Epilepsy syndromes during the first year of life and the usefulness of an epilepsy gene panel
Article information

Abstract
Recent advances in genetics have determined that a number of epilepsy syndromes that occur in the first year of life are associated with genetic etiologies. These syndromes range from benign familial epilepsy syndromes to early-onset epileptic encephalopathies that lead to poor prognoses and severe psychomotor retardation. An early genetic diagnosis can save time and overall cost by reducing the amount of time and resources expended to reach a diagnosis. Furthermore, a genetic diagnosis can provide accurate prognostic information and, in certain cases, enable targeted therapy. Here, several early infantile epilepsy syndromes with strong genetic associations are briefly reviewed, and their genotype-phenotype correlations are summarized. Because the clinical presentations of these disorders frequently overlap and have heterogeneous genetic causes, next-generation sequencing (NGS)-based gene panel testing represents a more powerful diagnostic tool than single gene testing. As genetic information accumulates, genetic testing will likely play an increasingly important role in diagnosing pediatric epilepsy. However, the efforts of clinicians to classify phenotypes in nondiagnosed patients and improve their ability to interpret genetic variants remain important in the NGS era.
Introduction
Recent developments in molecular genetics have resulted in tremendous advances in the medical field. The increased understanding of genetics and the advancement of molecular technology have led to the identification of previously unknown causes of diseases, thereby facilitating the development of novel therapies. During the last decade, great progress has also been made in understanding the genetics underlying epilepsy. Among these factors, epilepsy syndromes that occur during the first year of life are interesting from a genetic standpoint. The incidence of epilepsy is high during the first year and then declines throughout childhood. Several symptomatic causes, including metabolic disorders and structural brain lesions, are the major causes of epilepsy during this period.1) However, seizures may occur in neonates and infants with normal neurologic or metabolic statuses and family histories of early-onset seizures. In addition, certain patients experience intractable seizures accompanied by psychomotor retardation. Genetic testing may be helpful in these cases. An accurate early genetic diagnosis is crucial not only for avoiding unnecessary investigation but also for enabling better treatment strategies in certain cases. A genetic diagnosis can also provide useful information regarding the natural history and prognosis of the disorder and much more accurate information regarding other at-risk family members than broad empirical risk assessments.2)
In this review, epilepsy syndromes with various prognoses beginning during the first year of life and appropriate genetic tests, particularly the epilepsy gene panel, are discussed.
Benign familial epilepsy syndromes in infancy
Three benign epilepsy syndromes with autosomal dominant inheritance patterns are recognized in infancy. These conditions are primarily differentiated by the age of onset with certain overlapping periods. The age of onset typically occurs before the fifth day of life in benign familial neonatal epilepsy (BFNE), between 2 days and 7 months of age in benign familial neonatal-infantile epilepsy (BFNIE), and between 3 and 8 months of age in benign familial infantile epilepsy (BFIE). The incidence of BFNE is estimated to be 14.4 per 1,000 live births3); the incidences of BFNIE and BFIE are unknown. These syndromes typically occur in previously normal neonates and infants. Afebrile focal and prominent motor seizures that are secondarily generalized predominate, and occasionally are associated with apnea, cyanosis, and staring. Interictal electroencephalograms (EEGs) are normal, and patients respond well to antiepileptic drugs. Developmental and intellectual outcomes are typically normal. A genetic diagnosis is crucial because these three conditions have significant clinical overlap.
1. Benign familial neonatal epilepsy
BFNE occurs at a mean age of approximately 3 days and remits at a mean age of 3 months. Up to 11% of affected patients suffer from subsequent seizures.3) This disorder was originally described in an Austrian family by Rett and Teubel.4) Subsequently, numerous BFNE families have been described, including many families with potassium channel subunit mutations, particularly in KCNQ2 and KCNQ3 (Table 1).5) An analysis of a cohort of unrelated BNFE patients yielded mutation frequencies of 56% for KCNQ2 and 6.6% for KCNQ3.5) A recent study involving 33 families with BFNE reported 27 families with a KCNQ2 mutation and one family with a KCNQ3 mutation, demonstrating that the KCNQ2 mutation is the most common mutation in BFNE.6) KCNQ2 and KCNQ3 encode voltage-gated potassium channel subunits Kv7.2 and Kv7.3.789) Kv7.2 and Kv7.3 form the heteromeric channel responsible for the M-current, which stabilizes the resting membrane potential and is therefore important for regulating neuronal excitability.

