Effects of cord blood vitamin D levels on the risk of neonatal sepsis in premature infants
Article information
Abstract
Purpose
Vitamin D plays a key role in immune function. Vitamin D deficiency may play a role in the pathogenesis of infections, and low levels of circulating vitamin D are strongly associated with infectious diseases. In this study, we aimed to evaluate the effects of low vitamin D levels in cord blood on neonatal sepsis in preterm infants.
Methods
One hundred seventeen premature infants with gestational age of <37 weeks were enrolled. In the present study, severe vitamin D deficiency (group 1) was defined as a 25-hydroxyvitamin D (25(OH)D) concentration <5 ng/mL; vitamin D insufficiency (group 2), 25(OH)D concentration ≥5 ng/mL and <15 ng/mL; and vitamin D sufficiency (group 3), 25(OH)D concentration ≥15 ng/mL.
Results
Sixty-three percent of the infants had deficient levels of cord blood vitamin D (group 1), 24% had insufficient levels (group 2), and 13% were found to have sufficient levels (group 3). The rate of neonatal sepsis was higher in group 2 than in groups 1 and 3.
Conclusion
There was no significant relationship between the cord blood vitamin D levels and the risk of neonatal sepsis in premature infants.
Introduction
Sepsis remains a major cause of neonatal mortality and morbidity in premature infants. These infants have an increased incidence of sepsis. There are many other reasons for sepsis not only premature rupture of membranes (PROM)1). The observations of the association between infections and vitamin D deficiency were first described more than a century ago2). Vitamin D plays a key role in immune function. Recent reports have supported a role for vitamin D in promoting normal function of the innate and adaptive immune systems2). Specifically, vitamin D and its receptor exhibit key anti-inflammatory, membrane-stabilizing and antimicrobial properties at barrier sites such as the gut, lung and skin. Vitamin D is very important for the innate immune system, leading to production of cathelicidins and defenses that have antimicrobial and antiendotoxin activities34).
Once microbes broke epidermal/mucosal barrier, they are recognized by pattern-recognition receptors such as Toll-like receptors (TLR). Cord blood low plasma concentrations of vitamin D were also found to correlate with diminished TLR induction of cathelicidin, which encodes for an antimicrobial peptide5). This peptide possesses microbiocidal activity against gram-positive (e.g., Staphylococcus aureus) and gram-negative (e.g., Escherichia coli) pathogens, common organisms responsible for invasive infections sepsis in neonates6).
Current studies investigate the relationship between cord blood vitamin D status and in vitro measures of human monocyte function. Cord blood vitamin D deficiency, by its effects on TLR-induced antimicrobial production, causes alteration in vitro monocyte responses4).
Cord blood vitamin D deficiency, by its impact on the TLR-induced antimicrobial production, altered in vitro monocyte responses4). Moreover, there is a majority of epidemiological evidence indicating that circulating vitamin D concentrations from cord blood correlate indirectly with increased susceptibility to infection in newborns7). This finding has led to the common hypothesis that vitamin D deficiency may play a role in the pathogenesis of infections8). There are a few studies which reported a link between vitamin D deficiency and neonatal sepsis in term infants9). With the results of the first study, it is shown that maternal and neonatal vitamin D is in relation with early-onset neonatal sepsis (EOS). The other study reported lower cord blood vitamin D levels in the mature babies with EOS. To the best of our knowledge, no study evaluated the association between neonatal sepsis and cord blood vitamin D levels in preterm infants910). Moreover, there is a preponderance of epidemiological evidence indicating that lower vitamin D concentrations from cord blood correlate with increased susceptibility to infections in newborns11). We sought to evaluate the effect of lower vitamin D levels in cord blood on neonatal sepsis in preterm infants.
Materials and methods
1. Study population
This case-control study was conducted in the Zekai Tahir Burak Maternity Teaching Hospital, Neonatal Intensive Care Unit (NICU) in Turkey. The data was prospectively collected during the period between 1 May 2013 and 31 September 2013. Study was approved by the local Ethics Committee and informed parental consent was obtained for all infants.
During the study period, a total of 117 premature infants with a gestational age of less than 37 weeks were enrolled. Exclusion criteria were as follows: Infants with maternal risk factors; such as clinical and/or histological chorioamnionitis and PROM, refusal of parental consent, lack of laboratory data and major congenital abnormalities.
Cord blood was collected by an experienced nurse who was not responsible for the primary care and possible resuscitation of the baby, in the delivery room, right after the delivery. The obtained 2-mL cord-blood was put into tubes containing Ethylenediaminetetraacetic acid (EDTA). Serums obtained by micropipettes were put into sterile plastic storage tubes and serums with hemolysis were excluded. Fresh serum samples protected from light were analyzed for vitamin D levels in the Biochemistry laboratory. The level of cord blood vitamin D was measured by using a direct competitive chemiluminescent immunoassay (Elecsys; Roche Diagnostics, Mannheim, Germany). The results were calculated as ng/mL.
