Intramuscular and subcutaneous gonadotropin-releasing hormone agonist tests for central precocious puberty in girls: a randomized controlled trial
Article information

Abstract
Background
Central precocious puberty (CPP) results from premature activation of the hypothalamic-pituitary-gonadal axis. Although the standard intravenous gonadotropin-releasing hormone (GnRH) stimulation test is often inaccessible, a subcutaneous (SC) GnRH analogue (GnRHa) test is used. However, the conventional SC route presents logistical challenges including prolonged observation times and the need for multiple blood draws. Thus, identifying a more efficient administration route could optimize clinical workflows and enhance patient comfort. This study aimed to determine whether intramuscular (IM) administration is comparable to SC administration by analyzing the time to peak luteinizing hormone (LH) levels.
Purpose
To evaluate and compare the time to peak LH levels and diagnostic timing of IM versus SC GnRH stimulation tests in girls with CPP.
Methods
This randomized controlled trial enrolled 92 girls with suspected CPP. Participants were assigned via 2:1 block randomization to receive 100 mcg triptorelin acetate via SC (n=62) or IM (n=30) injection. Serial blood samples for LH and follicle-stimulating hormone were collected at 0, 30, 60, 90, and 120 minutes.
Results
There were no significant differences between the 2 groups in demographic characteristics. Peak LH responses were most frequent at 30 minutes in both groups (IM, 33.3%; SC, 35.5%; P=0.88). The mean LH levels at 30, 60, 90, and 120 minutes did not differ significantly between groups. Diagnostic confirmation of CPP occurred within 30 minutes in 96.7% and 96.8% of patients in the IM and SC groups, respectively.
Conclusion
The IM GnRH stimulation test was comparable to the standard SC test in terms of LH response magnitude and timing.
Key message
Question: Did the intramuscular (IM) and subcutaneous (SC) administration of gonadotropin-releasing hormone (GnRH) agonists have comparable timing and diagnostic utility for evaluating central precocious puberty in girls?
Finding: Both the IM and SC GnRH stimulation tests demonstrated comparable times to peak luteinizing hormone levels.
Meaning: Clinicians may consider the IM route as a time-efficient alternative, as it offers similar diagnostic utility for central precocious puberty without compromising the detection of hypothalamic-pituitary-gonadal axis activation.
Graphical abstract. GnRHa, gonadotropin-releasing hormone agonist; IM, intramuscular; SC, subcutaneous; LH, luteinizing hormone.
Introduction
Central precocious puberty (CPP) is characterized by the premature activation of the hypothalamic-pituitary-gonadal (HPG) axis. The initial clinical manifestation in girls is typically the development of breast buds (Tanner stage II) upon physical examination [1,2]. Diagnostic criteria for CPP in girls include the onset of Tanner stage II breast development before the age of 8 years, accompanied by accelerated linear growth velocity, advanced skeletal maturation, and biochemical confirmation of HPG axis activation. This hormonal activation is indicated by either a basal luteinizing hormone (LH) concentration exceeding 0.3 IU/L or a peak stimulated LH level above 5 IU/L, as determined by immunochemiluminometric assay methods [1,3].
The gold standard for definitively diagnosing CPP involves the intravenous (IV) gonadotropin-releasing hormone (GnRH) stimulation test [4]. However, due to the limited availability of IV GnRH in many regions, including Thailand, the subcutaneous (SC) GnRH test has been widely adopted [5,6]. The SC route is often favored for its perceived ease of administration; however, it presents logistical challenges, including a prolonged duration and multiple blood draws [7,8]. While intramuscular (IM) administration of GnRH is common for therapeutic purposes, its use for diagnostic stimulation is less well-characterized in pediatric populations. Pharmacokinetic data for other analogues like leuprorelin suggest distinct absorption profiles between IM and SC routes, raising the question of whether IM triptorelin might offer a more rapid peak LH, potentially shortening the testing protocol. This study aims to directly compare the time to maximum LH concentration (Tmax-LH) between IM and SC triptorelin acetate administration.
