Update on pediatric allergic rhinitis: narrative review based on guideline updates
Article information

Abstract
Pediatric allergic rhinitis, among the most common chronic allergic diseases in children and adolescents, represents a significant public health burden in Korea and other countries. Allergic rhinitis in childhood is closely associated with asthma and should be considered a unified airway disease requiring integrated management. Recent Allergic Rhinitis and its Impact on Asthma and Korean Academy of Asthma, Allergy and Clinical Immunology guidelines advocate an evidence-based control-oriented stepwise treatment strategy that incorporates a patient-centered approach that is supported by both randomized trial data and real-world evidence. Intranasal corticosteroids (INCS) remain the first-line treatment for moderate to severe pediatric allergic rhinitis, whereas INCS plus intranasal antihistamine (INAH) combination therapy is recommended when symptom control is inadequate with INCS alone. Oral antihistamines (OAH) and INAH are recommended for children with mild disease or when rapid symptom relief is required. However, the addition of OAH to INCS therapy does not confer clinically meaningful additional benefits compared with INCS monotherapy in most patients with allergic rhinitis; therefore, routine combination therapy is not recommended. Leukotriene receptor antagonists are not recommended as first-line therapy for allergic rhinitis and are mainly used as add-on therapy in patients with concomitant asthma. In patients with predictable seasonal allergic rhinitis, INCS may be initiated 1–2 weeks before the anticipated pollen season to optimize symptom control. Pediatric management requires special consideration of age-specific clinical features, treatment adherence, safety, and caregiver education. The early diagnosis and guideline-based treatment of allergic rhinitis in children may improve their quality of life and reduce long-term respiratory morbidity.
Key message
Intranasal corticosteroids remain the cornerstone treatment for moderate to severe allergic rhinitis. The 2024–2025 Allergic Rhinitis and its Impact on Asthma guideline update suggests that fixed intranasal antihistamine–intranasal corticosteroid combinations may provide greater symptom control in allergic rhinitis than either agent alone. A control-based patient-centered approach that incorporates real-world evidence is essential for optimizing treatment outcomes in children.
Graphical abstract. ARIA, Allergic Rhinitis and its Impact on Asthma.
Introduction
Allergic rhinitis (AR), among the most common chronic inflammatory diseases in childhood, requires early recognition and long-term management and represents a major global health burden in pediatric populations. AR affects approximately 30%–40% of school-aged children in South Korea [1]. The prevalence of pediatric AR has increased over recent decades, particularly in urbanized regions, and is primarily driven by the enhanced exposure to environmental allergens amplified by climate change and air pollution, which act synergistically to promote allergen sensitization, airway inflammation, and disease persistence. AR significantly impacts quality of life, sleep quality, and school performance as well as childhood behavior and development. Pediatric AR often coexists with asthma, atopic dermatitis, and other allergic diseases, and its presence increases a child's risk of asthma development and poor control.
The Allergic Rhinitis and its Impact on Asthma (ARIA) initiative has played a central role in our understanding and management of AR. The ARIA guidelines have undergone several revisions since the original 2001 document and incorporate evidence-based recommendations and classification systems that stratify AR by symptom duration (intermittent vs. persistent) and severity (mild vs. moderate to severe) [2]. These guidelines emphasize the concept of a unified airway and advocate for the integrated care of upper and lower airway diseases. Recent ARIA updates have further advanced this framework by incorporating Grading of Recommendations Assessment, Development and Evaluation methodology, real-world evidence, and patient-centered treatment algorithms [3,4]. Moreover, advances in pharmacologic therapies, allergen immunotherapy (AIT), and digital health tools have transformed the management landscape of pediatric AR.
The Korean Academy of Asthma, Allergy, and Clinical Immunology (KAAACI) has developed clinical practice guidelines tailored to epidemiological and clinical contexts in Korea. The KAAACI Allergic Rhinitis Guidelines, most recently updated in 2022, provide evidencebased recommendations for the pharmacologic and nonpharmacologic management of AR [5,6]. These guidelines address key clinical questions, including the use of intranasal corticosteroids (INCS), oral antihistamines (OAH), leukotriene receptor antagonists (LTRA), immunotherapy, and environmental control strategies.
