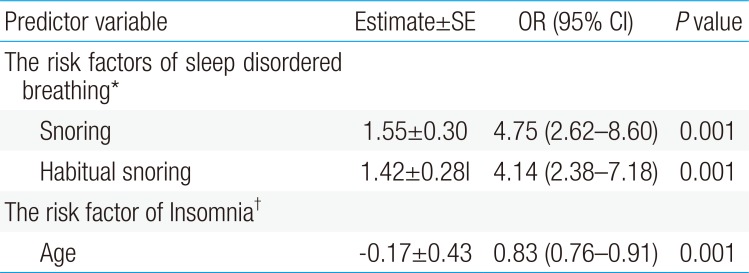
Logistic regression analysis showed a high incidence of SDB in snoring patients (Table 7).

Regression analysis of risk factors of sleep disordered breathing and insomnia
6) SDB and insomnia
Children diagnosed with SDB had a higher probability of insomnia than did those without SDB (P=0.00) (Table 7).
Discussion
This research investigated the frequency of sleep-related problems by surveying 936 patients under the age of 18, who had visited 1 of 6 different pediatric hospitals in the Seoul and Gyeonggi area. Results indicated that, among the patients, 13.2% had insomnia, 15.1% had sleep-related breathing disorders and 31.6% snored, of which 16.9% snored regularly (i.e., more than 3 times a week). In addition, other sleep related disorders, such as sleep walking, sleep terror, bruxism and enuresis, were also frequent, occurring in 1.6%, 19%, 21.1%, and 18% of subjects, respectively. Of the 5 relevant survey questions about insomnia, 13.2% replied “yes” to more than 2 questions, and a high rate (29.2%) replied “yes” to more than 1 question.
Archbold et al.2) reported that 18% replied “yes” to more than two questions and 41.4% said “yes” to more than one question in a similar survey. Furthermore, Lozoff et al.15) stated that the frequency of sleeping disorders in children was 31%. These studies, like this study, choose the study subjects and used surveys completed by children and parents who visited hospitals but did not have chronic illnesses.
The frequency of behavioral insomnia in children, including insomnia and night walking, was between 20% and 30% in early childhood, 15% in school-age children1617) and the prevalence of insomnia in adolescents between 16 and 18 years old was approximately 11%18). As in previous studies, we can see that the prevalence of behavioral insomnia is high in infants.
Childhood insomnia can be classified as either behavioral insomnia or psychological-physiological insomnia. Behavioral insomnia is usually more frequent in younger children, and psychological-physiological insomnia is more common among older children and adolescents1419). Since the survey used in this study investigates the presence of behavioral insomnia, it is presumed that the prevalence of insomnia was higher in younger patients. Furthermore, younger children often sleep together with their parents so their parents would have more easily observed symptoms related to insomnia.
Sleep-related breathing disorders are conditions that present problems in breathing during sleep and are caused by increased resistance in the upper respiratory tract. This includes snoring, upper airway resistance syndrome and obstructive sleep apnea.
Adenotonsillar hypertrophy is the most common cause of SDB in children and tends to occur in nasal obstruction (e.g., rhinitis, sinusitis, nasal septum deviation). Other risk factors include obesity, gastroesophageal reflux disorder, laryngomalacia, central facial hypoplasia syndrome (e.g., Pierre Robin sequence, Treacher Collins, Crouzon syndrome), lingual hypertrophy (e.g., 21 trisomy, Beckwith Wiedeman syndrome), and neuromuscular diseases2021).
There are a few major differences in SDB between children and adults. In children, the symptoms are more diverse and difficult to diagnose individually. In addition, excessive daytime sleepiness is common in adults while it is only seen in approximately 7% of children22). Conversely, hyperactivity is commonly seen among children. Lastly, symptoms of SDB vary in children depending on their age. In young cases, snoring, apnea, frequent arousal, sweating, dry mouth, and stunted growth are frequently seen. In contrast, cases in older patients frequently included symptoms of night terrors, sleep-talking, sleep-walking, enuresis, hyperactivity, and depression23). SDB can be diagnosed on the basis of patient history, physical examination, and polysomnography24).
