Dietary fiber in pediatric gastrointestinal health: a narrative review of evidence and challenges
Article information

Abstract
Dietary fiber plays a central role in pediatric gastrointestinal health; however, most children worldwide consume amounts well below recommended levels. Current pediatric guidelines from the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (2014) and global nutrition guidance from the World Health Organization recommend adequate dietary fiber intake as part of a balanced diet to support digestive health and prevent noncommunicable diseases. These recommendations generally correspond to daily fiber intake levels of approximately 14–31 g/day, or the practical rule of age (years) + 5 g/day for children, yet more than 80%–90% of children fail to meet these targets. This shortfall is clinically significant, as inadequate fiber intake is associated with increased risk of functional constipation, a condition affecting approximately 3%–29% of children globally. Dietary fiber contributes not only to stool bulk but also to the modulation of gut microbiota, gastrointestinal barrier function, and immune and metabolic pathways during critical developmental stages. Among common pediatric gastrointestinal disorders, the strongest evidence supports fiber use in constipation management, where supplementation or increased intake through whole foods has been shown to improve stool frequency and consistency in approximately 50%–60% of affected children. However, clinical trial outcomes remain inconsistent, varying according to fiber type, dosage, duration of intervention, and diagnostic criteria. Evidence for recurrent or functional abdominal pain remains limited and heterogeneous, with small sample sizes, differing endpoints, and high placebo response rates complicating interpretation. In pediatric inflammatory bowel disease, fermentable fibers have been shown to enhance short-chain fatty acid production. Nevertheless, robust pediatric clinical evidence remains insufficient, and findings from adult ulcerative colitis studies cannot be directly extrapolated to children. Dietary fiber represents an important supportive component of pediatric gastrointestinal management, but standardized dosing recommendations and high-quality pediatric clinical trials are still needed to establish evidence-based guidelines for clinical practice.
Key message
Dietary fiber plays a critical role in pediatric gastrointestinal health by modulating gut microbiota, improving bowel function, and supporting immune development. Evidence consistently supports its benefit in functional constipation, while effects on abdominal pain, inflammatory bowel disease, and irritable bowel syndrome remain variable due to differences in fiber type, dosage, and study design. Clinically, fiber should be used as an adjunct therapy within individualized dietary and behavioral management strategies for children.
Graphical abstract. SCFA, short-chain fatty acid; ATP, adenosine triphosphate; DC, dendritic cell; pDC, plasmacytoid DC; sIgA, secretory immunoglobulin A; IFN, interferon; TNF, tumor necrosis factor; IL, interleukin; Th1, T helper cell type 1; Tfh, follicular helper T cell; IgM, immunoglobulin M; IgG, immunoglobulin G; IgA, immunoglobulin A; GI, gastrointestinal.
Introduction
Dietary fiber is a vital part of a balanced diet and plays an important role in supporting overall health, making it essential for inclusion in the meals of children just as with other key nutrients. These fibers, whether fermented or not, serve a variety of physiological purposes in the host and should not merely be thought of as bulking material or indigestible food components [1]. Dietary fiber acts as a primary energy source for the gut microbiome, a complex community of microorganisms residing in the gastrointestinal tract [2]. When fiber is fermented by these microbes, it produces a range of bioactive compounds that deliver both immediate and prolonged effect in the host. These effects extend beyond digestive health to influence the immune system and organs such as the liver, kidneys, and brain. In the short term, adequate fiber intake helps maintain a healthy gut immune response and can reduce the risk or severity of autoimmune and inflammatory conditions, including inflammatory arthritis, gastrointestinal disorders, and allergies. Over the long term, a fiber-rich diet is linked to a lower likelihood of developing chronic conditions such as obesity, type 2 diabetes, hypertension, stroke, and cardiovascular disease [3]. In contrast, insufficient fiber consumption in children has been associated with issues such as constipation, irritable bowel syndrome (IBS), allergies, and immune disorders.
Childhood obesity and other diet-related chronic illnesses remain highly prevalent across many developed countries including those in the United States and Europe imposing substantial health care costs and reducing quality of life. In the European region, for example, about one in 3 children aged 7–9 is overweight or obese, and roughly 10% are classified as obese [4]. While the protective effects of dietary fiber against chronic disease in adults are well-documented, relatively little research has examined its potential role in pediatric health. In children from high-income countries, low-fiber intake has also been associated with functional constipation a common condition that has been reported with prevalence rates of about 8%–11% in European populations [5]. Chronic constipation in turn can severely impact quality of life, daily functioning, and academic performance in children, thereby further underscoring the importance of investigating dietary fiber’s role in promoting child health across developed settings.
Determining appropriate dietary fiber recommendations remains a complex challenge, as the physiological effects of different fiber types and their functional properties are still being clarified. Although Dietary Reference Intake guidelines provide detailed considerations regarding fiber sources and health impacts, these recommendations are largely derived from adult data and extrapolated to children, without clear distinctions between dietary and functional fiber requirements for achieving specific health outcomes [6]. Importantly, inadequate fiber intake among children is not confined to the United States but represents a widespread concern across developed nations, including Europe and other high-income regions, where national nutrition surveys consistently report fiber intakes well below recommended levels in children and adolescents [7]. Similar trends have also been observed in several middle-income and non-Western countries, such as Brazil and parts of the Middle East, indicating that suboptimal fiber consumption among children is a global issue rather than one restricted to Western dietary patterns. Collectively, these findings suggest that the primary challenge lies less in defining optimal fiber type and more in the pervasive underconsumption of fiber-rich foods during childhood, a pattern that persists across diverse socioeconomic and geographic contexts [8]. In spite of advancement in understanding chemistry of fibers and the role of gut microbiome in the recent years, the information on the functional nexus of dietary fiber, gut microbiome, immune modulation, and clinical outcomes in children remain poorly understood [9].
The objective of this review is to provide a critical assessment of the role of dietary fibers in shaping pediatric gastrointestinal, metabolic, and immunological health, with a particular focus on their capacity to modulate gut microbiota composition, enhance short-chain fatty acid production, and strengthen intestinal barrier integrity. This review synthesizes current global recommendations for dietary fiber intake in healthy children, evaluates evidence supporting fiber-based interventions across common pediatric gastrointestinal disorders, and integrates mechanistic and clinical findings to elucidate how different fiber types and doses influence health outcomes. By highlighting inconsistencies in existing guidelines and identifying key gaps in fiber-specific dosing, mechanistic understanding, and pediatric clinical evidence, this review aims to clarify current limitations and outline priorities for future research in fiberbased pediatric nutrition.