All preterm infants' characteristics including gestational age, gender, birth weight, Apgar scores, route of delivery, use of antenatal steroids and probable maternal risk factors were recorded. Clinical examination and anthropometric measurements including weight, length, and head circumference of newborns were performed at birth.
The preterm infants were categorized according to their cord blood vitamin D levels.
According to this categorization; severe vitamin D deficiency (group 1) was defined as 25-hydroxyvitamin D (25-OHD) concentration <5 ng/mL; vitamin D insufficiency (group 2), 5 ng/mL <25-OHD concentration <15 ng/mL; and vitamin D sufficiency (group 3), 25-OHD concentration ≥15 ng/mL12).
2. Sepsis evaluation
The babies with suspected neonatal sepsis were observed in the NICU. All the babies were evaluated by Töllner scores (abnormal skin color, delayed cap refill, muscular hypotonia, bradycardia, apnea, respiratory distress, hepatomegaly, gastrointestinal symptoms, number of leukocyte, increased number of immature series, thrombocytopenia, metabolic acidosis) on the first day of diagnosis13). Leukocyte counts, immature: total neutrophil ratio (I/T-ratio), C-reactive protein (CRP) and Interleukin 6 (IL-6) values of the patients which were obtained during hospitalization were recorded. Timing of the control evaluations of the abnormal infection markers was decided according to the clinical situation of the patients.
Symptoms present at the admission, duration of hospitalization, prescribed antibiotics, duration of the antibiotherapy, need for continuous positive airway pressure or intubation, total duration of hospitalization and exact diagnosis were also recorded.
Those who had ≥10 points of Töllner score, a high level of IL-6 (≥20 pg/mL), I/T-ratio (>20%) on admission, and an increasing serial CRP level above normal (≥5 mg/L) were assigned to the study group.
Venous blood samples were put into tubes with EDTA (Vacuette tubes, Greiner Bio-One, Monroe, NC, USA). Complete blood counts were done by the automatic measurement devices with LH-780 system (Beckman Coulter Diagnostics, Image 8000, Brea, CA, USA). For the CRP analysis, 0.5 mL of blood from a peripheral vein was drawn into a commercial blood sample tube without any additives. Then, the CRP levels were measured on a Roche-Hitachi P800R (Roche Diagnostics, Indianapolis, IN, USA) using a CRP (Latex) HS AssayR kit (Roche Diagnostics). For the quantitative IL-6 analysis, 0.5 mL of venous blood was drawn into an EDTA-containing neonatal blood tube and analyzed using the ImmuliteR 1000 System (Siemens, Munich, Germany) using an ImmuliteR 1000 IL-6 kit (Siemens). Approximately 1 mL of blood samples for blood cultures are obtained by venipuncture after cleaning the skin with iodine-alcohol solutions and are cultivated in BACTEC (Peti-Bact Blood Culture, Organon Teknika Corp., Durham, NC, USA). The microorganisms are identified and disc diffusion method is used for the antibiogram.
EOS is described as sepsis diagnosed before the 7th day of life. Late-onset neonatal sepsis (LOS) is described as sepsis diagnosed between 7th–30th day of life14).
Using variables significant on univariate analyses, (gestational age at birth, birth weight, cord-blood vitamin D level) multivariable logistic regression analysis was done for determining the risk of EOS and LOS.
3. Statistics
Data were analyzed using SPSS ver. 16.0 (SPSS, Inc., Chicago, IL, USA). Descriptive statistics were given as mean±standard deviation for continuous data with normal distribution, median and interquartile range for continuous data with nonnormal distribution and frequencies and percentages for quantitative data. Differences between groups were evaluated using chi-square tests for qualitative data and t test for independent sample for continuous data with normal distribution and Mann-Whitney U test for continuous data with non normal distribution. Two-way analysis of variance was used to indicate interaction between season and group. Values of P<0.05 were considered statistically significant.
Results
During this study period, 117 preterm infants were assessed. Overall, 17 infants were excluded due to the previously declared reasons. The study population included a total of 100 (55 boys, 45 girls) preterm infants. Data regarding to the distribution group of the infants is shown in the flowchart (Fig. 1). Of these infants, 63% had cord 25-OHD levels ≤5 ng/mL (group 1), 24% had 25-OHD levels 5–15 ng/mL (group 2), 13% had 25-OHD levels >15 ng/mL (group 3). No significant difference was detected according to the maternal demographic features, anthropometric parameters and perinatal co-morbidities, basal characteristics of between all the groups (Table 1).