This review aims to provide an up-to-date overview of pediatric AR by focusing on recent advances in management based on the ARIA and KAAACI guidelines and their clinical implications for pediatric care. By integrating current evidence and guideline recommendations, here we seek to help clinicians deliver optimal, age-appropriate, and evidence-based management strategies for children with AR.
Epidemiology
Nationwide, school-based epidemiological studies using the modified International Study of Asthma and Allergies in Childhood questionnaire have been conducted periodically since 1995 in Korea. A recent survey indicated that AR is the most common allergic disease in children and adolescents, with a prevalence exceeding that of asthma and atopic dermatitis [1,7,8]. Recent epidemiologic data suggest an increasing prevalence of AR, while asthma and atopic dermatitis appear to show stable or declining trends in certain populations [9]. The prevalence of AR symptoms over the last 12 months, reportedly less than 30% in 1995, increased to more than 45% in 2022 [1]. This rising prevalence underscores the need for continuous surveillance and updates to treatment strategies to reduce the disease burden affecting children's health and quality of life.
The recent rising prevalence of AR cannot be explained by genetic factors alone, as it is largely driven by environmental changes. Increased exposure to aeroallergens, including pollen, house dust mites, pet dander, and mold, plays a central role. Climate change and air pollution influence the development of AR via interactions with the epithelial barrier, Th2 immune responses, and epigenetics [10]. Disruption of the epithelial barrier allows allergens to infiltrate the subepithelial tissues, inducing allergic immune responses and exacerbating airway inflammation by increasing the release of proinflammatory cytokines [11]. Climate change extends the pollen season and increases allergen production and potency. In addition, air pollution acts as an adjuvant by intensifying airway inflammation and facilitating allergen sensitization [12]. Urbanization and lifestyle changes, characterized by reduced microbial diversity, increased indoor allergen exposure, and altered housing and ventilation patterns, further contribute to disease risk. Early childhood is a critical window of susceptibility during which epithelial barrier integrity, immune maturation, and microbiome development interact to determine allergic sensitization versus immune tolerance.
Pathophysiology
AR, a Th2-driven, immunoglobulin E (IgE)-mediated inflammatory disease of the nasal mucosa that evolves from early allergen sensitization to chronic inflammation and nasal hyperresponsiveness, is closely linked to asthma and other atopic conditions in children [13,14].
During the sensitization phase, antigen-presenting cells in the nasal mucosa process allergens and present them to CD4+ T lymphocytes, thereby promoting a Th2-dominant immune response. This leads to class switching in B cells and the production of allergenspecific IgE, which binds to high-affinity FcεRI receptors on mast cells and basophils. Upon re-exposure, allergen cross-linking of bound IgE triggers degranulation and the release of mediators such as histamine, leukotrienes, and prostaglandins that cause vasodilation, increased vascular permeability, mucus hypersecretion, and sensory nerve activation, resulting in symptoms such as rhinorrhea, itching, sneezing, and nasal congestion. The late-phase inflammatory response involves the recruitment of eosinophils, Th2 cells, and other inflammatory cells that sustain mucosal inflammation and hyperreactivity. Repeated or continuous allergen exposure leads to chronic inflammation of the nasal mucosa with epithelial damage, increased vascular permeability, and neural dysregulation. These changes bolster the chronic and recurrent nature of AR, particularly in children with perennial diseases caused by indoor allergens.
This immunopathological understanding underlies major guideline recommendations, including allergen avoidance strategies and pharmacologic interventions such as INCS and antihistamines, that target different steps of the inflammatory cascade. The ARIA guidelines emphasize the pathophysiological link between AR and comorbid conditions such as asthma through shared type 2 inflammatory pathways, reinforcing integrated management approaches.
Nasal hyperresponsiveness and neuroimmune interactions
AR is also associated with nasal hyperresponsiveness, a phenomenon in which the inflamed nasal mucosa exhibits exaggerated responses to specific allergens and nonspecific stimuli such as cold air, irritants, or strong odors. Neuroimmune interactions involving sensory nerves and inflammatory mediators further amplify a patient's symptoms and contribute to persistent nasal obstruction [15,16]. In pediatric patients, these mechanisms may explain the disproportionate impact of AR on sleep quality, behavior, and cognitive performance.