Current scenario on dietary fiber intake in children
Worldwide, children's consumption of dietary fiber is well below the recommended level, with regional patterns influenced by culture, economics, and nutritional changes. In Asian nations, for example, a meta-analysis found nearly 30% of children experience constipation, and fiber consumption is often below the age-plus-5-gram standard [9]. Hong Kong's preschool population was reported to have an average intake of 4.1 g/day, which is just 45% of the recommended daily allowance, with even lower fiber consumption in constipated children compared to their non-constipated counterparts [9]. A Japanese study of more than 5,600 school children associated increased dietary fiber intake with a lower risk of overweight and hypercholesterolemia. Within the Pan-American region, the dietary transition to ultraprocessed, low-fiber foods has produced troubling outcomes. A national survey of more than 71,000 teenagers in Brazil revealed that merely 13.1% of them achieved the fiber intake recommendation, and overweight teenagers were substantially more likely to consume too little fiber. Also, children with chronic constipation consumed significantly less total and insoluble fiber, making them more than 4 times as at risk for functional gastrointestinal disorders [10]. Such nutrient deficiencies are further exacerbated by inadequate access to whole foods and the growing trend towards more refined carbohydrates and sweet drinks [11]. In Europe and Central Asia, the same issues exist. Although certain Nordic nations have mounted effective public health interventions to enhance infant and earlylife nutrition, national surveys indicate that most children continue to fail to meet daily fiber intakes, particularly from insoluble sources [12]. In Finland, for instance, cereal grains and vegetables continue as key sources of dietary fiber, but consumption levels are strongly determined by parental education and socioeconomic status. A review from across Europe highlighted the absence of specially designed fiber education and expertise of standardized guidelines for pediatrics, which made policy development and intervention challenging [11].
Intervention studies have aimed at enhancing fiber consumption among children either by dietary behavior change or the consumption of high-fiber foods to address functional bowel disorders and improve gastrointestinal health [5,13]. One randomized behavioral trial, based on a formal self-monitoring and reward system, allowed children with chronic constipation to substantially improve their fiber intake within 3 months versus regular dietary advice. A broad systematic review and metaanalytic assessment of 9 pediatric trials (n=680 children) revealed variable results in studies on fiber-based dietary interventions. Some participants reported better stool consistency, frequency of evacuation, and reduction in abdominal pain, whereas others had no statistically significant improvements over control interventions; the inconsistency reiterates the importance of individualized use and better trial design. Furthermore, school-based interventions have shown that stepwise addition of fiber-containing snacks to children's food raises daily fiber consumption by 2–3 g effectively, with high acceptance among school-aged children and no negative effect on gastrointestinal outcomes [14]. Such approaches imply that repeated exposure to fiber-containing foods in a supportive context, combined with behavior reinforcement and meal planning, enabled long term improvements in routine intake [15]. Together, these strategies represent a practical and child-friendly method focusing on increasing total fiber intake gradually and rewarding good eating habits rather than using prescription laxatives, thus encouraging long term regularity of the gut and general health. The recommended amount of dietary fiber and actual consumption among children in different countries is presented in Table 1. In preschool populations, average intake has been reported as low as 4.1 g/day, significantly below the recommended 9–11 g/day for children aged 2–4 years [16]. Low-fiber intake is strongly associated with gastrointestinal disorders in children. Epidemiological studies indicate that children consuming less than 10 g/day of dietary fiber have a fourfold increased risk of functional constipation compared with children recommended intake levels [17]. School-based nutritional interventions have demonstrated that gradual increases in dietary fiber by 2–3 g/day can significantly improve bowel frequency and stool consistency within 8–12 weeks, highlighting the effectiveness of modest dietary modifications in pediatric populations [18].
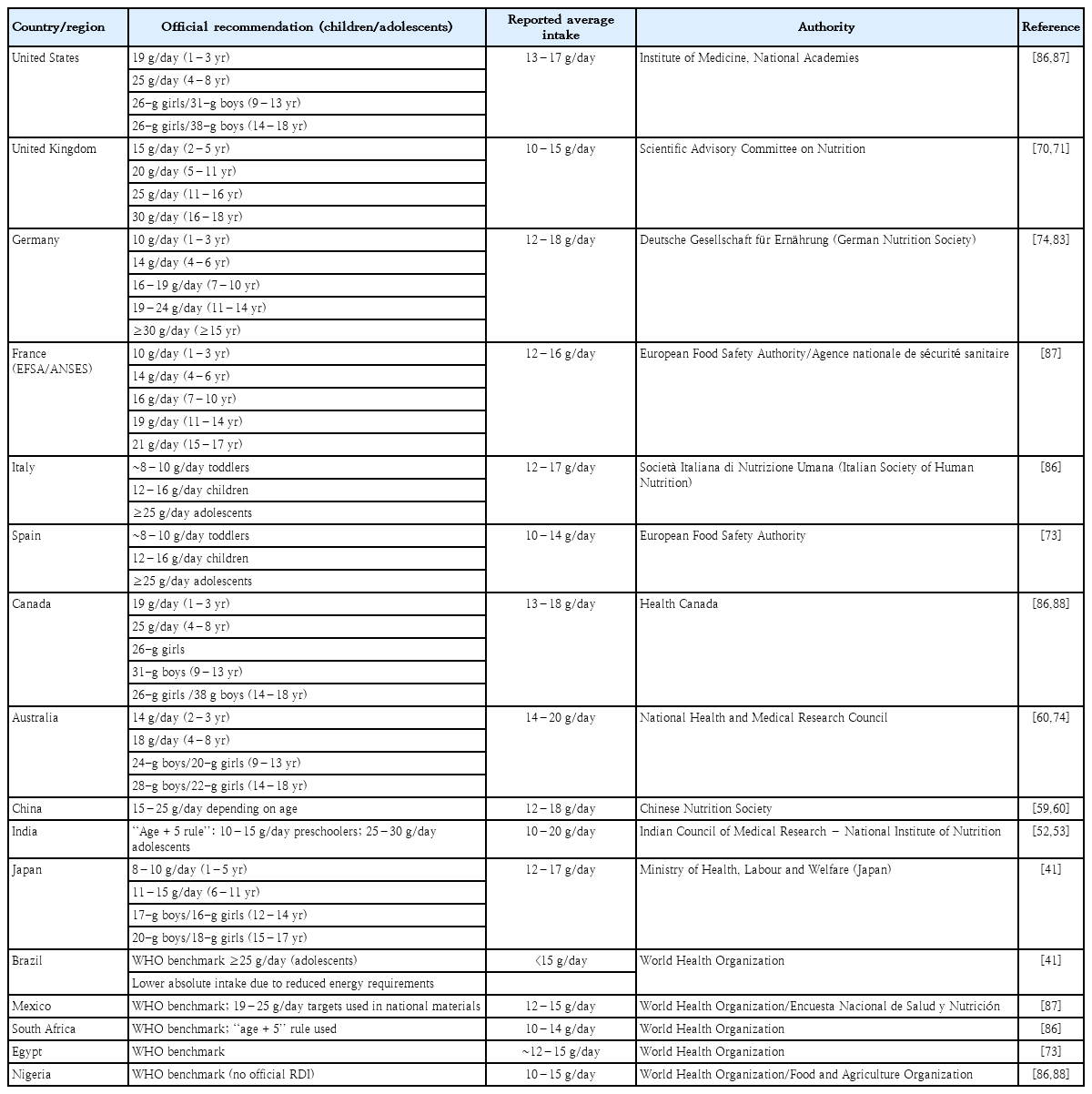
Dietary fiber recommendations and average intakes in children and adolescents across selected countries/regions
Types of fiber