In this study, the prevalence of snoring was 31.6%, of which habitual snoring (more than 3 days per week) was 16.9%. Preschool children (39%) and school age children (34%) showed a higher rate of snoring than did the other age groups. A previous study done in Korea by Cho et al.11) indicated that 15.5% of children snore at least once a week and 4.3% of children snore almost every day. In another study which investigated elementary school children10), 26.7% children were observed to snore and 7.1% of children snored more than 3 days a week. These 2 studies1011), which showed lower resulting numbers than does the current study, differed from this study in the recruitment of research subjects. The 2 studies gathered research subjects from elementary schools, whereas this study recruited outpatients. The diseases that the outpatients may have had at the time (e.g., upper respiratory infection, sinusitis, rhinitis, tonsillitis, etc.) could have had an influence on snoring, thereby increasing the frequencies shown in the study. In addition, since the subjects were children who visited hospitals, results might have shown higher snoring rates than an average child of similar age.
Particularly notable in this study was the frequency of habitual snoring in children younger than 24 months (9%) and in children between ages 2–5 (18%). Furthermore, this study is the first in our country to document the frequency of snoring in young children. Recently, it was shown that 60% of facial bones develop in children during the first 4 years of life25). Animal studies have shown changes in facial structure after induced nasal congestion26), and persistency of SDB with long-term follow-up27) suggest that persistent oral breathing caused by factors such as nasal congestion may structurally cause chronic development of SDB. This in turn highlights the necessity for early treatment during infancy and early childhood. Early detection and treatment of snoring and oral breathing may prevent the development of sleep apnea. However, the nature of this period has not yet been explored in our country. It can be said that the high incidence of 9%–18% shown in this study expresses the need for a more active diagnosis and treatment by pediatricians.
Research outside of Korea has demonstrated no difference in snoring between the sexes. However, this study showed a significantly higher incidence of snoring in boys. This was also the case in the two other studies1011) that were conducted in Korea. More research should be conducted to see if it this is due to unique characteristics of children in Korea.
Snoring children showed a significantly higher incidence of SDB, night terrors, and bruxism (Table 6). Logistic regression analysis showed the risk of SDB to be 4 times higher in children with habitual snoring (Table 7). Snoring is one aspect of SDB and the correlations between SDB and night terrors or bruxism has been demonstrated in previous studies2829). Parasomnia is regarded as a symptom of SDB in children, which is supported by the observation that treating SDB also relieves parasomnia and by its higher incidence in children who have a family history of SDB29). Therefore, in children with night terror or bruxism, it is recommended to primarily determine whether SDB is present and to treat it first.
In general, the prevalence of enuresis is higher in cases of snoring. The relationship between enuresis and snoring is believed to be due to an increase in plasma brain natriuretic peptide and a decrease in antidiuretic hormone concentration during sleep in SDB, thereby causing increased urine production, which is then aggravated by increased abdominal pressure due to the strong respiratory effort exerted by patients with SDB. Together, these events lead to urination.
However, in this study of the frequency of enuresis in ages greater than 5, there was no significant difference in its incidence across the 23% (14 of 60) of patients with habitual snoring, the 15% (8 of 52) of patients with occasional snoring, and the 17% (33 of 191) of patients who do not snore. Even when compared to habitual snoring and otherwise, the prevalence of enuresis showed no significant difference. The different results from existing studies is thought to be due to the simplistic classification of patients by their “yes” answer to the Korean version of question “Does your child wet the bed?” This level of detail is not sufficient to indicate enuresis, which requires that patients wet the bed at least twice a week for at least 3 months in children ages 5 or more and many parents misunderstood the questionnaire.
The risk factors of habitual snoring are similar to those of SDB. In a study targeting elementary school children in China30), risk factors, such as low family income, lack of higher education in the father, breastfeeding for less than 6 months, smoking during pregnancy, obesity, overweight, respiratory problems (rhinitis, asthma, adenoids hypertrophy, chronic otitis media), and a family history of habitual snoring were investigated. In this study, however, such risks were not examined.
The prevalence of night terrors was 19% and showed a significant difference by age. Night terrors occurred in 27% of infants aged 0–1 years old and in 19% of preschool children. In a study of twins, similar results to this study were obtained. A higher incidence of night terrors was observed in younger children, with a prevalence of 36.9% in children 18 months old and 19.7% in children 30 months old31). However, night terrors usually occur in ages 2–4 years and are known to appear in 6% of children, regardless of sex. The reason this study resulted in a high prevalence of night terrors is because all patients that answered “yes” to the question asking “awake in a panic or frightened” were classified as having night terrors, even though this question includes children who have either awaken while crying and those experiencing nightmares. This is a limitation of the survey since the patients may not have fully understood the meaning of night terrors.
Although there are many sleep-related problems in children and adolescents, parents and medical staff do not provide sufficient attention to this problem.