Unified airway concept and comorbidities
The inflammatory mechanisms underlying AR extend beyond the nasal mucosa and are closely linked to lower airway inflammation. The shared Th2-driven immune response supports the concept of a united airway disease in which AR and asthma represent manifestations of a common underlying inflammatory process. Children with AR are at an increased risk of asthma symptoms, bronchial hyperresponsiveness, and asthma development even in the absence of overt lower airway disease [15,17].
Diagnosis
The diagnosis of AR combines a clinical assessment with objective confirmation of allergic sensitization. A detailed history is fundamental, including symptom patterns (e.g., sneezing, rhinorrhea, nasal congestion, and itching), temporal relationship with allergen exposure, the impact on sleep and school performance, a family history of atopy, and the presence of associated conditions such as asthma or allergic conjunctivitis. Objective testing includes an allergen sensitization evaluation via skin prick tests or serum allergen-specific IgE measurements that help link symptoms to specific allergens and distinguish AR from non-AR, from which allergic sensitization is absent.
In children, AR often presents as a broad spectrum of clinical manifestations beyond the typical nasal symptoms. Nasal obstruction is among the most prominent symptoms that can lead to mouth breathing, sleep disturbances, and impaired daytime performance. Studies have shown that nasal congestion is the most common symptom in pediatric populations and strongly associated with disease burden [18,19]. Chronic nasal obstruction can result in sleep-related problems including poor sleep quality, snoring, and excessive daytime sleepiness, which, in turn, may impair a child's attention, learning, and school performance.
In school-aged children, uncontrolled symptoms are associated with reduced concentration and academic difficulties. In addition to its physical symptoms, pediatric AR is closely linked to psychosocial and behavioral issues. Children with AR reportedly exhibit increased emotional instability, depression, anxiety, and behavioral problems compared with healthy children [20,21]. These effects may be further aggravated during symptom exacerbation. Moreover, the disease's burden extends beyond the child to their caregivers, manifesting as increased parental stress and a psychosocial burden on the families of affected children. Therefore, pediatric AR should be recognized as a condition with a significant multidimensional impact on the physical, cognitive, and psychosocial domains that requires a comprehensive and multidisciplinary management approach beyond symptom control alone.
The ARIA guidelines recommend classifying AR based on symptom duration and severity as follows [22]: Intermittent AR (symptoms <4 days per week or <4 weeks) vs. persistent AR (symptoms ≥4 days per week and ≥4 weeks), and mild (no significant impact on sleep, daily activities, or school/work) vs. moderate to severe (impairment of sleep or daily functioning, troublesome symptoms).
The diagnostic criteria remain consistent with those presented by the ARIA and KAAACI guidelines, which emphasize the importance of confirming sensitization before implementing interventions such as allergenspecific immunotherapy.
Beyond the diagnosis, assessing disease severity and controlling symptoms are essential for guiding management. Tools such as symptom score or visual analogue scale (VAS) scores can evaluate the impact of symptoms on a child's daily activities, sleep, and quality of life [23,24]. Such structured assessments support a control-based approach to treatment and facilitates monitoring of the therapeutic response.
Treatment of pediatric AR
The management of pediatric AR aims to achieve effective symptom control, improve quality of life, prevent disease progression, and reduce the risk of comorbid conditions, particularly asthma. The ARIA guidelines recommend a control-based, stepwise, and patient-centered approach that is especially relevant for children because of their age-dependent disease characteristics, treatment adherence issues, and required caregiver involvement.
