Evaluation of prolonged pain in preterm infants with pneumothorax using heart rate variability analysis and EDIN (Échelle Douleur Inconfort Nouveau-Né, neonatal pain and discomfort scale) scores
Article information

Abstract
Purpose
The EDIN scale (Échelle Douleur Inconfort Nouveau-Né, neonatal pain and discomfort scale) and heart rate variability has been used for the evaluation of prolonged pain. The aim of our study was to assess the value of the newborn infant parasympathetic evaluation (NIPE) index and EDIN scale for the evaluation of prolonged pain in preterm infants with chest tube placement due to pneumothorax.
Methods
This prospective observational study assessed prolonged pain in preterm infants with a gestational age between 33 and 35 weeks undergoing installation of chest tubes. Prolonged pain was assessed using the EDIN scale and NIPE index.
Results
There was a significant correlation between the EDIN scale and NIPE index (r=-0.590, P=0.003). Prolonged pain is significantly more severe in the first 6 hours following chest tube installation (NIPE index: 60 [50–86] vs. 68 [45–89], P<0.002; EDIN score: 8 [7–11] vs. 6 [4–8], P<0.001).
Conclusion
Prolonged pain can be accurately assessed with the EDIN scale and NIPE index. However, evaluation with the EDIN scale is time-consuming. The NIPE index can provide instantaneous assessment of prolonged and continuous pain.
Introduction
Newborns observed in the neonatal intensive care units (NICU) are exposed to painful interventions every day and this in turn affects their further developments [1,2]. Acute pain is the most common type of pain in NICU. Chronic pain is defined as pain that takes 3 months in children, whereas in the newborn, this period has not been defined yet [3]. Therefore, long-term pain in the newborn can be defined as prolonged pain [4-7]. Pain assessment in neonates is among the most difficult challenges faced by health professionals. The main goal in assessing the pain response is, infant's painful condition determination of the level of pain [8]. Exposure of the newborn to pain leads to negative effects, both in the short- and long terms [2,9,10]. It is difficult to define prolonged pain compared to the acute pain, and thus it may not be treated. Pain relief is the primary issue in the newborn intensive care units. Correct evaluation of the pain provides correct determination of the analgesic need and the efficacy of the analgesics [11].
Acute pain may be assessed via many different tools, although a limited number of scoring systems are available to assess prolonged pain. Among these, the EDIN scale (Échelle Douleur Inconfort Nouveau-Né, neonatal pain and discomfort scale) is the most commonly used scoring system that assesses prolonged pain in preterm infants using five different behavioral elements [5]. In practice, the EDIN scale may be used 2 or 3 times daily at the NICU, and it may show variations between observations. Despite the availability of methods assessing prolonged pain such as the approved EDIN scale, the need for new methods has continued due to its long observation time and its inability to detect pain severity fluctuations [12,13].
The physiological effects of painful stimuli arise through the autonomic nervous system (ANS) [12]. Heart rate variability (HRV), parasympathetic and sympathetic transmission from the central nervous system to the sinoatrial nodule due to differences in levels [13]. Changes in parasympathetic stimulation that are particularly effective at HRV. HRV is a well-established non-invasive measure of cardiac autonomic control [14]. Previous studies have shown that painful stimuli cause a decrease in parasympathetic stimulation and thus a decrease in HRV [13-15]. The Newborn Infant Parasympathetic Evaluation (NIPE) monitor, based on HRV analysis, has been developed specifically for prolonged pain detection and continuous monitoring [12]. Ultimately, the NIPE index assesses parasympathetic excitability and may be a good decision aid for pain assessment for health professionals [12-15].
The aim of this study was to evaluate prolonged pain in premature infants undergoing chest tube installation due to pneumothorax using the EDIN scale and the NIPE index, and to compare the correlations between the 2 methods.
Materials and methods
1. Study population
This prospective and observational study was conducted at the NICU in Zekai Tahir Burak Hospital between February 1, 2015 and July 30, 2016. Premature infants with a gestational age of between 33 and 35 weeks undergoing chest tube installation due to pneumothorax were included in the study. Patients with circulatory system disorders necessitating vasopressor drug administration, a need for mechanical ventilation, congenital abnormalities, severe cardiac malformation and parents do not allow were excluded from the study. The release of this study and the data was approved by the local ethics committee, and all parents of the studied babies gave informed consent for data analysis and data publication.
2. Study protocol
Patients included in the study were administered fentanyl 1 μg/kg IV (over at least 5 minutes) and subcutaneous lidocaine 1% 2 mg/kg buffered with sodium bicarbonate (1:10) 2 minutes prior to chest tube placement [11]. The 8-Fr chest tube is placed in the midaxillary line 4–5, intercostal space. Then, fentanyl 1 μg/kg was continued once every 6 hours, and pain monitoring was performed via the EDIN scale and the NIPE monitoring.