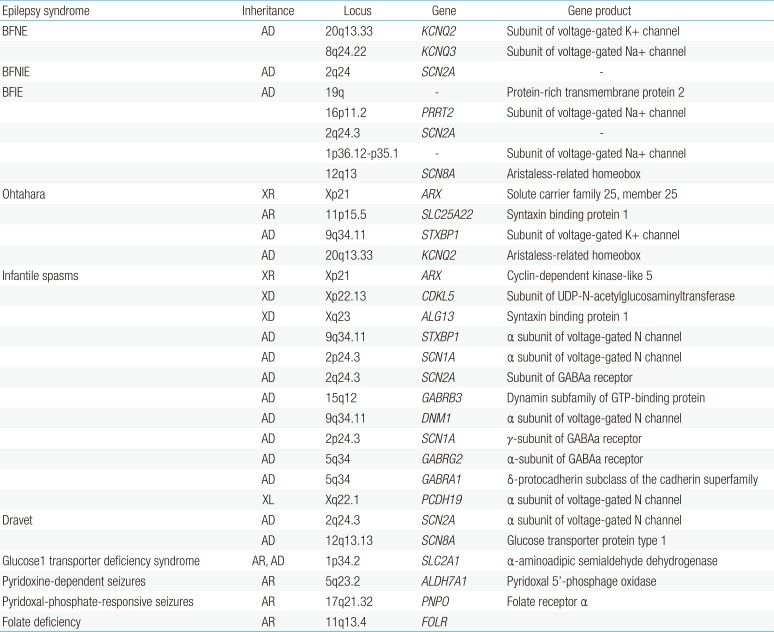
Epilepsy syndromes during infancy and commonly associated genes
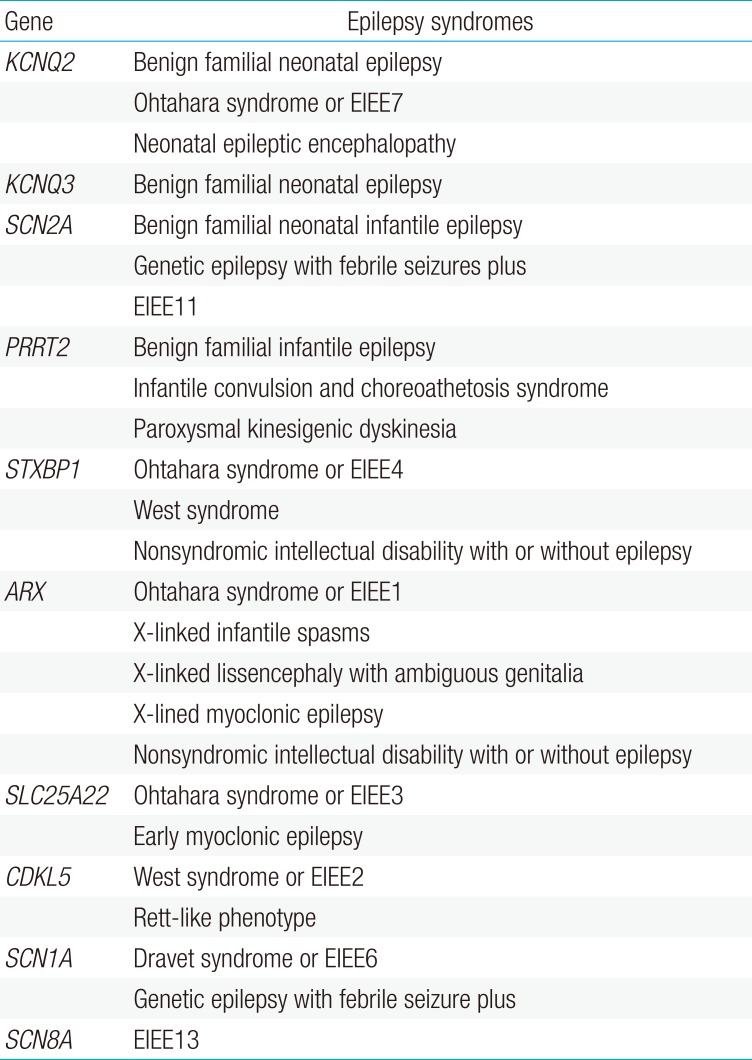
Interestingly, KCNQ2 mutations may present with a distinct phenotype characterized by neonatal seizures that evolve to drugresistant epileptic encephalopathy and mental retardation (Table 2).10111213) In these patients, the age of seizure onset and seizure type is similar to that of BFNE, but the seizures are resistant to therapy, and the seizure frequency gradually decreases over the first 5 years of life. EEGs show a burst-suppression pattern during the first few days of life, followed by multifocal epileptiform activities. During childhood, most patients suffer from profound intellectual disabilities and neurological abnormalities, such as hypotonia or spastic quadriplegia.141516)

Genotype-phenotype relationship of primary genes associated with benign familial epilepsies during infancy and early-onset epileptic encephalopathies
2. Benign familial neonatal-infantile epilepsy
BFNIE occurs between 2 days and 7 months of age and tends to remit by 1 year of age.17) This condition exhibits autosomal dominant inheritance and is often caused by a missense mutation in SCN2A, which encodes the α2 subunit of the voltage-gated sodium channel.18) This mutation increases the sodium current, leading to increased neuronal excitability.1920) BFNIE was first described as an intermediate phenotype between BFNE and BFIE. BFNIE is similar to BFNE, but the average age of onset differs; thus, these disorders cannot be consistently distinguished based on the age of onset.21) BFNIE is particularly difficult to diagnose in small families with limited clinical information, highlighting that genetic testing is the best and only method to distinguish BFNE from BFNIE.
Similar to the KCNQ2 mutation, the SCN2A mutation has a large range of phenotypes, including BFNIE and a variety of epilepsy syndromes, such as genetic epilepsy with febrile seizure plus (GEFS+), Dravet syndrome, and certain intractable childhood epilepsies. The mutations identified in intractable epilepsies alter the channel properties of NaV1.2 more than BFNIE mutations do, suggesting the mechanism of more severe epileptic phenotypes.22)