Methods
1. Participants
This unblinded randomized controlled trial was conducted at the pediatric endocrinology clinic of King Chulalongkorn Memorial Hospital in Thailand. Eligible participants were girls who presented with the onset of breast development (Tanner stage II) before the age of 8 years, between 2022 and 2024. Girls with a history of exogenous hormone use or a diagnosis of congenital adrenal hyperplasia were excluded. Initially, 119 girls under the age of 8, presenting with Tanner stage II breast development, were enrolled and underwent both IM and SC GnRH stimulation tests. Participants were assigned to the SC or IM group using a block randomization method with a 2:1 ratio (SC:IM). Following these initial assessments, 27 girls were diagnosed with premature thelarche and subsequently excluded from the primary study cohort. The remaining 92 participants who were confirmed to have CPP based on established hormonal criteria (defined as a baseline LH level ≥ 0.3 IU/L or a peak LH level ≥5 IU/L after GnRH stimulation) were included. Written informed consent from guardians and assent from participants were obtained prior to study enrollment (Fig. 1).
Flowchart of 92 girls with central precocious puberty (CPP) randomized in the study. CAH, congenital adrenal hyperplasia; GnRHa, gonadotropin-releasing hormone agonist; IM, intramuscular; SC, subcutaneous.
2. Methodology
In this study, 100 μg of triptorelin acetate (Diphereline, Ipsen Pharma Biotech, France) was administered either intramuscularly or subcutaneously, according to group assignment. IM injections were administered into the deltoid muscle contralateral to the IV cannula used for blood sampling. SC injections were also given in the deltoid muscle. To maintain impartiality, the trained clinician responsible for administering the injections was not involved in other aspects of the study. Blood samples were collected to measure LH, follicle-stimulating hormone (FSH), and estradiol at baseline (pretest), and LH and FSH levels were measured at 30, 60, 90, and 120 minutes after GnRH injection.
Clinical data were systematically gathered, encompassing the participants' pubertal status and various auxological parameters. Specifically, this included chronological age, age at breast onset, and standard deviation scores (SDSs) for weight, height, and body mass index (BMI), calculated against World Health Organization growth standards. Further assessments involved determining breast Tanner stage and bone age, with the latter meticulously evaluated by 2 pediatric endocrinologists using the Greulich and Pyle method. Parental heights were also recorded to compute midparental height (MPH), and predicted adult height was estimated utilizing the Bayley-Pinneau method [9].
3. LH and FSH measurement assay
Plasma LH and FSH levels were determined by an electrochemiluminescence Immunoassay. The intra- assay and interassay coefficients of variation ranged from 3.3% to 3.6% and 3.2% to 7.3%, respectively.
4. Ethical consideration
This study received ethical approval from the institutional review board (IRB) of Chulalongkorn University Faculty of Medicine (IRB No. 0913/66). It adhered to international standards for human research protection, including the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and ICH-GCP. The study is registered with the Thai Clinical Trial Registry (TCTR20240719003).
5. Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 29.0 (IBM Co., USA). The study utilized a 2:1 randomization ratio; this ratio was selected to ensure the control arm remained robust while adequately powering the experimental IM arm. Continuous variables with normal distribution and binomial distribution were reported as mean (standard deviation) and median (interquartile range), respectively. Categorical data were presented as proportions (percentages). Differences in continuous variables between the 2 groups were assessed using the independent t test. The Pearson chi-square test was used to analyze differences in the frequency of the LH peak proportion. A P value of <0.05 was considered statistically significant.
Results
1. Demographic and baseline data
The study involved a cohort of 92 girl participants. Of these, 30 girls underwent IM GnRH stimulation tests, while the remaining 62 girls underwent SC GnRH stimulation tests. Initial demographic data —such as chronological age, age at breast onset, SDS for weight, height, and BMI, bone age, and MPH—are summarized in Table 1. There were no significant differences in these baseline characteristics between the 2 groups.