The recognition of fiber-rich foods by Hippocrates and Galen in promoting digestive health was later reinforced by 19th century nutrition science [19]. The term dietary fiber was introduced in the mid-20th century to describe indigestible plant components. Dietary fiber comprises a heterogeneous group of nondigestible carbohydrates and related compounds, including nonstarch polysaccharides, resistant starches, lignin, and oligosaccharides, occurring naturally in plant-based foods or obtained through extraction or synthesis. According to Codex Alimentarius, dietary fibers resist digestion in the small intestine and reach the colon, where they may be fermented by gut microbiota, contributing to stool bulk, intestinal motility, and other physiological benefits [20]. Certain fibers, such as inulin, fructooligosaccharides (FOS), and galactooligosaccharides (GOS), also function as prebiotics by selectively stimulating beneficial gut microorganisms (Fig. 1).
Classification and dietary sources of dietary fibers. Schematic representation of the major classes of dietary fibers and their food sources. Dietary fibers are broadly categorized into noncarbohydrate components (e.g., lignin, phytate, chitin), modified resistant starches and synthetic components (e.g., maltodextrin, RS4 starch, highamylose maize starch), nonstarch polysaccharides (including insoluble fibers such as cellulose and hemicellulose, and soluble fibers such as β-glucans, pectin, glucomannan, galactomannan, mucilage, and gums), resistant oligosaccharides (prebiotics) (e.g., fructo-oligosaccharides, inulin, galacto-oligosaccharides, xylo-oligosaccharides), and resistant starch and dextrin. Representative plant-based dietary sources and molecular structures of selected fiber components are illustrated.
1. Soluble dietary fiber
Soluble fibers dissolve in water and can improve cholesterol levels and postprandial blood glucose by increasing viscosity, delaying gastric emptying, and slowing nutrient digestion [21]. Viscosity depends on polymer length and molecular weight, meaning not all soluble fibers are viscous [22]. Certain nonviscous fibers, such as inulin-type fructans and resistant maltodextrin, also improve lipid and glucose profiles. Fermentation rates vary depending on fiber source, processing, and food combinations [23,24].
Oligosaccharides (3–20 sugar units) such as GOS, FOS, and xylooligosaccharides (XOS) resist digestion in the small intestine and function as prebiotics by selectively stimulating beneficial bacteria like bifidobacteria [25]. Fructans, including inulin and oligofructose, are β(2–1)-linked fructose polymers naturally found in plants, with shorter-chain fructans fermenting more rapidly than longer-chain forms, while FOS can also be produced enzymatically from sucrose [26]. GOS is generally obtained via enzymatic hydrolysis of lactose. Resistant starch, either soluble or insoluble, also acts as a fermentable fiber, with fermentability influenced by gut microbiota composition; corn fiber, a soluble resistant starch with mixed α-linkages, is produced by enzymatic hydrolysis of corn starch and resists digestion in the small intestine.
Wheat bran, high in insoluble arabinoxylans and cellulose, also contains proteins, lignin, and micronutrients, and supplementation with wheat bran oligosaccharides has been shown to increase bifidobacteria and reduce harmful protein fermentation byproducts in children. Soluble dietary fiber is a hydrophilic component of plant foods that forms gel-like viscous solutions in the gut, slowing gastric emptying and nutrient absorption, which helps regulate blood cholesterol and glucose levels while increasing satiety [27]. It is extensively fermented by gut microbiota, leading to the production of short-chain fatty acids (SCFAs) that nourish colonocytes, modulate immune responses, and enhance the integrity of the gut barrier. The fermentation process favors beneficial bacteria such as bifidobacteria, Faecalibacterium, and Akkermansia, enriching microbiota diversity and contributing to the prevention of metabolic and inflammatory disorders [28]. In pediatric populations, the physiological tolerance of dietary fiber varies with age, gastrointestinal maturity, and hydration status. Clinical pediatric guidelines recommend gradual increases in fiber intake of approximately 2–5 g/day increments to minimize gastrointestinal discomfort such as bloating or abdominal pain. For children aged 1–3 years, recommended fiber intake ranges from 19 g/day, increasing to 25–31 g/day for children aged 4–13 years, depending on sex and energy requirements. Excessive fiber intake without adequate fluid consumption may lead to reduced nutrient absorption and poor weight gain in young children, particularly in those under 2 years of age, emphasizing the need for balanced dietary planning in pediatric clinical practice [29].
2. Insoluble dietary fiber
Insoluble fibers resist fermentation, increase stool bulk, and accelerate transit [30]. While lignin and chitin have no direct microbiota effects, some cellulose, hemicellulose, xyloglucans, and resistant starches may have prebiotic potential when processed. In children, these fibers promote gut motility, prevent constipation, and may lower the risk of developing diverticular changes later in life. By adding bulk to the stool and enhancing bowel regularity, they support overall gastrointestinal function and contribute to healthy weight management. Regular intake of insoluble fiber during childhood helps establish beneficial bowel habits and fosters a balanced gut microbiome, which is essential for long term digestive health. Healthy bowel habits that may last into adulthood are also established by adequate intake during childhood [31].