General treatment principles
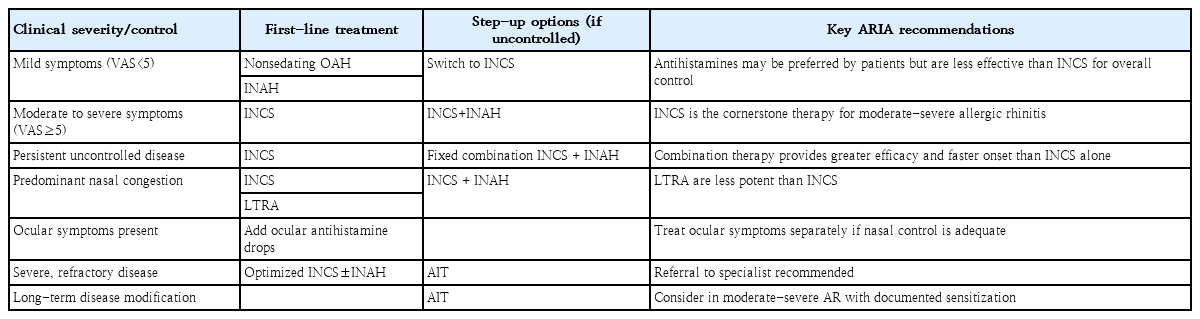
Treatment selection for children should be individualized based on symptom severity, disease control, predominant symptoms (e.g., nasal congestion, sneezing, and itching), patient preferences, and previous treatment response. Disease control is commonly assessed using VAS scores, which indicate treatment escalation or de-escalation (Table 1). Nonpharmacologic measures, including allergen avoidance and environmental control, should be considered adjunctive strategies, although their effectiveness as standalone interventions is limited.
ARIA guidelines-based pharmacologic treatment of allergic rhinitis
Additional considerations beyond pharmacologic efficacy are required for pediatric patients. Younger children often have difficulty using the correct intranasal spray technique, which can significantly affect treatment efficacy. Children tend to prefer oral medications because intranasal sprays can cause nasal irritation, sneezing, and a bitter taste. Dependence on caregivers for medication administration, variability in symptom perception, and concerns regarding long-term safety may influence treatment adherence and clinical outcomes. Therefore, the treatment strategies for children should include caregiver education, simplified regimens, and age-appropriate delivery methods.
Adherence to intranasal therapy regimens remains a major challenge in real-world clinical practice, particularly in pediatric populations. Recent studies from the ARIA research group using real-world data, including digital tools such as the MASK-air mobile application, demonstrated that many patients, including children, tend to use intranasal medications intermittently or only when their symptoms worsen rather than as prescribed [4,25].
Improper spray techniques and a lack of caregiver supervision are common treatment barriers. This discrepancy between guideline-directed recommendations and actual use highlights the importance of patient and caregiver education about correct techniques, the use of visual aids, and the need for simplified and practical treatment strategies.
The use of proper intranasal spray technique is essential for effective drug delivery, particularly in pediatric patients for whom incorrect use is common [26]. Before drug administration, the nasal passages should be gently cleared by blowing the nose or nasal irrigation. The child’s head should be positioned slightly forward rather than backward to prevent the medication from draining into the nasopharynx. The spray nozzle should be inserted gently into one nostril and directed laterally away from the nasal septum to optimize the distribution over the lateral nasal wall and reduce the risk of epistaxis. During actuation, the child should inhale gently through the nose while spraying. Forceful sniffing should be avoided, as it may result in the deposition of medication in the throat rather than in the nasal mucosa. Caregiver supervision and repeated instructions are critical for ensuring the correct technique and improving adherence in children (Fig. 1).
Illustration of intranasal spray administration technique. (A) Incorrect technique consisting of a spray directed toward the nasal septum that can cause septal irritation and epistaxis. (B) Correct technique consisting of a spray directed away from the nasal septum that optimizes distribution over the lateral nasal wall.