3. NIPE monitor
The NIPE monitor (Mdoloris Medical Systems, Lille, France) is designed to assess HRV. The NIPE index is based on continuous cardiac signal (electrocardiography or plethysmographic waveform) processing. The detection of each heartbeat is realized and the RR series is computed as the time evolution of the period between 2 heart beats. The RR series are resampled at 8 Hz and the mean centered and normalized in a 64-second moving window [12]. A wavelength-based high pass filter over 0.15 Hz is applied in order to keep parasympathetic-related variations only, which are mainly affected by the respiration cycle. Following the RR filtering, local maxima and minima are determined in the 64-second window. Lower and upper envelopes are plotted in order to compute 4 areas under the curves (AUC) (one area/16 seconds: A1, A2, A3, and A4). AUC min is detected as the minimum value of A1, A2, A3, and A4. In order to obtain a value normalized between 0 and 100, it has been defined as the NIPE index: NIPE=100*(5.1*AUCmin+1.2)/12.8, where 12.8 corresponds to the maximum AUC value (A1+A2+ A3+A4=64×0.2=12.8 cf.) and where the linear equation’s values (5.1 and 1.2) were defined empirically on a 200-patient population in order to keep a good correlation between the visual information and the numerical value.
In clinical practice, a NIPE close to 100 corresponds to a high level of comfort. On the opposite, a NIPE close to 0 can be interpreted as a very low comfort level, which could be related to a high stress level [12]. The algorithm is computed continuously by sliding the moving window with a 1-second moving period. NIPEm is then computed as the record’s last 20 minutes mean value, but the software also gives a value of instantaneous NIPE for short-term analysis of neonatal high frequencies HRV. The mean NIPE scores were assessed every twenty minutes and the mean values were recorded for each hour in the first 12 hours.
4. EDIN scale
The EDIN scale uses 5 behavioral indicators of prolonged pain: facial activity, body movements, quality of sleep, quality of contact with nurses, and consolability [8]. Each indicator is scored from 0 to 3 and the EDIN scale is the sum of the five items; that is, the final score ranges from 0 to 15 [5]. An EDIN score of >6 demonstrates the presence of marked pain clinically [16]. At the end of a 6-hout observation period, the nurses calculate the EDIN score while performing their duties.
5. Statistical analysis
Statistical analyses were performed using the IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). The descriptive data for categorical variables were given as frequencies (%) and for continuous variables as median (interquartile range) or mean (±standard deviation) as appropriate. Mann-Whitney U test was used for the comparison of nonnormally distributed variables. While investigating the association between EDIN scale and NIPE index, Spearman correlation test was used. A P value of <0.05 was considered statistically significant.
Results
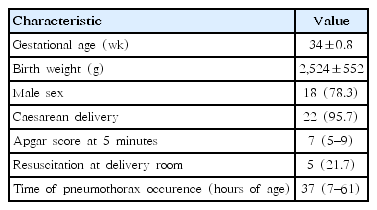
A total of 23 preterm infants were included in the study (Fig. 1). The patient characteristics have been presented in Table 1. The mean gestational week of the infants was 34±20.8 weeks and the mean birth weight was 2,524±552 g. Five preterm infants (21.7%) had undergone positive pressure ventilation after birth. The median time for development of pneumothorax and chest tube installation in the study group was 37 (7–61) hours of age (Table 1).

Study population.
Demographic and clinical characteristics of study groups
The median NIPE index within the first 6 hours after chest tube installation was 60 (50–86), and it was 68 (45–89) within the second 6 hours (P<0.002). The median EDIN score within the first 6 hours was 8 (7–11), and it was 6 (4–8) in the second 6 hours (P<0.001) (Table 2). A significant negative correlation was determined between the EDIN scale and the NIPE index measured within both 6-hour periods (r=-0.590, P=0.003).

Comparison of EDIN scale and NIPE monitor values
Discussion
We aimed to evaluate the pain level using the NIPE monitoring and the NIPE index that has been developed recently, and the EDIN scale, which is a classical method in premature infants undergoing chest tube installation due to pneumothorax. We recorded the highest pain levels within the first 6 hours following chest tube installation. A significant negative correlation was observed between the NIPE index and the EDIN score during the course of the chest tube. We concluded that NIPE monitoring is a reliable method in monitoring of prolonged pain. Within the second 6-hour-period after chest tube installation, the EDIN scores were decreased and the NIPE indexes were increased. This was evaluated as adaptation to pain and relieved comfort in response to the administered analgesics.
