Impact of obesity on pulmonary function of preschool children: an impulse oscillometry study
Article information

Abstract
Background
The increasing global prevalence of obesity poses significant public health problems, as obesity exerts adverse effects on many systems and lung function. However, research on the lung function of preschool children with obesity is limited and inconclusive. In addition, studies specific to obesity indices that influence lung function in young children with obesity are limited.
Purpose
This study aimed to evaluate lung function of obese versus normal-weight preschool children using impulse oscillometry (IOS) and identify obesity indices predictive of altered lung function.
Methods
We enrolled obese children aged 3–7 years as well as age- and sex-matched normal-weight controls. The participants underwent IOS assessments that measured the resistance at 5 Hz (R5) and 20 Hz (R20), the difference in resistance between these frequencies (R5–R20), reactance at 5 Hz (X5), resonance frequency, and reactance area (AX). We compared these parameters between groups and analyzed the correlations between obesity indices and IOS measures within the obese group using multiple linear regression.
Results
The study included 68 participants (n=34 each group). In the obese group, significantly higher values were observed for R5 (adjusted for height, P=0.02; % predicted, P=0.01; z score, P<0.001), R5–R20 (absolute value, P=0.002; adjusted for height, P=0.001), and AX (z score, P=0.01). AX adjusted for height showed a greater trend (P=0.07). The waist-to-height ratio was the most robust independent predictor of total and peripheral airway resistance, with increases in R5 (b=1.65, P=0.02) and R5–R20 (b=1.39, P=0.03) and a near-significant correlation with AX (b=12.12, P=0.06).
Conclusion
Preschool children with obesity exhibit impaired lung function, characterized by elevated total and peripheral airway resistance. Waist-to-height ratio was the strongest predictor of these changes.
Key message
Question: Does obesity in preschool children affect lung function, and which obesity indices can predict such alterations?
Finding: Preschool children with obesity exhibit impaired lung function characterized by elevated total and peripheral airway resistance. Waist-to-height ratio was the strongest predictor of such changes.
Meaning: Early obesity prevention and treatment are needed. Monitoring waist-to-height ratio, body weight, and body mass index may help identify children at risk of altered lung function.
Introduction
The rising global prevalence of obesity poses a significant public health challenge because it adversely affects the metabolic, cardiovascular, and respiratory systems. Obesity is associated with various respiratory complications including obstructive sleep apnea, exercise intolerance, and altered lung function [1-3].
Among obese children and adolescents, recent studies and meta-analyses have shown a decreased ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC), despite the presence of normal or elevated FEV1 and FVC values [3-6]. Traditionally, spirometry has been the primary tool for assessing lung function in these populations. However, its requirement for substantial patient effort and cooperation limits its utility in preschool-aged children, who often cannot perform the test reliably.
In contrast, impulse oscillometry (IOS) is better suited for young children due to its reliance on tidal breathing and minimal patient cooperation, simplifying the assessment process [7]. The IOS is also more sensitive than spirometry for detecting resistance in both central and peripheral airways, making it a superior choice for evaluating smaller airways [8]. Research has demonstrated that IOS can detect increased peripheral airway resistance in obese school children and adults even when spirometry results are normal [9,10].
Only 2 prior studies [11,12] have explored the impact of obesity on lung function in preschool children using IOS. Kalhoff et al. [11] reported a slight increase in resistance at 5 Hz compared to the reference values but no significant changes in IOS parameters with increasing body mass index (BMI). Conversely, Lauhkonen et al. [12] reported no notable differences in IOS parameters between obese and normal-weight children but found correlations with BMI z scores.
Research on IOS-measured lung function in preschool-aged and school-aged children with obesity remains limited and inconclusive. Previous studies have focused predominantly on BMI and overlooked other potential obesity indices, such as chest circumference (CC), waist circumference (WC), hip circumference (HC), and waist-to-height ratio (WHR). Consequently, the current investigation aimed to compare lung function using IOS between obese and normal-weight preschool children and to identify obesity indices, including BMI z score, CC, HC, and WHR, that might predict changes in lung function. The findings may deepen our understanding of how obesity affects respiratory mechanics in this specific age group, leading to improved management strategies.