Pharmacologic treatment
1. Intranasal corticosteroids
INCS remain the cornerstone of treatment for moderate to severe AR and are the recommended first-line therapy for moderate to severe pediatric AR. INCS effectively reduce nasal inflammation and provide superior control of nasal congestion compared with other pharmacologic options. When used at the recommended pediatric doses,
INCS have a favorable safety profile featuring minimal systemic absorption and no clinically significant effects on growth when appropriately monitored. INCS generally begins to show therapeutic effects within a few hours after the first dose (approximately 3– 12 hours) in many patients, and the maximum clinical benefit typically develops with regular daily use over 1–2 weeks [27]. INCS is effective for both seasonal and perennial AR and should be used regularly rather than on an asneeded basis in children with persistent symptoms. However, the ARIA 2024–2025 guidelines acknowledge that real-world medication use in children is often intermittent or as-needed rather than continuous; this pattern is reflected in the evidence appraisal. While the ARIA and KAAACI guidelines do not prescribe a strict INCS treatment duration, clinical practice and evidence support continuing therapy for several weeks to months depending on symptom patterns, allergen exposure, and response and allow their long-term use when indicated with safety reassurance. In Korea, INCS are generally approved for use in children 2 years of age and older depending on the drug (Table 2).
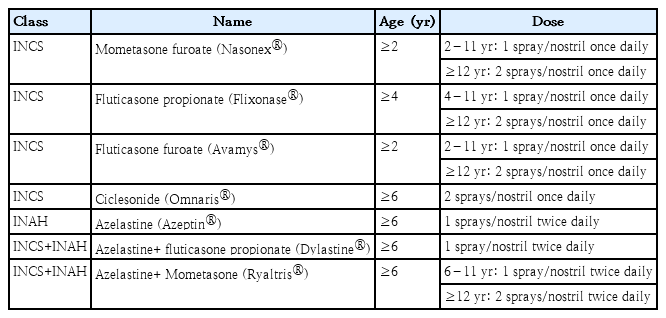
Intranasal sprays for pediatric allergic rhinitis in Korea
2. Oral antihistamines
Second-generation OAH may be used in children with mild symptoms, particularly when sneezing, itching, and rhinorrhea predominate or allergic conjunctivitis is present. These agents are less effective against nasal congestion and generally considered less potent than INCS. Second-generation OAH (e.g., levocetirizine, loratadine, and fexofenadine) usually begin to work within 1 hour after ingestion, with a peak effect within 1–2 hours [27].
3. Intranasal antihistamines
Intranasal antihistamines (INAH) are recommended for children with mild disease or who require rapid symptom relief. INAH offer a more rapid onset of action than INCS, i.e., within a few minutes rather than an hour. INAH is more effective for nasal symptoms than OAH [28,29].
The ARIA 2024–2025 guidelines conditionally recommend using a fixed combination of INCS+INAH rather than INAH alone [4]. Compared with INAH alone, INCS+ INAH more notably improves nasal symptoms and quality of life in seasonal AR. For ocular symptoms, the differences are minimal and evidence is lacking.
Despite their rapid onset of action and efficacy, INAH have several limitations, particularly in pediatric populations, including bitter taste, local nasal irritation, potential sedation, and lower efficacy for nasal congestion than INCS, that can adversely affect treatment adherence. Therefore, INAH are typically recommended for mild diseases or as adjunctive therapy, rather than as monotherapy in persistent or more severe cases.
In Korea, intranasal azelastine is available for use in children with vasomotor rhinitis aged 12 years and older. The indications for AR have been approved in adults only.
Combination therapy
1. Combined INCS + INAH
For children who experience insufficient symptom control with INCS alone, ARIA guidelines support the use of combination therapy with INCS+INAH. This combination provides faster symptom relief and improved efficacy compared to INCS monotherapy and is particularly useful in patients with moderate to severe disease or prominent nasal congestion. The 2023 KAAACI guidelines also suggested that INCS+INAH combination therapy may provide improved symptom relief compared to INCS monotherapy, particularly in terms of nasal congestion [5]. The 2024–2025 ARIA guidelines recommend INCS+INAH combined therapy as a step-up option for patients with inadequate control using INCS alone, balancing faster symptom relief against potential tolerability and adherence issues, particularly in pediatric patients [4].
However, use of the INCS+INAH combination was associated with higher rates of local adverse effects, notably bitter taste and nasal discomfort, which may reduce adherence, particularly in children. Moreover, the required twice-daily dosing may further reduce adherence in children compared with once-daily INCS. Therefore, combination therapy should be reserved for selected patients based on symptom control, tolerability, and patient or caregiver preferences, using a controlbased management approach.