Lignin and chitin are insoluble, noncarbohydrate component of dietary fiber found in seeds, grains and certain vegetables. In children, lignin contributes to stool bulk and supports bowel regularity, indirectly aiding gut health. Its antioxidant properties may also support immune function and overall well-being. While lignin itself is gluten-free, some lignin-rich foods (e.g., rye) contain gluten and should be avoided in children with celiac disease or gluten intolerance. Early dietary exposure to lignin-rich plant foods can help establish a diverse and resilient gut microbiome, promoting digestive health throughout life [32].
XOS are nondigestible carbohydrates materials that act as selective prebiotics, promoting the growth of beneficial gut bacteria, particularly Bifidobacterium and Lactobacillus, while inhibiting potential pathogens. Their fermentation in the colon leads to the formation of SCFAs that support intestinal health barrier integrity, modulate immune function, and may reduce the risk of gastrointestinal infections. Compared to other prebiotics, XOS are effective at relatively low doses and are well tolerated, making them a promising dietary intervention to enhance gut health in children.
Xylitol is a naturally occurring sugar alcohol found in small amounts in fruits and vegetables and widely used as a sweetener. In children, xylitol has notable oral health benefits, as it inhibits the growth of Streptococcus mutans, the primary bacteria responsible for dental caries. At moderate intakes, xylitol may also have mild prebiotic effects by stimulating beneficial gut bacteria such as Bifidobacterium [33].
Gut microbiota modulation on consumption of dietary fiber
Dietary fibers that are resistant to small intestinal digestion regulate gut health by shaping microbiota composition, function, and metabolism. Delivered to the colon as microbiota-accessible carbohydrates [34,35], they undergo fermentation to yield SCFAs like acetate, propionate, and butyrate [36,37]. Different dietary fibers promote distinct microbial consortia and SCFA profiles (Table 2).
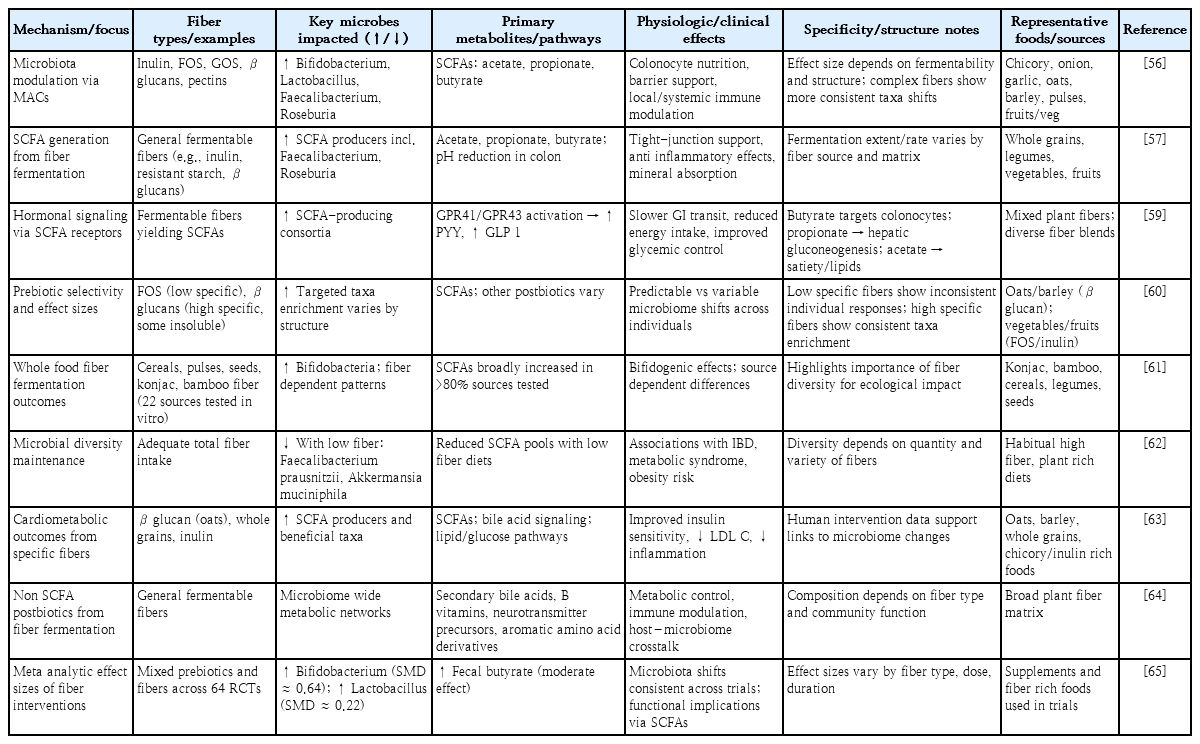
Impact of dietary fibers on gut microbiota, metabolite production, and health outcomes in children
Dietary fibers selectively stimulate beneficial intestinal microbes. Inulin-type fructans, are fermented by bifidobacteria, in the colon which additionally promotes butyrate-producing microbes, referred to as the butyrogenic effect. Gut microbiota is dependent on one another through cross-feeding. For instance, fermentation of beta-fructans by Bifidobacterium leads to the production of acetate and lactate while acetate and lactate in turn are converted into butyrate by Eubacterium hallii. Anaerostipes caccae ferments the acetate and fructose that Bifidobacterium longum produces during substrate breakdown in a mixed culture [38].
The kind of fermentable carbohydrate and the species of butyrate-producing bacteria can affect how quickly acetate-consumers (such as Faecalibacterium prausnitzii and Roseburia intestinalis) produce butyrate [39].
Apart from inulin-type fructans, resistant starch fermentation also exhibits the butyrogenic action. Studies conducted in vitro on germinated barley have demonstrated effective butyrate synthesis in a coculture of B. longum and Eubacterium limosum. Since lactate was previously created by B. longum during starch breakdown, E. limosum uses lactate for butyrate production by cross-feeding. Roseburia intestinalis first aids in the breakdown of xylan by producing hydrogen and carbon dioxide, which act as substrates for the growth of Ruminococcus hydrogenotrophicus in addition to acetate. Afterwards, this SCFA serves as a crucial co-substrate for the synthesis of butyrate [40].