Meltzer et al.9) reported that the prevalence of sleep problems according to the ICD-9 (International Classification of Diseases, 9th revision) is 3.7%, which was lower than the results of previous studies. Low prevalence is thought to be a result of the study having been conducted retrospectively based on medical records. Given the lack of interest in sleep problems, most issues relevant to our study were not recorded.
The lack of interest in addressing sleep problems has been studied in previous research32) that indicated that while 24.6% of patients suffer from sleep problems, only 4.1% of parents discussed the problems and only 7.9% of parents consulted a doctor.
Other causes of sleep problems that were not covered in this study, include family suffering from illness or accidents, sleeping with a parent, the absence of the mother during the day, depression of the mother, and maternal ambivalence toward their children. Nevertheless, a previous study had shown that sex, age, birth order, family size, breastfeeding, parental education, occupation, paternal presence15).
Furthermore, children waking up in a panic were shown to have more stress in the family and the mothers exhibited more psychiatric disorders33).
In another study, the prevalence of sleep problems was higher in children of low income families and in infants younger than 1 year of age with a head circumference less than 2SD, in children older than 1 year of age with a body mass index greater than 2SD9).
There are some limitations to this study. A diagnosis using the PSQ does not replace the clinical diagnosis of an experienced physician. However, using a survey consisting of verified items associated with sleep problems has been shown to be similar to a physician in achieving a diagnosis. Despite this, diagnosing parasomnias in particular is nonspecific compared to the sensitivity of the survey because it is diagnosed using only 1 question. In addition, the subjects of the study do not represent all children and adolescents of our country. As the survey was completed by outpatients, and not by members of the public, the prevalence shown in the results may be higher than that of the community. Further research related to sleep problems using a representative sample group would be necessary.
Moreover, because the participants conducted the survey after having visited the hospital because of an illness, there is a possibility that the disease was affecting sleep and thus the answer was affected. Additionally, while socio-economic status which we did not asked in this study may have affected the sleep in children. Finally, the age of the subject may affect survey responses. Young children are mostly observed by the parents while sleeping, whereas older children who sleep alone may have had difficulties recognizing their sleep problems, which may have affected their answers to the survey.
Despite these limitations, this study is meaningful given the prevalence of SDB, insomnia, and snoring among Korean children and adolescents. Pediatric clinics of primary medical care centers report a relatively high prevalence of these conditions. Furthermore, our results show a higher incidence of snoring in infants with a higher frequency in boys. These snoring children had a four times higher risk of SDB.
Acknowledgment
This research received support from Dr. Hyeung Chae Kang of LeeKang Pediatric Clinic, Dr. Ki Tae Kim of Seoul Pediatric Clinic, Dr. Seung Nam Park of Park Seung Nam Pediatric Clinic, and Dr. Ki Dong Hwang of Hanmaeum Teunteun Pediatric Clinic.
Notes
Conflict of interest: No potential conflicts of interest relevant to this article was reported.
Appendices
Appendix
Pediatric Sleep Questionnaire
While sleeping does your child...
1. Snore more than half the time?
2. Snore over three days per a week?
3. Snore loudly?
4. Have loud breathing?
5. Have trouble or struggle with breathing?
Have you ever...
6. Seen your child stop breathing during the night?
Does your child...
7. Have restless sleep?
8. Tend to breathe through the mouth during sleep?
9. Tend to breathe through the mouth during the day?
10. Have a dry mouth upon waking up in the morning?
11. Occasionally wet the bed?
12. Wake up feeling un-refreshed in the morning?
13. Have a problem with sleepiness during the day?
14. Has a teacher or other supervisor comment that your child appears sleepy during the day?
15. Does your child wake up with headaches in the morning?
16. Did your child stop growing at a normal rate at any time since birth?
17. Is your child over weight?
This child often...
18. Does not seem to listen when spoken to directly.
19. Has difficulty organizing tasks.
20. Is easily distracted by extraneous stimuli.
21. Fidgets with hands or feet and squirms in their seat.
22. Is “on the go” or often acts as if “driven by a motor”.
23. Interrupts or intrudes on others (e.g., butts into conversations or games).
Does your child...
24. Walk in their sleep?
25. Awake in a panic or fright?
26. Grinds teeth during sleep?
27. Has difficulty in falling asleep during the night?
28. Wakes over two times during the night?
29. Has difficulty falling back to sleep after nighttime awakening?
30. Awake early in the morning and has difficulty falling back to sleep?
31. Resists going to bed?