Methods
1. Study protocol
This cross-sectional study, conducted from February 2023 to February 2024 at the Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University in Bangkok, Thailand, involved children aged 3 to 7 years. The participants included children diagnosed with obesity and a control group of age- and sex-matched, normal-weight children. Obesity was defined per the World Health Organization (WHO) criteria as a BMI z score >3 for children ≤5 years and >2 for those >5 years [13]. Normal weight was characterized by a BMI z score between -1 and 1. Children were excluded if they had a history of pulmonary, cardiac, or neuromuscular diseases; prematurity; exposure to environmental tobacco smoke; respiratory infection in the past 4 weeks; or inability to perform the IOS test. The study protocol and IOS procedures were explained to participants and their guardians, who provided written informed consent. The study received ethical approval from our center’s Institutional Review Board under approval number Si-029/2023.
Detailed demographic and obesity-related data, including age, sex, height, body weight (BW), BMI, BMI z score, CC, WC, and WHR, were recorded. The same well-trained technician performed all pulmonary function tests using IOS.
2. Anthropometric evaluation
Anthropometric measurements were obtained using standardized tools from TANITA Corp. (Tokyo, Japan). BW and height were recorded to calculate BMI, which was defined as the BW in kilograms divided by the height in meters squared (m2). BMI was further adjusted for age and sex to compute the BMI z score, referencing WHO growth standards [14]. The CC, WC, and HC were accurately measured at the nipple level, between the lower margin of the last rib and the iliac crest, and at the largest circumference around the buttocks, respectively.
3. IOS measurement
IOS evaluations were conducted with the Vyntus IOS device (Vyaire Medical, Mettawa, IL, USA) and in strict adherence to European Respiratory Society guidelines [15]. Participants were seated with their heads in a neutral position, and a nose clip was used to minimize nasal air leakage. An investigator or caregiver supported each participant’s cheeks to prevent pressure loss. Participants maintained a firm seal on the mouthpiece and breathed normally. Each IOS maneuver lasted at least 16 seconds, with short breaks between attempts. Only maneuvers free from artifacts such as coughing, swallowing, vocalization, breath holding, or mouth opening were selected. The procedure was repeated until 3 consistent readings were achieved, with a coefficient of variation ≤15%. The mean of the 3 best trials was then calculated.
4. IOS measurement parameters
The IOS-measured parameters included resistance at 5 Hz (R5) and 20 Hz (R20), indicating total and central airway resistance, respectively. The difference between these frequencies (R5–R20) represents peripheral or small airway resistance. Reactance at 5 Hz (X5) evaluates airway obstruction and restriction, while the area of reactance (AX) and the resonance frequency (Fres) assess peripheral airway obstruction and lung compliance [16]. The percent predicted values for R5, R20, X5, and Fres were computed using the default reference data provided by Dencker et al. [17].
To account for ethnic differences in lung function, z scores for the IOS parameters were calculated using specific reference values for Asian populations, as delineated by Lee et al. [18] and Lai et al.19) The z scores were derived using the following formula: ([measured value – predicted value]/residual standard deviation) of a normative population).
5. Statistical analysis
Sample size in the normal and obese group was estimated based on the objective of comparing mean of IOS parameters between the 2 groups. Previous study in children revealed a statistically significant difference in mean R5 between normal and obese subjects [9]. Mean (standard deviation [SD]) of R5 value in the normal and obese group were 0.57 (0.14) and 0.68 (0.19) respectively [9]. Using a 2-sided type I error of 0.05, 80% power, n1=n2, a difference in mean R5 of 0.11 and SD of 0.14 and 0.18, a sample of 34 subjects in each group was required.
Normally distributed continuous variables are presented as the mean±SD, and categorical variables are presented as the frequency and percentage. Shapiro-Wilk test was performed to test normality of data. Independent sample t tests were utilized to compare anthropometric and IOS parameters between the obese and control groups. Given the average height difference of 7.82 cm between obese and normal-weight children and the impact of height on IOS values [17-19], multiple linear regression adjusted for group (normal, obese) and height was applied to accurately compare IOS parameters across groups. Additionally, multiple linear regression analysis within the obese group explored the influence of obesity indices on IOS parameters, with results presented as correlation coefficients (b) and P values. The presence of multicollinearity among independent variables was assessed using the variance inflation factor. All tests were deemed statistically significant at a P value<0.05. Analyses were conducted using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
Results
Sixty-eight children, equally divided into obese and normal-weight groups (34 each), participated in this study. There were no significant differences in age or sex between the groups. Children in the obese group were significantly taller, and all anthropometric measurements—BW, BMI, BMI z score, CC, WC, HC, and WHR—were markedly greater than those in the normal-weight group. The family history of asthma and allergic rhinitis in parent and siblings was not different between the groups (Table 1).