INCS+INAH combinations currently available for pediatric use (ages 6 years and older) in Korea include azelastine+fluticasone and olopatadine+mometasone (Table 2). According to the 2024–2025 ARIA guidelines, azelastine+fluticasone demonstrated superior efficacy to olopatadine+mometasone in adults; however, the evidence was insufficient in children and adolescents to support the superiority of any specific treatment. In patients who experience a bitter taste with azelastine+ fluticasone, olopatadine+mometasone may be preferred.
2. Combined INCS+OAH
Evidence indicates that INCS+OAH combination therapy does not demonstrate superior improvement in overall AR or allergic conjunctivitis symptoms compared with INCS monotherapy. However, combination therapy may slightly improve rhinorrhea and patient-reported quality of life compared to INCS alone [5]. Since INCS typically does not exert marked effects within the first 2 hours of administration, adding a fast-acting OAH (e.g., levocetirizine, cetirizine, or fexofenadine) may providemore rapid symptomatic relief [3]. Despite this potential benefit, combination therapy is associated with a greater tendency toward treatment-emergent adverse events such as dry mouth and notably increased sleepiness compared to INCS alone, although the overall adverse event rates are low for both strategies. Given the different routes of administration and their potential impact on patient adherence, the guidelines committee issued a conditional recommendation for choosing INCS+OAH combination therapy or INCS monotherapy based on individual patient values and preferences and the risk– benefit ratio. The use of INCS+OAH does not confer a significant additional benefit over INCS alone and is not routinely recommended [5].
Leukotriene receptor antagonists
LTRA may be considered an add-on therapy, particularly in patients with concomitant asthma, but are generally less effective than INCS for rhinitis symptom control. The KAAACI also suggested LTRA use to improve rhinitis symptoms in patients with AR and asthma [5]. LTRA monotherapy does not adequately suppress nasal mucosal inflammation; therefore, it should not be a first-line treatment for moderate to severe AR.
Compared to second-generation OAH, LTRA show similar or inferior efficacy for most nasal symptoms. As a result, the ARIA guidelines do not routinely recommend LTRA monotherapy for AR. As LTRA are orally administered, they may be preferred by children and caregivers who have difficulty administering intranasal therapies.
An important limitation in pediatric practice is concern regarding adverse neuropsychiatric effects including mood changes, sleep disturbances, and behavioral symptoms, which are reportedly associated with montelukast. Recent meta-analyses reported a modestly increased risk of anxiety associated with montelukast use, whereas no consistent association has been demonstrated with depression or suicidal behaviors [30]. Although concerns regarding montelukast-associated neuropsychiatric adverse events have been reported, the overall risk remains relatively low, and these agents continue to be widely used in clinical practice, particularly in children with concomitant asthma. Therefore, LTRA may be considered an alternative or add-on therapy in selected patients with appropriate monitoring and after individualized risk– benefit assessments.
Prophylactic treatment for seasonal AR
For children with seasonal AR, prophylactic treatment, ideally initiated 1–2 weeks before pollen exposure and continued throughout the exposure period, improves symptom control, with INCS recommended as first-line therapy [5].
Current treatment guidelines support a preemptive, control-based approach in patients with well-defined seasonal triggers such as trees, grass, or weed pollen. Initiating treatment before allergen exposure can reduce the intensity of allergic responses, resulting in better symptom control, reduced medication escalations, and improved quality of life during pollen season. Children with a history of moderate to severe seasonal symptoms, recurrent annual exacerbations, or significant impairment during the pollen season are particularly suitable candidates for prophylactic therapy.
Second-generation OAH or INAH may be prophylactic options in children with mild seasonal symptoms or as adjunctive therapy [31]. However, antihistamines primarily target histamine-mediated symptoms and are less effective than INCS at preventing nasal congestion and latephase inflammation. As a result, antihistamines alone are generally insufficient as prophylactic monotherapy in children with moderate to severe seasonal AR.
For children with a history of inadequate symptom control using INCS alone during previous seasons, combination intranasal therapy (INCS+INAH) may be considered a prophylactic or early-season step-up option. This approach offers faster symptom relief while maintaining anti-inflammatory control but should be balanced against potential tolerability and adherence issues.
