Ultrasonographic features of 5-aminosalicylic acid intolerance in pediatric ulcerative colitis
Article information

5-Aminosalicylic acid (5-ASA) is a first-line therapy for mild-to-moderate ulcerative colitis (UC), including pediatric cases. 5-ASA intolerance affects approximately 10% of UC patients [1], mimicking exacerbations [2]. and potentially causing unnecessary treatment escalation [3]. No reliable method currently exists to distinguish 5-ASA intolerance from UC exacerbation. Abdominal ultrasonography is useful for assessing the extent and localization of inflammatory lesions in inflammatory bowel disease [4]. In pediatric patients with UC, bowel wall thickening has been identified as a sonographic indicator for detecting inflamed intestinal tracts [5]. However, the ultrasound features of 5-ASA intolerance remain unexplored. Herein, we retrospectively examined the ultrasonographic features and discussed the utility of ultrasonography in patients with 5-ASA intolerance. Written informed consent was obtained from all patients and their legal guardians.
Case 1: A 10-year-old boy presented with arthralgia and was referred. Abdominal ultrasonography was performed due to positive fecal occult blood, which showed thickening in the transverse and descending colon. The patient was diagnosed with UC by colonoscopy and histological examination. Time-dependent release mesalazine was initiated at 2,000 mg/day, which was increased to 3,000 mg/day after 2 weeks. Following dose increase, diarrhea and oral ulcers worsened. Ultrasonography revealed ileal wall thickening but no thickening of the descending or sigmoid colon. Suspecting 5-ASA intolerance, mesalazine was discontinued and prednisolone (45 mg/day) initiated, leading to symptom resolution. While maintaining prednisolone, a challenge test with mesalazine (3,000 mg/day) caused diarrhea. Ultrasonography revealed ileal wall thickening (Fig. 1A) and intestinal fluid accumulation (Fig. 1B), without colonic thickening. Mesalazine discontinuation led to symptom resolution.
Abdominal ultrasonographic findings of the ileum and ascending colon at the onset of symptoms of 5-aminosalicylic acid (5-ASA) intolerance. The arrows indicate thickening of the intestinal wall, while the asterisks indicate intestinal fluid accumulation. Thickening of the ileal wall (A) and intestinal fluid accumulation (B) in case 1. Thickening of the ileal wall (C) and intestinal fluid accumulation (D) in the ileum in case 2. Thickening of the ascending colonic wall (E) and intestinal fluid accumulation (F) in the ileum in case 3.
Case 2: A 5-year-old girl presented with bloody stools, diarrhea, and abdominal pain. Abdominal ultrasonography revealed wall thickening in the sigmoid colon. The patient was diagnosed with UC based on colonoscopy and was administered time-dependent release mesalazine (1,500 mg/day) and prednisolone (16 mg/day). Following improvement, prednisolone was tapered to 5 mg/day. Six weeks after starting treatment, the mesalazine dose was increased to 2,000 mg/day, triggering symptom recurrence. Ultrasonography revealed ileal wall thickening (Fig. 1C) and intestinal fluid accumulation (Fig. 1D), but no abnormalities were observed in the transverse or descending colon. Suspected 5-ASA intolerance led to mesalazine discontinuation, with symptoms resolving within four days. While receiving prednisolone at 15 mg/day, a subsequent challenge test with salazosulfapyridine reproduced the intestinal fluid accumulation without colonic thickening, confirming 5-ASA intolerance.
Case 3: A 15-year-old girl presented with abdominal pain and bloody stools. Ultrasonography revealed wall thickening in the descending and sigmoid colons. She was diagnosed with UC by colonoscopy. She was started on pH-dependent release mesalazine (2,400 mg/day). Ten days after treatment initiation, the patient developed diarrhea and abdominal pain. Ultrasonography revealed ileal and ascending colonic wall thickening (Fig. 1E) and intestinal fluid accumulation (Fig. 1F), with no lesions in the descending or sigmoid colon. Discontinuation of mesalazine for suspected 5-ASA intolerance, followed by prednisolone (45 mg/day), resolved symptoms within 3 days. While receiving prednisolone (15 mg/day), a challenge test with salazosulfapyridine induced diarrhea and abdominal pain after 4 days.