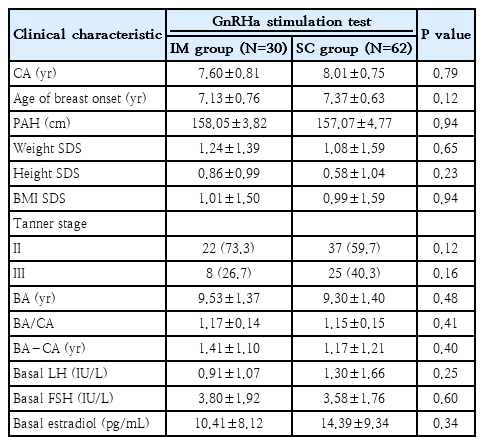
Participants' demographic and clinical characteristics
2. LH Response to stimulation
Table 2 and Fig. 2 present the mean LH levels at each time point. In the IM GnRH stimulation test group, the mean LH levels at 0, 30, 60, 90, and 120 minutes were 0.91, 17.46, 18.10, 16.72, and 15.50 IU/L, respectively. In the SC GnRH stimulation test group, the mean LH levels at the same time points were 1.30, 20.82, 21.24, 19.77, and 18.45 IU/L. No significant differences were observed between the 2 groups at any time point.

Mean LH levels after the GnRHa stimulation test
Mean luteinizing hormone (LH) level over time following gonadotropin-releasing hormone analogue (GnRHa) stimulation by study group. IM, intramuscular; SC, subcutaneous.
The frequency of peak LH responses is shown in Table 3. In the IM group, the peak LH responses occurred in 10 (33.3%), 9 (30.0%), 3 (10.0%), and 8 participants (26.7%) at 30, 60, 90, and 120 minutes, respectively. In comparison, the SC group showed peak responses in 22 (35.5%), 19 (30.6%), 9 (14.5%), and 12 participants (19.4%) at the corresponding time points. There were no significant differences in the proportions at each time point, with P values of 0.87, 1.00, 0.51, and 0.47, respectively. Data regarding peak FSH responses are provided in the supplementary Table 1.
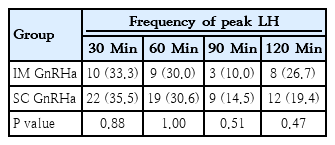
Frequency of peak LH at each time point
3. Diagnostic timing
We also analyzed the time to diagnosis of CPP using the GnRH stimulation test, as shown in Table 4. In the IM group, CPP was diagnosed in 29 girls (96.7%) within 30 minutes and in 1 girl (3.3%) within 90 minutes. In the SC group, CPP was diagnosed in 60 girls (96.8%) within 30 minutes and in 2 girls (3.2%) within 60 minutes. No significant difference was observed between the IM and SC groups.
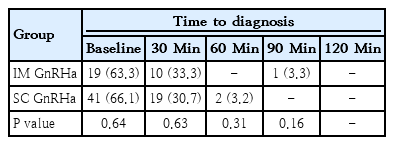
Cumulative time to diagnosis of CPP
Discussion
The diagnosis of CPP hinges on accurately assessing the activation of the HPG axis. In many parts of the world, including Thailand, the gold standard IV GnRH stimulation test isn't readily available [10-14]. As a result, SC GnRH stimulation tests, particularly those using triptorelin acetate, have become standard clinical practice. These tests have proven effective and accurate in distinguishing CPP from other forms of premature pubertal development, like premature thelarche [5,6].
However, the conventional SC GnRH stimulation test protocol presents significant logistical challenges. It requires blood sampling at 5 distinct time points over 120 minutes, leading to a prolonged procedure and the need to collect a relatively large total blood volume. This can cause considerable inconvenience and discomfort for patients. Given these practical limitations, we hypothesized that the IM route for GnRH administration could offer a more time-efficient alternative for CPP diagnosis. Notably, before this study, direct comparative data were scarce on the time to peak LH levels after IM versus SC administration of triptorelin acetate.