LTRA are not recommended as first-line prophylactic therapy for seasonal AR because of their limited efficacy compared with INCS. Thus, their use should be considered only in selected children, particularly those with concomitant asthma, and careful attention paid to their safety.
AIT (subcutaneous or sublingual) is a long-term prophylactic strategy for children with severe seasonal AR and well-defined pollen sensitization. When initiated and continued appropriately, immunotherapy can reduce seasonal symptom severity and medication use over successive pollen seasons and may provide sustained benefits beyond the treatment period [32].
Although omalizumab, a monoclonal anti-IgE antibody, has shown potential benefits of reducing seasonal AR symptoms in selected studies, the ARIA guidelines do not recommend its use as a prophylactic therapy; thus, its role remains limited to off-label use in selected patients, particularly those with comorbid severe asthma [33].
The ARIA guidelines emphasize that prophylactic treatment for seasonal AR should be individualized based on symptom severity in the previous seasons, anticipated allergen exposure, patient age, and treatment preferences. The early initiation of an effective therapy, particularly INCS, is central to achieving optimal seasonal symptom control in children.
Allergen immunotherapy
AIT is the only disease-modifying treatment for AR that induces long-term immune tolerance against specific allergens. Unlike pharmacologic treatments that provide symptomatic relief, AIT can lead to sustained improvement in AR symptoms and reduced medication requirements despite treatment discontinuation, the possible prevention of new allergen sensitization, and a potentially reduced risk of developing asthma or worsening lower airway disease, supporting the concept of unified airway management [32]. For patients with persistent symptoms despite optimized pharmacotherapy, the ARIA guidelines recommend considering AIT, particularly in patients with clearly identified allergen sensitization and coexisting asthma.
AIT should be considered in patients with clinically relevant IgE-mediated AR when the following conditions are met: (1) confirmed sensitization to relevant allergens demonstrated by skin prick testing or serum allergenspecific IgE; (2) moderate to severe and persistent symptoms that significantly impair quality of life; (3) inadequate symptom control despite optimized pharmacotherapy and allergen avoidance or a desire to reduce long-term medication use; and (4) a clear correlation between allergen exposure and symptoms, with AIT being especially appropriate when symptoms are triggered by a limited number of well-defined allergens [34].
In pediatric practice, AIT is generally recommended for children aged 5 years and older, although the exact age threshold may vary depending on treatment modality and the child’s ability to cooperate [35].
Despite its advantages, AIT has several limitations. Treatment requires a long duration, typically 3–5 years, which may affect adherence. The benefits of AIT are not immediate, and symptom improvement usually occurs gradually over several months. Additionally, AIT is allergen-specific and may not be suitable for patients with polysensitization without clear dominant allergens. Cost, accessibility, and patient or caregiver preference also influence treatment decisions. Safety considerations are critical. subcutaneous immunotherapy (SCIT) carries the risk of systemic allergic reactions including anaphylaxis; therefore, it must be administered in a medical setting with appropriate supervision. Sublingual immunotherapy (SLIT) has a more favorable safety profile, with most adverse events being local and mild and including oral itching or throat discomfort; however, systemic reactions, though rare, may still occur. Unlike SCIT, which requires monthly injections at a hospital, SLIT requires daily administration at home, which can lead to poor compliance and loss of follow-up.
Nonpharmacologic treatments
Saline nasal irrigation is recommended as an adjunctive therapy for patients of all ages, including children, to reduce nasal symptoms and improve mucociliary clearance with minimal side effects [6].
Environmental control measures, including the use of dust mite-proof bedding or high-efficiency particulate air filters, can reduce indoor dust mite concentrations and alleviate dust mite-related AR symptoms [6].
For patients with AR sensitized to animal dander whose symptoms become aggravated after exposure to animals, the use of air purifiers, bathing of the animals, and avoidance therapy or environmental management of the animals is recommended [6].