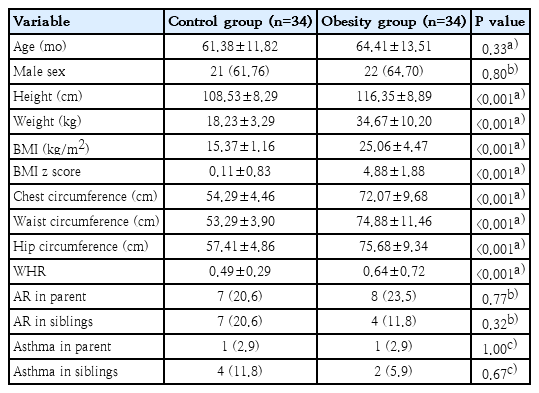
Comparative demographic and anthropometric data of control versus obese groups
According to the IOS assessments, the resistance at 5 Hz (R5) was marginally higher in the obese group by 0.06 kPa/L/sec (P=0.16), but this difference increased to 0.11 kPa/L/sec (P=0.02) after adjusting for height. The R5 z scores, adjusted based on reference data from Korean [18] and Taiwanese [19] populations, were significantly higher in the obese group (P<0.001). The difference in resistance between 5 Hz and 20 Hz (R5–R20) also showed greater values in the obese group both in absolute terms (0.11 kPa/L/sec, P=0.002) and after height adjustment (P=0.001). The absolute value of AX demonstrated no significant initial difference (P=0.25). However, adjustments for the z score revealed significant differences (P=0.01), with a trend to increase but no significant difference following height adjustment (P=0.07). No significant differences in R20, X5, or Fres were observed before or after adjustment (Table 2).

Impulse oscillometry parameters of control versus obese groups
Multiple linear regression analysis indicated that, among obese preschool children, the WHR was positively correlated with both R5 (b=1.65, P=0.02) and R5–R20 (b=1.39, P=0.03) and showed a trending association with the AX (b=12.12, P=0.06). Conversely, the BMI z score, CC, HC, and sex did not correlate with the other IOS parameters (Table 3). However, no obesity indices were found to affect IOS parameters in normal-weight group (Table 4).

Multiple linear regression analysis of influence of obesity indices on impulse oscillometry parameters among preschool children with obesity

Multiple linear regression analysis of influence of obesity indices on impulse oscillometry parameters among normalweight preschool children
Discussion
This study provides evidence of altered lung function in obese preschool children, as indicated by IOS measurements. We observed significant increases in both total and peripheral airway resistance, with higher R5 and R5–R20 values than in the normal-weight group. Additionally, the AX tended to increase after height adjustment, and a significantly elevated AX z score was observed in the obese group. No significant differences were noted in R20, X5, or Fres across the groups.
To our knowledge, prior research on the impact of obesity on lung function in preschool children is limited. Our findings align with those of Kalhoff et al. [11], who reported increased R5 in obese preschool children. In contrast, Lauhkonen et al. [12] studied children aged 5–7 years who were diagnosed with bronchiolitis between 0 and 6 months and found no significant differences in standard IOS parameters (R5, R20, X5, and Fres) between the obese and normal-weight groups. Crucially, Lauhkonen et al. [12] did not report R5–R20 or the AX, parameters our study suggests are significant in assessing altered lung function due to obesity in young children.
Investigations into lung function in obese children and adolescents, as measured by IOS, are also limited and have yielded inconclusive results. Consistent with previous studies, our research revealed significant increases in R5, R5–R20, and the AX in obese subjects, with no changes in X5 [9,20,21]. However, our findings differed regarding Fres, which was elevated in earlier studies [9,21] but not in our study. Additionally, prior results for R20—indicative of central airway resistance—have been inconsistent. One study noted a significant difference [21], while another reported no variation [9]. The disparity in outcomes between our study and these reports may arise from differences in the age groups of the participants. More research is needed to determine the impact of obesity on lung mechanics via IOS.
There is evidence indicating that increased peripheral airway resistance is linked to a higher risk of asthma and wheezing [22-25]. Therefore, our finding of increased peripheral airway resistance in obese preschool children may imply that this group is at an increased risk for developing asthma and wheezing.
In this study, we explored the relationships between various obesity indices—BMI z score, CC, HC, and WHR—and lung function in obese preschool children. Our findings indicate that the WHR is the most robust independent predictor of increased total and peripheral airway resistance, as evidenced by higher R5 and R5–R20 values. Additionally, the WHR had trend to correlate positively with the AX, which is associated with peripheral airway resistance. Conversely, the BMI z score and other obesity indices did not demonstrate significant associations with lung function as measured by IOS in this population.