The clinical characteristics and ultrasonographic findings of three patients are summarized in Table 1. In this report, small intestinal fluid accumulation and wall sensithickening were observed in all cases. Furthermore, right-sided colonic wall thickening occurred in 1 patient. Two patients with small bowel lesions were treated with time-dependent release mesalazine, which releases in the small intestine. One patient with terminal ileal and ascending colonic wall thickening received pH-dependent release mesalazine, which releases in the distal small intestine. These findings suggest that bowel wall thickening may develop in regions directly exposed to 5-ASA, depending on the formulation's release characteristics.
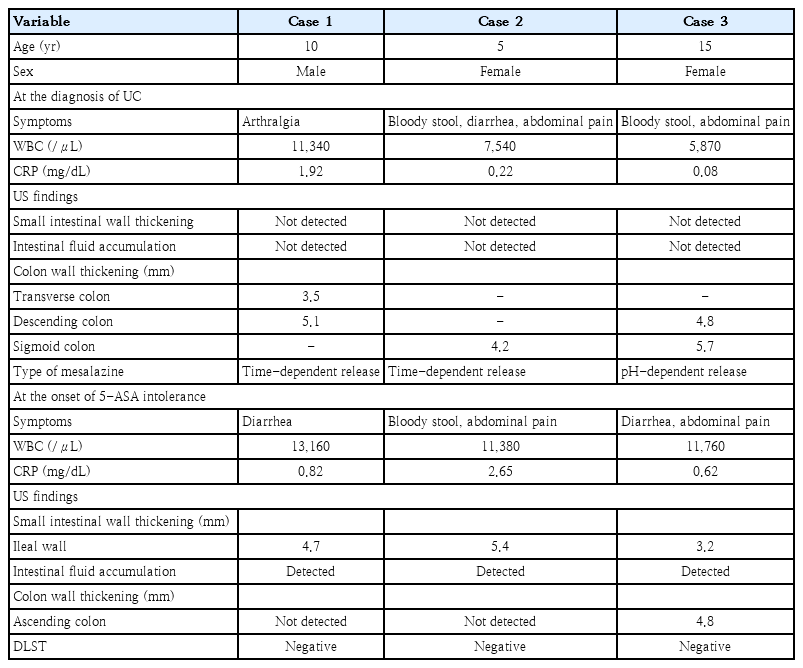
Clinical characteristics and ultrasonographic findings of pediatric patients with ulcerative colitis and 5-ASA intolerance
A case series on endoscopic findings in 5-ASA intolerance reported intense mucosal inflammation in the right-sided colon, presumably due to high 5-ASA concentration [6]. Additionally, a single mesalazine suppository caused severe inflammation in the descending colon, the site of direct exposure [7]. These studies support our findings.
Notably, no colonic wall thickening was observed at the onset of 5-ASA intolerance in our patient. Bowel wall thickening correlates with disease activity in pediatric UC [8]. 5-ASA intolerance should be considered if symptoms suggest relapse but ultrasonography shows minimal colonic involvement and prominent small intestinal lesions.
All patients tested negative for drug lymphocyte stimulation test (DLST) against mesalazine. A previous study reported that the DLST might not be suitable to exclude the 5-ASA intolerance because of the low sensitivity [6]. Given the DLST is a time-consuming procedure, ultrasonography may serve as a useful screening tool for suspected 5-ASA intolerance.
This study has limitations, including the small sample size and operator-dependent nature of ultrasound examination. Further studies are needed to confirm these findings.
We demonstrated the features of ultrasonography in patients with 5-ASA intolerance and highlighted its potential for managing this condition. In conclusion, when small intestinal or right-sided colonic abnormalities are detected by ultrasonography in patients with UC receiving 5-ASA, intolerance should be considered a differential diagnosis.
Question
Which ultrasonographic finding is useful for distinguishing 5-ASA intolerance from UC exacerbation?
(A) Left-sided colonic wall thickening
(B) Small intestinal or right-sided colonic lesions without left-sided colonic wall thickening
(C) Isolated rectal wall thickening
(D) Intestinal abscess formation
Answer: B
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contribution
Conceptualization: YS, YA; Data curation: HM, YS, YA; Formal analysis: HM, YS, YA; Methodology: YS; Visualization: YS, YA; Writing - original draft: HM; Writing - review & editing: YS, SH