Surgical intervention
Surgery may be considered for children with structural abnormalities such as turbinate hypertrophy, septal deviation, and refractory symptoms despite optimal medical therapy. Surgery is not recommended for children under 6 years of age because of limited evidence of its efficacy and anatomical immaturity [6].
Stepwise treatment and disease control
The ARIA guidelines emphasize a step-up and stepdown strategy based on symptom control rather than severity using symptom burden (e.g., VAS scores) and incorporating patient preferences, adherence, and feasibility into shared decision-making [4]. Treatment should be escalated if symptoms remain uncontrolled and deescalated once adequate control is achieved. Regular reassessments of disease control, treatment adherence, and spray techniques are essential in pediatric practice.
Integrated airway management
Consistent with the ARIA guidelines' concept of a unified airway, children with AR should be evaluated and managed for coexisting asthma. The effective treatment of AR improves asthma control and reduces exacerbations, highlighting the importance of integrated airway management in pediatric patients.
What is new in the 2024–2025 ARIA guidelines
Compared with the previous ARIA guidelines, the 2024–2025 update introduces several clinically important refinements (Table 3). First, it strengthens the preference for INCS as a cornerstone therapy based on higherquality comparative evidence. Second, it supports the use of a fixed-dose INCS+INAH combination as a stepup strategy when control is inadequate. The INCS+INAH combination can provide greater symptom reduction and faster onset of action than INCS monotherapy. Third, it reinforces a control-based, patient-centered approach using real-world evidence rather than relying on severitybased classifications. Fourth, it provides more explicit recommendations that discourage ineffective add-on therapies such as the routine combination of OAH and INCS. Furthermore, it underscores the importance of adherence and correct intranasal spray techniques, especially in pediatric populations, where improper use remains a major barrier to effective disease control. Finally, the ARIA guidelines do not support the routine use of intranasal decongestants for AR owing to limited longterm benefits and safety concerns; rather, their use may only be considered for short-term relief of severe nasal congestion (≤5 days). A key limitation is the high risk of rebound nasal obstruction (rhinitis medicamentosa). Compared with INCS or INCS+INAH, intranasal decongestants do not provide sustained control of inflammation or overall symptoms. Overall, these guidelines support a stepwise, patient-centered approach that integrates evidence-based pharmacotherapy with real-world considerations to optimize AR outcomes.
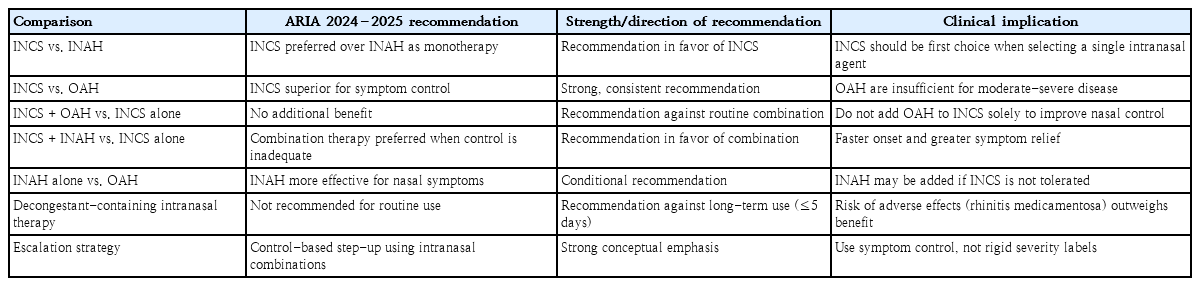
Head-to-head comparisons of intranasal treatments, 2024–2025 ARIA guidelines
Conclusion
In summary, the 2024–2025 ARIA and 2023 KAAACI guidelines reaffirm INCS as the first-line therapy for AR, with combination therapy (INCS+INAH) recommended for patients who experience inadequate control. The ARIA guideline update further strengthens the shift toward a patient-centered, real-world approach that emphasizes adherence, correct intranasal delivery techniques, and individualized treatment decisions. Overall, optimal management requires both evidence-based pharmacotherapy and the consideration of patient preferences, disease variability, and long-term strategies such as AIT in selected cases.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contribution
All contributions to this paper were made by the single author (JYS).