3. Benign familial infantile epilepsy
BFIE occurs between 3 and 8 months of age, and the seizures spontaneously remit before the age of 3 years.23) Seizures are typically not observed later in life; however, certain cases develop paroxysmal dyskinesia or paroxysmal kinesigenic choreoathetosis during adolescence. Additionally, certain patients in these families have paroxysmal movement disorders, suggesting that a common genetic defect underlies both disorders. This condition is referred to as infantile convulsion and choreoathetosis syndrome (ICCA). The main causative mutation underlying BFIE was identified in the PRRT2 gene.2425) Interestingly, this gene mutation was first identified as causing paroxysmal kinesigenic dyskinesia, and mutations in the same gene were subsequently reported in families with BFIE or ICCA.2426) PRRT2, which is located at chromosomal region 16p11.2, encodes a proline-rich transmembrane protein that is mainly expressed in the brain, i.e., the cerebral cortex and basal ganglia. The function of PRRT2 is currently unknown, but this gene may interact with synaptosomal-associated protein 25 kDa, which is involved in releasing neurotransmitters from synaptic vesicles.27) Currently, PRRT2 is among the main causes of BFIE and accounts for up to 70% of BFIE families.2425)
Epileptic encephalopathies
Certain children with seizures beginning during the first year of life have serious outcomes, including refractory epilepsy and psychomotor retardation. Epileptic encephalopathies are characterized by recurrent seizures and prominent interictal epileptiform discharges during the early infantile period.28) The numerous etiologies of epileptic encephalopathies are primarily associated with structural brain defects and inherited metabolic disorders. However, many pathogenic gene mutations could be involved in the development of epileptic encephalopathies. To date, more than 100 genes including STXBP1, ARX, SLC25A22, KCNQ2, CDKL5, SCN1A, SCN1A, POLG, SC2A1, and PCDH19 have been defined to be associated with early-onset epileptic encephalopathies.12930) These genes are classified as early infantile epileptic encephalopathy (EIEE) types and have been reported up to EIEE58 (https://www.ncbi.nlm.nih.gov/omim/).