Our randomized controlled trial aimed to bridge this knowledge gap by directly comparing the time to Tmax-LH between IM and SC GnRH stimulation tests in girls with CPP. Contrary to our initial hypothesis that IM administration would significantly shorten the time to peak LH levels, our findings showed no significant differences in LH responses between the IM and SC groups at any of the measured time points. Both IM and SC triptorelin administration consistently demonstrated mean peak LH levels clustering around the 60-minute mark (IM, 18.10 IU/L; SC, 21.24 IU/L) [5,15-18]. Furthermore, the frequency of peak LH responses was comparable between the 2 groups across all time points, with a substantial majority of diagnoses occurring within 30 minutes in both cohorts. Our findings indicate that the IM route does not significantly accelerate the time to peak LH compared to the SC route, contrary to our initial hypothesis. Both routes resulted in peak LH clustering around 30 to 60 minutes.
However, a notable gap exists in the current literature regarding the pharmacokinetics of IM triptorelin. This lack of understanding hinders a comprehensive comparison with other GnRH. In contrast, existing pharmacokinetic investigations of 7.5-mg leuprorelin, a related GnRH, have demonstrated distinct absorption profiles depending on the administration route. Specifically, peak LH levels were observed approximately 2.1 hours following SC leuprorelin injection and at an earlier interval of 1-hour post-IM leuprorelin injection [19].
The findings from our study, which used a significantly lower dose of 100 μg of triptorelin for diagnostic stimulation in girls with suspected CPP, may not directly align with the aforementioned leuprorelin data. This lower dosage regimen could account for the observed similarity in the time to peak hormone levels between IM and SC triptorelin injections in our cohort. At such a reduced concentration, the overall drug load and subsequent absorption dynamics might be less influenced by the route of administration. Furthermore, it's crucial to acknowledge that triptorelin and leuprorelin, despite belonging to the same drug class, possess distinct molecular structures. Consequently, they may exhibit inherent differences in their pharmacokinetic and pharmacodynamic properties. These inherent differences could contribute to variations in their absorption, distribution, metabolism, and excretion profiles, further complicating direct comparisons between studies using different GnRH agonists.
This study provides crucial evidence affirming the diagnostic equivalence of IM and SC GnRH stimulation tests in girls with CPP. The finding that both routes achieve diagnostically significant peak LH levels within a remarkably similar and relatively short timeframe carries substantial practical implications. This suggests that the selection of the administration route can be flexibly determined by factors such as patient comfort, clinician expertise, and logistical convenience within a clinical setting, without compromising diagnostic accuracy or efficiency. While our study's design didn't include a direct assessment of patient comfort or preference between the 2 routes, the expedited diagnostic window for both routes, coupled with the inherent simplicity of IM injection, could significantly enhance the overall patient experience.
Several limitations must be acknowledged. First, the study was unblinded due to the visible nature of the injection technique. Second, we did not include a healthy control group due to ethical constraints regarding stimulation testing in healthy children. Third, while we hypothesized improved convenience, we did not utilize a validated scale to measure patient pain or comfort. Finally, a subset of patients met diagnostic criteria based on basal LH levels alone; however, our sub-analysis confirms that the stimulated profile remains comparable between groups for those requiring dynamic testing.
For diagnosing CPP in girls, both IM and SC GnRH stimulation tests demonstrate comparable LH response patterns and diagnostic timing. Clinicians can use either method with confidence to get accurate diagnostic results, as both are equally effective at prompting the necessary hormonal responses.
Supplementary material
Supplementary Table 1 is available at https://doi.org/10.3345/cep.2026.00052.
Mean FSH levels following the GnRHa stimulation test
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was funded by the Ratchadapisek Sompot Fund of Chulalongkorn University, Bangkok, Thailand (GA 67/061).
Acknowledgments
The authors extend their gratitude to the patients and their families who participated in this study, contributing invaluable data for the advancement of our understanding of CPP diagnosis. We also express our appreciation to the healthcare professionals at the pediatric endocrinology clinic of King Chulalongkorn Memorial Hospital for their dedicated care and assistance in the collection of essential data.
Author contribution
Conceptualization: SW, KS; Data curation: WL; Formal analysis: VS, KS; Funding acquisition: KS; Methodology: WL; Project administration: KS; Visualization: SW, VS; Writing - original draft: WL; Writing - review & editing: KS