The number of studies evaluating pain observed as a result of treatment in the newborn with respiratory distress is limited in the literature. In a study investigating the effect of fentanyl infusion on acute and prolonged pain in preterm infants receiving mechanical ventilation, fentanyl was shown to reduce acute pain but not affect prolonged pain. However, severe prolonged pain (EDIN score of >6) in the placebo group was found to be significantly high compared to the fentanyl group [17]. In our study the EDIN score in the first 6 hours was found to be high showing prolonged pain.
The EDIN scale is affected by gestational age and postnatal age. Passing from 32 and 37 weeks to 37 weeks and higher results in a 1-point increase in the scale. Likewise, the EDIN score significantly increases with the increase in postnatal age between 0, 60, and 120 days. Furthermore, the need for respiratory support, sepsis and surgical operations affects the EDIN score to be >6 [11]. The preterm infants included in our study had close gestational ages and similar characteristics.
Studies suggesting that pain should be one of the monitoring parameters in NICU have demonstrated that prolonged pain could be assessed using HRV [12,13,15]. It has been shown in these studies that pain perception centers in the brain are associated with the centers regulating cardiovascular functions [18,19]. Neurons that receive nociceptive impulses and those that start autonomic responses are close to each other in most regions of the brain, and they are related to each other in central and peripheral levels [19]. Painful or stress stimuli affect the physiological functions via the effect of the ANS. The real time effect of ANS on body regulation may be monitored via HRV. HRV is a well-constructed noninvasive measuring method for cardiac autonomic control [14,18]. HRV is formed by altered parasympathetic and sympathetic stimuli levels from the central nervous system to the sinoatrial node of the heart. In particular, the changes in the parasympathetic outflow lead to major changes in HRV. Parasympathetic and sympathetic outflows lead to a lower number of changes in HRV [20]. A parasympathetic stimulus decreases during painful stimuli in infants [18]. The decreased parasympathetic stimulus results in reduced HRV. It has been determined in the study of Smith et al. [21] that massage leads to comfort and an increase in HRV in preterm infants. In another study, an increase in HRV was observed during kangaroo care for heel puncture in preterm infants [22].
In 2 different studies of De Jonckheere et al. [13] and Faye et al. [15], a decreased HRV was observed in high EDIN score that indicates prolonged pain, and an increased HRV was observed in low EDIN score. It has been reported that the decrease in HRV is a good indicator of prolonged pain, and that HRV analysis and the EDIN scale are correlated [13,15]. Subsequently, the NIPE Monitor was developed by Butruille et al. [12] in order to monitor the real time prolonged pain. In the study of Butruille et al.12) infants with a gestational age longer than 34 weeks were divided into 2 groups as low and high EDIN groups following a major surgical operation, and the NIPE index was found to be significantly low in the high EDIN group, which indicated a decreased HRV. Furthermore, a significant negative correlation was determined between the EDIN score and the NIPE index. Similar to the studies of De Jonckheere et al. [13], Faye et al. [15], and Butruille et al. [12], a significant decrease was determined in the high EDIN scores that indicate prolonged pain and a negative correlation between the NIPE index and the EDIN score in our study. Considering the data obtained in our study, we believe that NIPE monitoring is an effective and reliable method in the evaluation of painful interventions.
The most important advantage of the NIPE monitor from the EDIN scale is that it is possible to assess prolonged pain in a very short period of time. It also provides instant and continuous evaluation. The NIPE monitor is a noninvasive method that provides objective data in assessing prolonged pain to clinicians. Since environmental factors affect HRV, similar environmental conditions must be provided for monitoring the baby. Factors such as age of pregnancy and drug use also affect HRV. However, even in such a case, continuous monitoring with the NIPE monitor can cause the NIPE index to decrease if there is prolonged pain. However, in order to fully determine the effect of these conditions, it will be the end result of studies that will include newborns at different gestational ages or who use and do not use medicines that affect HRV.
The NIPE index that is used in our study may be affected by various environmental factors. HRV is controlled by the ANS outflow, which is altered by numerous factors including maturation, environmental conditions or drugs [11]. However, the environmental conditions were strictly controlled in our study. Furthermore, the sample size of the study was small. However, the data obtained are of clinical practical value.
Prolonged pain can be accurately assessed via EDIN scale and NIPE monitors. However, a long time period is required for evaluation with the EDIN scale. With the NIPE monitors, instantaneous and continuous prolonged pain can be assessed.
Notes
No potential conflict of interest relevant to this article was reported.