1. Ohtahara syndrome
Ohtahara syndrome is characterized by intractable seizures during the first few weeks to months of the neonatal period, suppression-burst patterns on interictal EEGs, and poor developmental outcomes.31) The prognosis is typically grave, including severe psychomotor retardation and high mortality, particularly during the early stages of the disorder. Structural brain anomalies, inborn errors of metabolism, genetic abnormalities, and unknown factors are involved in the pathogenesis of Ohtahara syndrome. To date, various genes that play essential roles in the neuronal and interneuronal functions of the brain have been associated with Ohtahara syndrome. Syntaxin-binding protein 1 (STXBP1), which regulates the release of synaptic vesicles and the secretion of neurotransmitters, is the most important cause of Ohtahara syndrome.32) Other genes include aristaless-related homeobox (ARX), which acts as a regulator of the proliferation and differentiation of neuronal progenitors33); solute carrier family 25 member 22 (SLC25A22), which encodes a mitochondrial glutamate transporter34); and potassium voltage-gated channel (KCNQ2), which plays a key role in the generation and transmission of electrical signals.13)
2. Infantile spasms (West syndrome)
The main characteristics of infantile spasms include developmental regression and a characteristic hypsarrhythmia on interictal EEGs.35) The spasms typically start between 4 and 6 months of age with clustering and are typically observed as an infant awakes from or falls to sleep. The hypsarrhythmic EEG pattern consists of random, high voltage, nonsynchronous spikes and slow waves of variable duration and topography.35) A fraction of the symptomatic causes of infantile spasms, including chromosomal abnormalities, hypoxic ischemic encephalopathy, and intracranial infection, has been steadily increasing due to improved diagnostic techniques.36) The developmental outcome of infants with infantile spasms is poor. Mental retardation is recorded in approximately 70% to 80% of cryptogenic infantile spasm cases and 85% to 90% of symptomatic infantile spasm cases.35) Although infants with cryptogenic infantile spasms have better prognoses than infants with symptomatic infantile spasms, the outcome of infants with cryptogenic infantile spasms remains poor.37) ARX and CDKL5 are among the genes most frequently associated with infantile spasms. The other reported mutations are summarized in Table 1.
3. Dravet syndrome
Dravet syndrome or severe myoclonic epilepsy of infancy is a rare epileptic encephalopathy. This disease is characterized by generalized febrile or hemiconvulsive seizures starting during the first year of life, followed by multiple types of intractable afebrile seizures and psychomotor retardation.38) At its presentation, interictal EEGs and brain imaging are normal, which often delays diagnosis. The seizures are refractory to antiepileptic drug therapy, and the affected patients have a high mortality rate due to the increased risk of status epilepticus and sudden unexpected death.38) Sodium channel blockers, such as lamotrigine and carbamazepine, should be avoided, while valproic acid, topiramate, clobazam, and stiripentol may be beneficial.39) SCN1A has been implicated in the phenotype of 70%–80% of patients with Dravet syndrome.40) This gene encodes a voltage-gated sodium channel and is mainly associated with neuronal excitability. SCN1A has also been associated with generalized epilepsy with febrile seizure plus (GEFS+).41) The identification of a mutation in SCN1A is important for the early diagnosis and appropriate treatment of Dravet syndrome. However, not all patients exhibit SCN1A mutations. Various genes, including GABR2, SCN2A, and SCN8A, have also been reported to cause Dravet syndrome.4243)
Application of an epilepsy gene panel in patients with epilepsy syndromes during the first year of life: benefits and limitations
Many studies have attempted to elucidate the genetics of epilepsy over the past 2 decades. Many advances have been made, such as the complexities of phenotype-genotype relationships and the discovery of numerous genes associated with epilepsy.44)
Several genetic testing methods are currently available (Table 3). Sanger sequencing is preferentially indicated in patients with well-defined phenotypes associated with a single gene mutation and is the gold standard for detecting small sequence variations. To increase the diagnostic yield of this test, clinical expertise leading to the suspicion of a causative gene is required. Sanger sequencing enables the screening of only one gene at a time and is often expensive and time consuming because several rounds of testing are needed. On the other hand, NGS is a high-throughput DNA sequencing technology that can analyze thousands of genes in a single reaction.4546) Using NGS, a targeted gene panel including only phenotypically relevant genes has become available. Currently, several commercial epilepsy gene panels, each containing 70–465 genes, are available.47) As research studies increase our current understanding, new genes will be added to the list.