Acetate, propionate, and butyrate are key SCFAs generated by microbial fermentation of fiber in the colon and represent a major mechanistic link between diet, gut microbiota, and host health [41]. Human studies have consistently shown that SCFAs exert multiple beneficial physiological effects by acting as both energy substrates and signaling molecules (Fig. 2A). Butyrate serves as the principal energy source for colonocytes, promoting epithelial cell differentiation, enhancing tight-junction protein expression, and maintaining intestinal barrier integrity, thereby reducing gut permeability [42]. Acetate and propionate enter systemic circulation and influence hepatic and peripheral metabolism, where they contribute to lipid and glucose homeostasis through activation of GPR41 and GPR43 and modulation of insulin sensitivity. SCFAs are also responsible for maintaining the local anaerobic environment at the gut epithelium which prevents overgrowth of facultative anaerobes.
Mechanisms of dietary fiber fermentation and gut–brain–immune interactions. (A) Dietary fibers derived from fruits, vegetables, and whole grains undergo fermentation by gut microbiota, leading to the production of short-chain fatty acids (SCFAs) such as acetate, propionate, and butyrate. SCFAs exert multiple beneficial effects, including enhancement of gut-barrier integrity, anti-inflammatory activity through down-regulation of proinflammatory cytokines, reduction of visceral hypersensitivity, modulation of mast cell activation, and regulation of gut motility. (B) SCFAs also influence the enteric nervous system and vagus nerve signaling, thereby linking the gut microbiota to central nervous system regulation. GPCR-LC, G protein-coupled receptor – like cell surface receptor; TLR, toll-like receptor; CLR, C-type lectin receptor; HDAC, histone deacetylase.
In pediatric populations, increased SCFA production resulting from fiber-rich diets has been associated with improved bowel function, reduced incidence of functional gastrointestinal disorders. These findings collectively support the premise that dietary fiber-driven modulation of the gut microbiota, via increased SCFA production, is a central mechanism through which positive health outcomes are achieved in children (Fig. 2B). Dietary fiber intake plays a central role in shaping the developing gut microbiota in children. Pediatric intervention studies have shown that supplementation with prebiotic fibers such as inulin or galacto-oligosaccharides can increase beneficial bacterial populations, including Bifidobacterium sp., by 1–2 log units within 2–4 weeks of intervention [43]. These microbial changes are associated with increased production of SCFAs, particularly butyrate, which contributes to improved intestinal barrier function and reduced gastrointestinal inflammation in children. Clinical studies further demonstrate that children consuming fiber-rich diets exhibit improved bowel movement frequency, increasing from approximately 2–3 bowel movements per week to 5–7 per week following dietary fiber supplementation, highlighting the functional significance of microbiotamediated fermentation processes in pediatric gastrointestinal health [44].
Immune modulation on consumption of dietary fiber
Dietary fibers influence host immunity both directly and indirectly (Fig. 3). Specific fibers such as GOS, inulin, pectin, and β-galactomannan enhance epithelial integrity by regulating tight-junction proteins, stimulating goblet cells, promoting epithelial growth, and supporting glycocalyx maturation. In vitro studies also show that inulin, GOS, FOS, and arabinoxylan hydrolysates affect cytokine and chemokine release from epithelial cells, macrophages, and dendritic cells, partly through activation of PPARγ [45]. Moreover, fibers can engage pattern recognition receptors (PRRs), including C-type lectin receptors (e.g., β-glucans), galectins, and toll-like receptors (TLRs) (mainly TLR2 and TLR4, e.g., GOS and FOS), on epithelial and innate immune cells [46]. Conversely, some fibers inhibit PRR signaling, as demonstrated by pectin blocking TLR2-mediated cytokine secretion. Notably, distinguishing true fiber–PRR interactions from contamination-driven effects remains a methodological challenge [47].
Immunomodulatory effects of dietary fiber-derived short-chain fatty acids (SCFAs). Fermentation of dietary fibers produces SCFAs that interact with host immune cells via G-proteincoupled receptors (GPR41 and GPR43) and histone deacetylase (HDAC) inhibition. SCFAs modulate innate immunity by influencing macrophages, tolerogenic dendritic cells, and natural killer (NK) cells, while promoting adaptive immune responses through increased regulatory T (Treg; FoxP3+) cells, enhanced immunoglobulin A (IgA) production, and suppression of proinflammatory Th1/Th17 responses. Additionally, SCFAs regulate key signaling pathways including NF-κB suppression and mTOR/AMPK signaling, contributing to immune homeostasis and intestinal health. NF-κB, nuclear factor-kappa B; mTOR/AMPK, mechanistic target of rapamycin/AMP-activated protein kinase.
SCFAs also regulate host immunity through G protein-coupled receptors (GPR41, GPR43, GPR109A), inhibition of histone deacetylases, and, in the case of butyrate, activation of the aryl hydrocarbon receptor (AhR) [48]. They modulate multiple immune functions: enhancing interleukin (IL)-10 secretion, supporting Treg differentiation, shaping hematopoiesis, dampening effector T-cell activity, improving barrier integrity, stimulating immunoglobulin A (IgA) responses, and suppressing mast cell and innate lymphoid cell activation. Acetate, via acetyl-CoA and the tricarboxylic acid cycle, can also drive IL-10–producing regulatory B cells. Dietary fiber consumption has been shown to influence immune development in children through modulation of gut microbiota and production of immunoregulatory metabolites. Clinical pediatric trials indicate that supplementation with prebiotic fibers such as galacto-oligosaccharides can increase secretory IgA levels by approximately 15%– 30% within 4–8 weeks, enhancing mucosal immunity and reducing susceptibility to gastrointestinal infections [49]. Furthermore, observational studies have reported that children consuming high-fiber diets exhibit a 20%–25% lower incidence of allergic and inflammatory conditions, including eczema and food allergies, compared with children consuming low-fiber diets [50]. These findings underscore the preventive role of dietary fiber in pediatric immune health.
Dietary fibers in gastrointestinal disorders in children
Gastrointestinal disorders in children broadly include conditions such as abdominal pain, bloating, altered bowel habits, diarrhea, constipation, and IBS, which affect the digestive tract and impair quality of life [51]. Dietary fibers have been proposed as a first-line, nonpharmacological intervention for managing constipation and other gastrointestinal symptoms in children. Several clinical studies have evaluated fiber supplementation in pediatric gastrointestinal disorders, showing improvements in stool frequency, stool consistency, and reduction of abdominal pain (Table 3).