The limited predictive value of BMI or the BMI z score for altered lung function in individuals with obesity may be attributed to its composite measure of body size, encompassing both fat mass and lean mass, without specifically reflecting fat distribution. Previous studies focused solely on BMI in preschoolers reported different results. One study found no significant correlations with IOS parameters [11] while another demonstrated the association between BMI z score and R5, Fres, and frequency dependence of resistance [12]. Studies involving older children and adolescents, such as that of Ekström et al. [20], noted a correlation between BMI and R5–R20. Likewise, Wilhite et al. [21], who studied children aged 8–12 years, reported associations between the 95th percentile of BMI, percent body fat measured by dual-energy x-ray absorptiometry, and R5–R20. Our study differs in that it considered a wider range of obesity indices, offering a more comprehensive assessment.
Our study was the first to investigate the impact of the WHR, an indicator of abdominal fat deposition, on lung function in obese children using IOS. We found that the WHR is associated with increased total and peripheral airway resistance. This finding aligns with previous research on obese older children and adolescents, which identified abdominal obesity—measured by WC [26,27] or WHR [3,28]—as a predictive factor for alterations in lung function detectable through spirometry. Similarly, a study in adults by Molina-Luque et al. [29], highlighted the WHR as the most significant predictor of impaired lung function, with notably worse outcomes in obese individuals with a WHR exceeding 0.55. Our results, in addition to these studies, suggest that routine evaluations of obese individuals should include WC and WHR as well as BW and BMI. However, given the limited and inconclusive data available, further research is necessary to confirm the relationships between WHR, other obesity indices, and altered lung function in preschool-aged individuals.
Abdominal or central obesity characterized by a higher accumulation of visceral fat around the abdomen, is substantially associated with altered lung function [30-32]. The primary pathophysiological impact of abdominal fat deposition on lung function is believed to be excessive pressure on the diaphragm and abdominal viscera, which adversely affects lung expansion and diaphragmatic movement leading to decreased lung volume and increased airway resistance [21,31,33]. In addition, visceral fat produces pro-inflammatory cytokines that can contribute to low-grade systemic inflammation. This inflammation may adversely affect lung tissue and airway function [33,34]. Another explanation might be that visceral fat is a key component of metabolic syndrome which can further compromise lung function [33,34].
Given the limited and inconclusive existing research, further studies are essential to clarify the impact of obesity on oscillometric lung function parameters in obese children, particularly in preschoolers. Advancing our understanding of the pathophysiology related to obesity will enhance management approaches for this condition.
Our study excluded children with a history of pulmonary disease including asthma, reactive airways, and other obstructive and restrictive lung diseases, and also excluded those with exposure to environmental tobacco smoke. In addition, family history of asthma and allergic rhinitis was not different between obese and normal-weight group. Therefore, our findings provide particular evidence regarding the impact of obesity on altered lung function. This study has several limitations. First, the small sample size may affect the generalizability of our findings. Second, instead of using direct body fat measurement methods such as bioelectrical impedance analysis or dual-energy x-ray absorptiometry, we opted for simpler, more practical approaches suitable for routine clinical settings. Third, we did not collect data on variables like physical activity or diet that could influence outcomes.
In conclusion, our findings indicate that preschool children with obesity have impaired lung function, as evidenced by increased total and peripheral airway resistance (R5 and R5-R20 adjusted for height; AX z score), compared to normal-weight peers. The WHR emerged as the most significant predictor of this increased resistance. These results underscore the need for early obesity prevention and weight loss encouragement in young children. Additionally, monitoring the WHR, BW, and BMI may help identify preschool children at risk of altered lung function.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This research was supported by the Siriraj Research Development Fund of the Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand, under grant number IO-R016631032.
Acknowledgments
The authors extend their deepest gratitude to the participating children and their parents for their willingness to participate in this study. Special thanks to Assistant Professor Chulaluk Komoltri for her invaluable assistance with the statistical analyses. This research project was supported by Siriraj Research Development Fund, Grant number (IO) R016631032, Faculty of Medicine Siriraj Hospital, Mahidol University.
Author Contribution
Conceptualization: KU, AK; Data curation: AK, PC, KM; Formal analysis: KU, PC, AP; Funding acquisition: KU, AK; Methodology: KU, AK, PC, KM; Project administration: KU; Visualization: AK, KM; Writing - original draft: AK, AP; Writing - review & editing: KU