Comparison of genetic testing strategies
Epilepsy gene panels are cost-effective time-saving methods of simultaneously examining multiple genes associated with a disease, particularly in various infantile epilepsy syndromes, with which multiple genes are associated.2029) Epilepsy gene panels also simplify the decision-making process for the ordering physician. Several studies have demonstrated the diagnostic yield of gene panels. A German study reported that 16 of 33 patients (48%) with epileptic disorders were successfully diagnosed using a targeted epilepsy gene panel of 265 genes.45) Ortega-Moreno et al.48) reported that in 17 of 87 patients (19.5%), disease-causing variants were able to be identified via a gene panel with the highest yield in patients with early-onset epileptic encephalopathies. In a study of 400 patients with early-onset epilepsy and developmental delay tested with a gene panel, 30 of 77 (39%) of those with seizure onset within the first 2 months had a causative mutation.49) Recently, Mercimek-Mahmutoglu et al.50) reported that targeted epilepsy gene panels have increased the diagnostic yield from <10% to >25% in patients with epileptic encephalopathy. These authors insisted that epilepsy gene panels are a cost-effective alternative to Sanger sequencing of individual genes for the genetic diagnosis of epilepsy. However, gene panel testing has several limitations. Because the gene panels include only genes that have been previously identified, a disease caused by a mutation of a previously unknown gene could be missed. Several researchers question the usefulness of gene panels in an era during which new genes are discovered daily at high rates.
Considering which genes to include in a panel applied in genetic testing is important. Genes that are strongly associated with a disorder should certainly be included to increase the diagnostic yield. However, if physicians include all genes that are remotely associated with a phenotype under the assumption that more is better, the gene of interest may ultimately be revealed to not be the cause of the phenotype. Therefore, close communication between clinicians and laboratory geneticists is essential for selecting the appropriate gene panel because the gene panel should be understood by the ordering physician from a clinical perspective.
Finally, targeted NGS is not technically an independent diagnostic test and requires confirmation using a second method. Complementary Sanger sequencing is often required due to the low coverage and no-coverage exons, and complementation using a single nucleotide polymorphism array is required to detect the copynumber variations in the targeted genes.
Whole exome sequencing (WES) enables the investigation of all exons in the genome and could be performed if a genetic disease without a specific available test is suspected or if the specific genetic tests are negative.51) This method can discover new genes if a number of patients with similar phenotypes carry similar variants.52) However, WES is expensive and time consuming, which combined with the complexity of interpreting WES data, prevents many physicians from ordering this analysis as a first-line test.
Conclusions
In conclusion, benign familial neonatal/infantile epilepsies and epileptic encephalopathies have a wide variety of genetic etiologies, and new genetic causes are continually discovered. Epilepsy gene panel testing using NGS can be useful for patients with epilepsy syndromes during the first year of life because clinical diagnosis is difficult and multiple genes are implicated although there are several limitations. Its application is currently covered by the Korean National Health Insurance since 2017 in 17 institutions. The dramatically reduced cost of genetic testing and the accumulation of genetic information could enable genetic testing as a part of routine pediatric epilepsy diagnosis before long. The role of the clinician in selecting the best genetic testing method remains important, and the clinician plays a role in interpreting whether an identified genetic variant is causing a child's phenotype.
Acknowledgments
This study was supported by the Basic Science Research Program of the National Research Foundation of Korea funded by the Ministry of Science, ICT and Future Planning (NRF- 2017R1C1B5076772).
Notes
Conflicts of interest: No potential conflict of interest relevant to this article was reported.