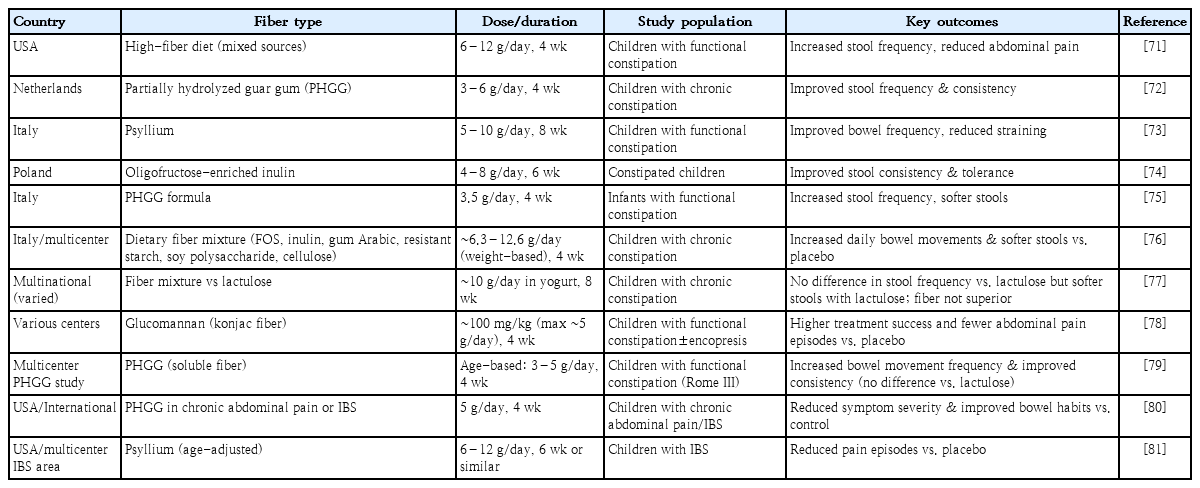
Fiber consumption and improvement in constipation among children
1. Constipation
Constipation is defined by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition and the Rome IV criteria as infrequent, difficult, or painful defecation, often associated with hard stools and incomplete evacuation. Functional constipation is one of the most common pediatric gastrointestinal disorders, affecting approximately 3%–29% of children globally and accounting for nearly 25% of pediatric gastroenterology consultations [52]. Symptoms frequently begin during infancy or early childhood, with up to 35%–52% of affected children experiencing persistent symptoms into adolescence [53]. Randomized controlled trials in pediatric populations have demonstrated that dietary fiber supplementation can significantly improve stool frequency and consistency. For example, supplementation with a combination of fermentable and nonfermentable fibers increased treatment success rates from 16.7% in control groups to 60% in intervention groups, representing a statistically significant improvement in bowel function [54].
In many children, symptoms begin during the first year of life and may persist long-term in approximately 35%–52% of cases. Dietary habits play an important role, as more than half of affected children consume less fiber than the recommended levels. Evidence from a small perspective trial showed that the children who consumed a high-fiber diet, including bran and exceeding the intake of age + 10 g/day, experienced resolution of constipation by the end of the study [55]. Notably, no difference in colonic transit time was detected, indicating that symptom improvement was not driven by accelerated intestinal motility. Instead, the beneficial effects are likely attributable to increased stool bulk, enhanced water retention, and microbial fermentation of fibers leading to shortchain fatty acid production, which collectively improve stool softness and promote more effective defecation [56]. Two systematic reviews in 2018 reported modest benefits of fiber in constipated children, but heterogeneity in study design, outcome definitions, and fiber types limited firm conclusions [57,58]. Across pediatric clinical trials, the magnitude of benefit from dietary fiber supplementation in constipation varies considerably depending on fiber type, dosage, and study design. Randomized controlled trials (RCTs) using glucomannan at doses of approximately 2–5 g/day have demonstrated significant increases in stool frequency from 2.1±0.6 bowel movements per week at baseline to 5.3±1.2 per week after 4 weeks of treatment, compared with minimal improvement in placebo groups [61]. Similarly, a controlled trial evaluating cocoa-husk fiber supplementation in children reported a reduction in colonic transit time by approximately 20– 25% and improvement in stool consistency scores within 2 weeks of intervention [59].
However, larger systematic reviews involving more than 690 pediatric patients across 10 randomized trials have reported only modest overall treatment effects, with pooled response rates ranging from 45% to 55%, indicating that dietary fiber alone does not resolve constipation in all children [60]. A key strength of randomized trials is their ability to minimize bias and provide standardized outcome measures, whereas observational studies often report higher treatment success rates due to uncontrolled confounding factors such as hydration status and behavioral interventions. Limitations across studies include small sample sizes (commonly n=30–80 participants), short intervention duration (typically 2–8 weeks), and variability in fiber composition. From a clinical perspective, the collective evidence suggests that dietary fiber supplementation improves bowel frequency and stool consistency in approximately 50%–60% of pediatric patients, but should be considered an adjunct therapy rather than a replacement for pharmacologic management in children with moderate to severe functional constipation.
A 2022 meta-analysis of 10 RCTs (690 children) assessed 7 fiber formulations: only one mixture (acacia fiber, psyllium, fructose) was as effective as a laxative [61], glucomannan was superior to placebo in one trial, while other mixtures, including FOS- or inulin-based supplements, did not show significant advantages [62]. A prospective trial of polydextrose (4.17 g) plus FOS (0.45 g) in 77 children reported marked reductions in constipation-related symptoms (hard stools, defecation pain, abdominal pain, and fear of defecation) but lacked a control group. Thus, fiber supplementation to the children with constipation does not overcome the symptoms completely rather improves the stool frequency at a modest level with inconsistent benefits across different outcomes.