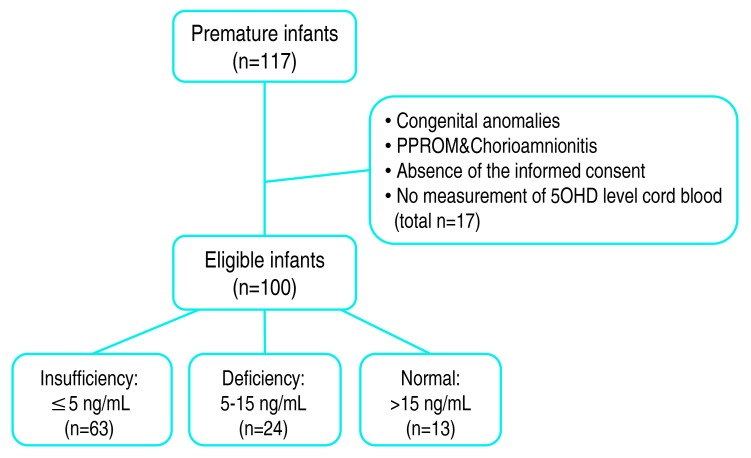
Data regarding to the distribution group of the infants is shown in the flowchart.

Basic demographic characteristics of the enrolled infants and pregnant women
The association between the cord vitamin D levels and neonatal sepsis rates were evaluated. Vitamin D levels were detected significantly lower in infants who were diagnosed as neonatal sepsis. In group 2, EOS and LOS rates were higher than groups 1 and 3 (Table 2). Both EOS and LOS rates were similar between groups 1 and 3.

Relationship between cord blood 25(OH)D levels and neonatal sepsis
The association between the presence of vitamin D deficiency and culture-proven sepsis was also evaluated. Two infants with EOS had positive blood cultures indicating gram-negative sepsis (E. coli, n=2) and 5 with LOS had positive blood cultures (Staphylococcus epidermidis n=2, Klebsiella n=2, Pseudomonas n=1). There were no significant difference between the cord blood vitamin D level and culture-proven sepsis. None of them had meningitis. None of the infants died during the study period.
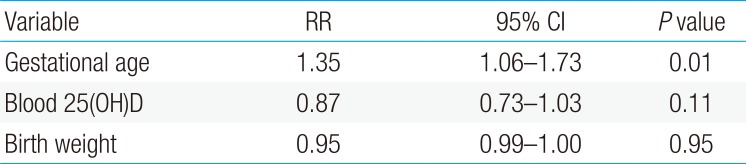
Using variables significant on univariate analyses, (gestational age at birth, birth weight, cord-blood vitamin D level) multivariable logistic regression analysis was done for determining the risk of EOS and LOS. Low cord-blood 25(OH)D levels as <5 ng/mL was not associated with the occurrence of both EOS and LOS in the model (relative risk [RR], 0.87; 95% confidence interval [CI], 0.73–1.03; P=0.11 and RR, 1.01; 95% CI, 0.86–1.19; P=0.84) (Tables 3, 4).

Multivariate analysis for early-onset neonatal sepsis

Multivariate analysis for late-onset neonatal sepsis
Discussion
The aim of our study was to better evaluate the effect of cord-blood vitamin D levels on sepsis, by excluding the babies with known risk factors for infection and who underwent resuscitation.
The observations of the association between infections and vitamin D deficiency were first described more than a century ago15). Today, it is well established that monocytes and macrophages possess 1-α hydroxylase and, the active metabolite of vitamin D can also be synthesized in the immune system2). This finding has led to the common hypothesis that vitamin D deficiency may play a role in the pathogenesis of infections, and low levels of circulating vitamin D have been shown to be strongly associated with infectious diseases816). Moreover, there is a preponderance of epidemiological evidence indicating circulating vitamin D concentrations from cord blood correlate. Only few studies in the literature, regarding to the relationship between neonatal vitamin D levels and early onset sepsis are present. Cetinkaya et al.10) has shown that, low maternal and neonatal vitamin D levels are related to EOS of the newborn. Cizmeci at al.91011), similarly, emphasized that the maternal and cord blood vitamin D levels are significantly low in the babies who have EOS.
We concluded that vitamin D deficiency detected via the blood taken from the umbilical cord may be related to increased rates of neonatal sepsis in preterm infants. With the results of our study, we showed that vitamin D insufficiency is not an independent risk factor for sepsis in premature infants.