2. Abdominal pain
Recurrent abdominal pain affects approximately 8%– 25% of school-aged children worldwide, making it one of the most prevalent functional gastrointestinal disorders in pediatric practice [63]. Clinical trials investigating dietary fiber supplementation have reported mixed outcomes. In one randomized pediatric study, consumption of 10 g/day corn fiber for 2 weeks reduced the frequency of abdominal pain episodes by approximately 50% compared with placebo [64]. However, subsequent meta-analyses involving more than 130 pediatric participants found no consistent reduction in pain frequency or severity across different fiber types, suggesting that treatment response varies depending on fiber composition, dosage, and individual patient characteristics [65]. The earliest trial investigating fiber for recurrent abdominal pain in children, defined by Apley’s criteria, was conducted in 1985 [66]. Nearly 3 decades later, a randomized trial in 2013 tested glucomannan for 4 weeks in 84 children with functional abdominal pain diagnosed by Rome III criteria, but no difference was observed compared with placebo. These divergent findings are biologically plausible when the heterogeneous physicochemical properties of dietary fibers are considered. Fibers differ markedly in solubility, viscosity, fermentability, and water-holding capacity, all of which influence gastrointestinal transit, luminal distension, and microbial fermentation [67]. In the same year, supplementation with partially hydrolyzed guar gum significantly lowered pain intensity compared to placebo (40% vs. 13%). A Cochrane review published in 2017 synthesized evidence from 4 RCTs on dietary fiber interventions for recurrent or functional abdominal pain in children, defined using Apley’s or Rome criteria [68]. The fibers tested included corn fiber, partially hydrolyzed guar gum, glucomannan, and psyllium (6–12 g/day). Pooled analysis showed no consistent benefit of fiber over placebo in reducing abdominal pain frequency (odds ratio [OR], 1.83; 95% confidence interval [CI], 0.92– 3.65; 2 trials, 136 participants) or intensity (standardized mean difference, -1.24; 95% CI, -3.41 to 0.94; 2 trials, 135 participants). The quality of evidence was rated as low due to methodological bias, imprecision, and high heterogeneity [69]. The inconsistent results likely arise from substantial heterogeneity among studies, including differences in diagnostic criteria (Apley vs. Rome), fiber type and fermentability, dosage, and duration of intervention. Comparative analysis of pediatric trials indicates that treatment outcomes vary substantially according to study methodology and patient selection criteria. Early exploratory studies using corn fiber supplementation at doses of approximately 10 g/day reported reductions in abdominal pain frequency by nearly 50% within 2 weeks, whereas more recent randomized placebo-controlled trials evaluating glucomannan at doses of 2.5 g twice daily showed no statistically significant improvement in pain intensity scores after 4 weeks of treatment [70]. These discrepancies likely reflect differences in sample size, placebo response, and diagnostic criteria. A strength of recent pediatric trials is the use of standardized diagnostic frameworks such as the Rome III and Rome IV criteria, which improve reproducibility and reduce diagnostic variability. However, limitations include high placebo response rates ranging from 30% to 60%, short follow-up periods, and reliance on subjective symptom reporting rather than objective biomarkers. Meta-analytic evidence involving approximately 136 pediatric participants across multiple trials demonstrates inconsistent treatment effects, with pooled odds ratios for symptom improvement ranging from 0.92 to 1.83, indicating uncertain clinical benefit [71]. Clinically, these findings suggest that dietary fiber may be beneficial in selected children, particularly those with constipation-associated abdominal pain, but routine use for all cases of functional abdominal pain cannot be universally recommended without individualized assessment.
Fibers vary markedly in their physicochemical properties and effects on gut microbiota and fermentation, which can influence symptom response. Additionally, small sample sizes and methodological limitations reduce statistical power and contribute to variability in outcomes. Importantly, most pediatric trials did not assess mechanistic endpoints such as changes in gut microbiota composition, SCFA production, intestinal permeability, or markers of neuroimmune activation, limiting causal interpretation. Collectively, current evidence suggests that abdominal pain relief observed in some fiber interventions is likely mediated through microbiota-dependent fermentation, modulation of gut–brain signaling, and reduction of visceral hypersensitivity rather than through a uniform “fiber effect.” The absence of fiber-specific dosing frameworks, mechanistic stratification, and adequately powered pediatric trials remains a critical barrier to translating these findings into evidencebased clinical recommendations.
3. Inflammatory bowel disease
Inflammatory bowel disease (IBD) in children is a chronic disorder characterized by inflammation of the gastrointestinal tract, primarily presenting as Crohn disease and ulcerative colitis. Core symptoms in children include recurring abdominal pain, diarrhea (often with blood), weight loss, decreased appetite, fatigue, growth failure, and various extraintestinal manifestations such as joint pain, skin rashes, and liver issues. IBD can significantly impact nutritional status and overall development, with some children facing delayed growth or puberty [72].
The prevalence of pediatric IBD has increased substantially worldwide over the past few decades. The increase has been most pronounced in high socio-demographic index regions, including Canada and Northern Europe. In these regions, annual incidence rates have reached approximately 19.9 cases per 100,000 children, compared with fewer than 1 case per 100,000 children in low-income countries [73]. Dietary fiber intake may play a protective role in pediatric IBD by enhancing gut-barrier function and increasing production of antiinflammatory metabolites such as butyrate. Observational studies indicate that children with higher fruit and vegetable intake have a 30%–40% lower risk of developing ulcerative colitis, supporting the role of fiber-rich diets in disease prevention [74].
The underlying causes of IBD in children involve a multifactorial interaction involving genetic susceptibility, immune imbalance, and environmental influence, dietary patterns, and possibly alterations in gut microbiota. Long term investigations in Europe established that a westernized diet (high-fat, high-sugar, low fruit and vegetables) increases the risk of IBD whereas a diet high in poly-unsaturated fatty acids, fruit and vegetables is associated with decreased risk of IBD [75]. Furthermore, dietary fiber along with other components of fruits and vegetables are important in reducing the risk factor of IBD.
Evidence on dietary fiber use in IBD remains limited, particularly in children. Comparative evaluation of dietary fiber interventions in IBD reveals substantial variation in outcomes across studies due to differences in disease severity, fiber formulation, and study population. In adult randomized trials, supplementation with inulin at doses ranging from 10 to 15 g/day has been associated with reductions in fecal calprotectin concentrations by approximately 20%–40% and improvement in clinical disease activity scores in patients with mild ulcerative colitis [76]. However, pediatric evidence remains limited, with most studies involving small cohorts of fewer than 50 participants and short follow-up durations of 4–12 weeks. A key strength of adult trials is the use of objective inflammatory markers, including fecal calprotectin and C-reactive protein, which provide measurable indicators of disease activity [77]. In contrast, pediatric studies frequently rely on symptom-based assessments, limiting the ability to establish causal relationships between dietary fiber intake and disease remission. Additionally, differences in growth requirements, nutritional status, and immune development between children and adults may influence treatment response. From a clinical standpoint, current evidence supports maintaining moderate dietary fiber intake in children with stable IBD to support microbiota diversity and intestinal barrier function. However, individualized dietary adjustments remain essential during active disease or in children with structuring complications [78].
Many patients restrict fiber during active disease due to concerns about symptom worsening, yet fibers may offer benefits by enhancing gut-barrier function, restoring the mucus layer, modulating dysbiosis, increasing SCFAs (notably butyrate), and reducing inflammation. Polyphenols from fruits, vegetables, legumes, nuts, and whole grains may further support gut microbiota and attenuate inflammatory pathways. Observational studies suggest high fruit intake lowers the likelihood of developing ulcerative colitis as well as Crohn’s disease, while vegetable intake appears protective only for ulcerative colitis [79].However, fiber responses can vary by microbiota composition, with some individuals showing proinflammatory effects. A European pediatric consensus advises against routine fiber restriction in children with IBD unless structuring disease or fiber intolerance is present. A systematic review of 8 RCTs in adults assessed 5 fiber types [80]. Prebiotic reduced proinflammatory cytokines and disease activity in ulcerative colitis. Psyllium seed husk (Plantago ovata) improved symptoms but not significantly more than placebo. Wheat bran with psyllium altered microbiota without affecting stool bulk, while wheat bran with resistant starch showed no clinical benefit. Psyllium seeds increased butyrate production but did not prolong remission. Inulin reduced dyspeptic symptoms and fecal calprotectin in mild to moderate colitis but had no effect on quality of life or disease activity. In Crohn disease, FOSs failed to improve activity or biomarkers and were linked to lower quality of life. Only one trial was judged at low risk of bias [81].
4. Irritable bowel syndrome
IBS is a frequently observed functional gastrointestinal condition in children, marked by repeated episodes of abdominal discomfort accompanied by changes in bowel patterns, including constipation, diarrhea, or a combination of both. Under the Rome IV guidelines, pediatric IBS is diagnosed when a child experiences abdominal pain on at least 4 days per month over a minimum period of 2 months, with the pain being related to bowel movements or accompanied by alterations in stool frequency or consistency, and without evidence of any other underlying medical disorder [82]. IBS significantly affects quality of life, schooling, and healthcare costs in children. The global prevalence of pediatric IBS varies widely due to cultural and diagnostic differences. IBS affects approximately 8.8% of children globally, with higher prevalence reported in Asian populations reaching 12.4%, reflecting regional differences in dietary habits and diagnostic criteria. Pediatric IBS significantly impacts quality of life, contributing to increased school absenteeism and healthcare utilization. Clinical trials evaluating fiber supplementation in pediatric IBS have demonstrated moderate therapeutic benefit. A RCT involving children aged 7–18 years reported that supplementation with psyllium at doses of 6–12 g/day significantly reduced abdominal pain frequency and severity compared with placebo over an 8-week treatment period [83]. These findings support the role of soluble fiber as an adjunctive therapy in pediatric IBS management. A meta-analysis of studies from 1957–2014 reported a prevalence of 8.8% among children, with higher rates noted in Asia (12.4%). Country-specific studies report prevalence rates such as 13.25% in China, 16% in Nigeria, and 22.6% in Turkey, whereas lower prevalence was observed in the United States (2.8%–5.1%) and Mediterranean region (4%). Subtype distribution also varies, with IBS-C (constipation-predominant) being most common in Europe, while IBS-M (mixed) is more frequent in Greece and Nigeria [84]. The exact cause of IBS in children remains unclear; however, it is widely believed to arise from an interplay of biological, psychological, and environmental factors [85]. Dietary fiber is helpful for many individuals with IBS but not in all cases. Differences in treatment outcomes across pediatric studies are largely attributable to variation in IBS subtype, fiber solubility, and dosing strategies. RCTs evaluating soluble fibers such as psyllium have reported more consistent symptom improvement compared with studies using insoluble fibers. For example, a placebo-controlled trial involving children aged 7–18 years demonstrated a reduction in abdominal pain episodes from approximately 3–4 episodes per week at baseline to 1–2 episodes per week after 8 weeks of psyllium supplementation at doses of 6–12 g/day [86]. In contrast, studies using insoluble fiber supplementation have reported inconsistent results, with some children experiencing increased bloating or abdominal discomfort. A methodological strength of recent pediatric IBS trials is the use of standardized symptom scoring systems and controlled study designs [87]. However, limitations include small sample sizes, short intervention periods, and variability in dietary adherence. Clinically, soluble fiber supplementation may be considered an appropriate first-line dietary intervention for children with constipation-predominant IBS, while careful monitoring is recommended in diarrhea-predominant cases to prevent symptom exacerbation.
Its beneficial effect has been dependent on the type of IBS, fiber type and the dose. Soluble, gel forming fiber like psyllium and inulin has been useful in individuals in IBS-C. Its effect is mediated by consistency, frequency and softening of stool. While in patients with IBS-D, more soluble fiber like psyllium and less insoluble fiber was able to able to reduce the intestinal transit and improve the stool consistency. Decreasing the FODMAP diet reduces abdominal pain, gas formation and diarrhea by reducing the availability of easily fermentable carbohydrates in the intestine. Though these studies has been based on adult patients, Menon et al. [88] reported that psyllium reduces the symptoms of IBS in children, particularly by decreasing the occurrences and intensity of abdominal pain, compared with placebo.
Future perspective
Although significant mechanisms of dietary fibers in pediatric health, important gaps remain that call for further research. Future studies should adopt personalized nutrition approaches that account for differences in gut microbiota, genetics, and diet among children, while also exploring novel fiber sources such as seaweed polysaccharides, bamboo shoot fibers, resistant starches, and engineered prebiotic blends. Integrating multiomics technologies, including metagenomics, metabolomics, and transcriptomics, will help unravel the mechanistic pathways through which fibers modulate microbial metabolism, immune responses, and growth outcomes. Longitudinal and multicenter pediatric trials are essential to implications of fiber intake on growth, cognition, immunity, and chronic disease prevention, while also clarifying their therapeutic potential in conditions such as obesity comorbidities. At a global level, harmonizing dietary recommendations for fiber intake in children and translating scientific evidence into practical applications such as culturally acceptable, child-friendly fiber-rich foods, school meal programs, and functional products will be crucial to optimizing fiber consumption and promoting lifelong health benefits.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contribution
Conceptualization: BT; Writing – original draft: RD, BT; Writing – review and editing: RD, BT.