Premature infants are extremely susceptible to infection, and sepsis is a significant cause of morbidity and mortality in this population114). They not only lack enough IgG type antibodies which pass transplasentally from the mother but also have immature immune system. Additionally, prenatal factors, delivery room management and resuscitation circumstances, delivery room and neonatology unit flora, number and quality of healthcare personnel, infection control methods used in the NICU and antibiotics used during sepsis are the main factors affecting sepsis incidence and mortality in premature infants1614). Because of this, it is not surprising that the results of our study did not show vitamin D level as an independent risk factor for neonatal sepsis.
This is mainly due to insufficient functioning of their skin as a barrier, low sensitivities against physiologic and pathologic signaling mechanisms, not enough passage of maternal IgG antibodies through the placenta, decreased opsonization and phagocytosis function due to low serum complement levels, immaturity of the neutrophilic migration ability, insufficient production of interferons and other proinflammatory cytokines, decreased intracellular oxidative response against opsonized bacteria and insufficient production of antibacterial factor by the polymorph nuclear leucocytes1718). Other risk factors are; urinary tract infection and bacterial vaginitis of the mother, multiple pregnancy, too many vaginal examinations during labor, long-term internal fetal monitorizations low Apgar scores and resuscitation. Even if the ratios of EOS and LOS were greater in the group with vitamin D levels <5 ng/mL, after performing logistic regression analysis for gestational age and birth weight, we determined that the vitamin D level was not an independent risk factor. But we propose that, more prospective studies regarding to the relationship of vitamin D and sepsis in premature infants are needed.
Preeclampsia has an incidence of 3% during pregnancy. Severe preeclampsia is found to be 5.4 fold more in the 15- to 20-week pregnant who have vitamin D levels <20 ng/mL19). But on the other hand, some studies did not find difference between the vitamin D levels and preeclampsia. The results of our study revealed no difference in the incidence of preeclampsia when the infants are grouped according to their cord-blood vitamin D levels.
Vitamin D levels are found to be significantly low in the pregnant women who have gestational diabetes and deterioration in glucose tolerance20). But with the results of our study, no relation between the cord-blood vitamin D levels and gestational diabetes incidence is found. The finding of a study as the low values of calcitriol in 22 women with cholestasis during pregnancy makes us think that the low values may be related to this morbidity21). In our study, no difference regarding to maternal cholestasis is found. Due to the absence of serum vitamin D levels of the mothers who have premature deliveries, the results obtained give only indirect data about maternal morbidities and vitamin D. Epidemiologic studies are needed for investigating the possible maternal effects of low vitamin D levels during pregnancy.
Premature deliveries are also found to be increased in case of gestational vitamin D insufficiency22). In our study which included only premature infants, the number of patients with <5 ng/dL vitamin D levels was more than the other 2 groups. With our study, we found that 70% of the infants had deficient vitamin D levels.
Intrauterine fetal growth is regulated by the participation and interaction of fetal, placental and maternal factors. One of the factors accepted as a regulator is vitamin D. In a study, small for gestational age probability was found to be 7.5 fold higher in the babies of the mothers with <15 ng/mL vitamin D levels23). But, on the other hand, there are also studies which did not find a relationship between the pregnancy vitamin D levels and birth weight and length. In a study carried out by Javaid et al.24), no relationship between the third trimester vitamin D levels and neonatal birth weight, length and head circumference was found. Birth weight, head circumference and intrauterine growth restriction incidence of premature infants were similar between the 3 groups in our study.
Our study has potential limitations. First of all, none of the mothers were checked for their serum vitamin D levels before delivery. Secondly, we also do not have data related to other dietary factors which could be interfering with vitamin D level. Vitamin D in the circulation of the mother can pass through the placenta to the fetus. In the literature, cord-blood vitamin D levels are reported to be mainly 20% lower than the maternal blood levels25). Due to this knowledge, we supposed that the cord-blood vitamin D levels are proportional to the maternal blood levels. Besides, all the mothers in the study had a history of irregular vitamin usage. But the maternal vitamin D intake was found to the similar in all 3 groups. And thirdly, with the consideration as the possible effect of seasonal changes in vitamin D levels on the results, we only included the babies which are born during the summer period.
As a conclusion; our study is the first to investigate the relationship between the cord-blood vitamin D levels and neonatal sepsis in preterm infants. According to the results of our study, we concluded that there is no relationship between the cord-blood vitamin D levels and neonatal sepsis in preterm infants. Further evaluation in a larger sample of patients or randomized controlled trials is necessary to further explore our results.
Acknowledgments
I gratefully acknowledge the support and generosity of the Zekai Tahir Burak Maternity Teaching Hospital, Neonatal Intensive Care Unit, without which the present study could not have been completed. Dr. Sahin presented a version of this paper at the 4th International Congress of the UENPS 11th–14th, December 2014.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.