Intercontinental comparison of caustic ingestion in children
Article information
Abstract
Purpose
To investigate the caustic ingestion in children among different continents according to demographic characteristics (core purpose), main symptoms, common caustic agents, signs and symptoms, management, treatment and complications.
Methods
This systematic review was performed by searching the databases Science Direct, ProQuest, Google Scholar, and PubMed, electronically and manually. We included studies that were published from 1980 to 2013, at University of Medical Sciences of Tabriz, Iran. A strategic search was performed with keywords including caustic, corrosive, ingestion and children, and was limited to articles in English and Persian. Statistical analysis was performed by SPSS ver. 18.
Results
Of 63 selected articles of caustic ingestion with 9,888 samples, the proportion of Africa was 3 articles (4.8%) and 95 samples (1%), America 9 articles (14.3%) and 305 sample (3%), Asia 29 articles (46%) and 2,780 samples (28.1%), Europe 17 articles (27%) and 3,002 samples (30.4%), and Oceania 5 articles (7.9%) and 3,706 samples (37.5%). The average age was in the Africa 3.07±2.02 years, America 3.17±1.83 years, Asia 3.34±1.58 years, Europe 3.58±2.09 years and Oceania 3.52±2.02 years. Sex distribution was in Africa 76 males (0.91%) and 19 females (0.23%), America 49 males (0.58%) and 41 females (0.49%), Asia 1,575 males (18.76%) and 1,087 females (12.95%), Europe 1,018 males (12.13%) and 823 females (9.8%), and Oceania 1,918 males (22.85%) and 1,788 females (21.3%). Statistical analysis of the data indicated higher consumption in Europe and Oceania in the boys with higher average age of years.
Conclusion
The comparison of caustic ingestion indicated that the cause substances of caustic ingestion in children are different among continents, therefore prevention strategy and different treatment guidelines among continents will be needed.
Introduction
Accidental caustic ingestion in children is a worldwide problem1). Overall, in the early 1950s, rate of childhood ingesting was estimated at 286 per 100,000 children under the age of 6 years and mortality rate for children aged 1 year was 10.6 and 5.9 per 100,000 for males and females, respectively2).
Although the incidence has decreased in developed countries due to security measures imposed on hazardous products, it is the potential threat to children because of the continuously expanding household agents in markets3). The incidence of caustic ingestion in children has persisted in most developing countries4).
In some countries there is effective planning of regional health policy or vigorous preventative programs have noticeably helped to reduce accidents15). In Denmark, enforcement of these legislations led to a perfect drop in the incidence5).
The improper storage and utilization pattern of household in the home have been responsible for a noticeable number of ingestion cases6). Also, the educational level of families, economic status and sociodemographic profiles might be associated with occurrence of these events7).
The degree of a corrosive lesion depends on the nature, concentration, and quantity of the caustic ingestion8). The early manifestations are nausea, abdominal pain, vomiting, and dyspnea. The systematic symptoms, which may develop rapidly or be delayed, include fever, tachycardia, tachypnea, and dysphasia9). The determination of the severity of damage following caustic substances is one of the most important initial steps for treatment and the prevention of formulation of injuries, which can be short-term and long-term1011).
Early esophagogastroduodenoscopy allows a safe and proper evaluation of the location and degree of damage to the upper gastrointestinal tract12).
Two to 4 days postinjury was observed perforation, scarring and contracture. Up to 33% of patients develop long-term complications, principally esophageal, oral and pharyngeal strictures13).
Different treatments were considered, for example antiacid, antibiotic, corticosteroid and esophageal dilatation with esophagoscopy such as traditional treatment, however, there is no standard treatment of caustic ingestion during the acute phase; several treatment protocols are described in pediatrics surgery books but standard management remains to be controversial714).
Early reference and proper assessment of the patients is very important because the prognosis depends on application of appropriate treatment15). So, caustic ingestion remains a serious medical and social problem in world5).
This study includes10 aims, that 1st, 2nd, 3rd, and 4th aims are the original purposes of the study in order to compare the rate of published articles, rate of ingested children, age distribution, and sex ratio among continents. 5th, 6th, 7th, 8th, 9th, and 10th aims are minor purposes to compare the type of ingested agents, main sign and symptoms, diagnostic protocols the initiating time of endoscopic examination, therapeutic methods, and complications in ingested children of different continents. Therefore prevention strategy and different treatment protocols among continents will be needed and the results of this study would be helpful.
Materials and methods
This study was performed for assessment and comparison the published articles, rate of ingested caustic agents in children, age distribution, sex ratio, type of ingested agents, symptoms, diagnostic procedures, therapeutic methods, complications, the initiating time of the endoscopic examination and impact of chemical factors on the organs in children among 5 continents since 1980 based on the systematic review of papers and in 4 phases, including planning and performance of search strategy, collection of articles and review systematic, evaluation of inclusion and exclusion criteria and finally data extraction and analysis as follow:
1. Searching strategy
In the first phase, databases such as Springer, Science Direct, ProQuest, Google Scholar, and PubMed were strategically searched to find studies written in English from 1980 to July 14, 2013, at University of Medical Sciences of Tabriz, Iran. A search strategy was planned for each database using Boolean research methods, field, cut documentation, collection, and English language limits with keywords such as caustic, corrosive, ingestion, and children by medical subject headings (MeSH) for Medical Science Databases with cooperating of gastroenterology pediatric subspecialist, physiologist, PhD by researchers, and clinical librarian. Search strategy was employed similar with the following strategy designed to PubMed:
caustics"[Pharmacological Action] OR "caustics"[MeSH Terms] OR "caustics"[All Fields] OR)))"caustic"[All Fields]) OR ("caustics"[Pharmacological Action] OR "caustics"[MeSH Terms] OR "caustics"[All Fields] OR "corrosive"[All Fields])) AND ("eating" [MeSH Terms] OR "eating"[All Fields] OR "ingestion"[All Fields])) AND ("child"[MeSH Terms] OR "child"[All Fields] OR "children"[All Fields].
Also, despite the inability to use of research strategies in internal databases, wider and manual research was performed with minimum limitation in SID, Magiran, Iranmedex, and MedLib. Finally, references were surveyed for accessibility to other related studies. It was considered all of ethical aspects.
2. Evaluation and selection of studies
In the second phase, all collected studies were separately surveyed by two authors from different centers independently to evaluate article quality, and irrelevant studies (e.g., related to adults, swallowing batteries, drug abuse, printed articles before 1980 due to low quality) were excluded with appraisals' agreement. Then we asked an independent author from a third center to review the paper(s) in question. Finally, Kappa Agreement Rate was higher than 85% as inclusion criteria to the next phase.
3. Inclusion and exclusion criteria
In the third phase, irrelevant studies, without location, systematic articles, case control articles, cohort articles, clinical trial articles, animal studies, Kappa Agreement Rate less than 85%, duplication articles and letters were considered as exclusion criteria. Also, the related articles obtained manually from references of review articles were added to the set.
4. Data extraction and statistical analysis
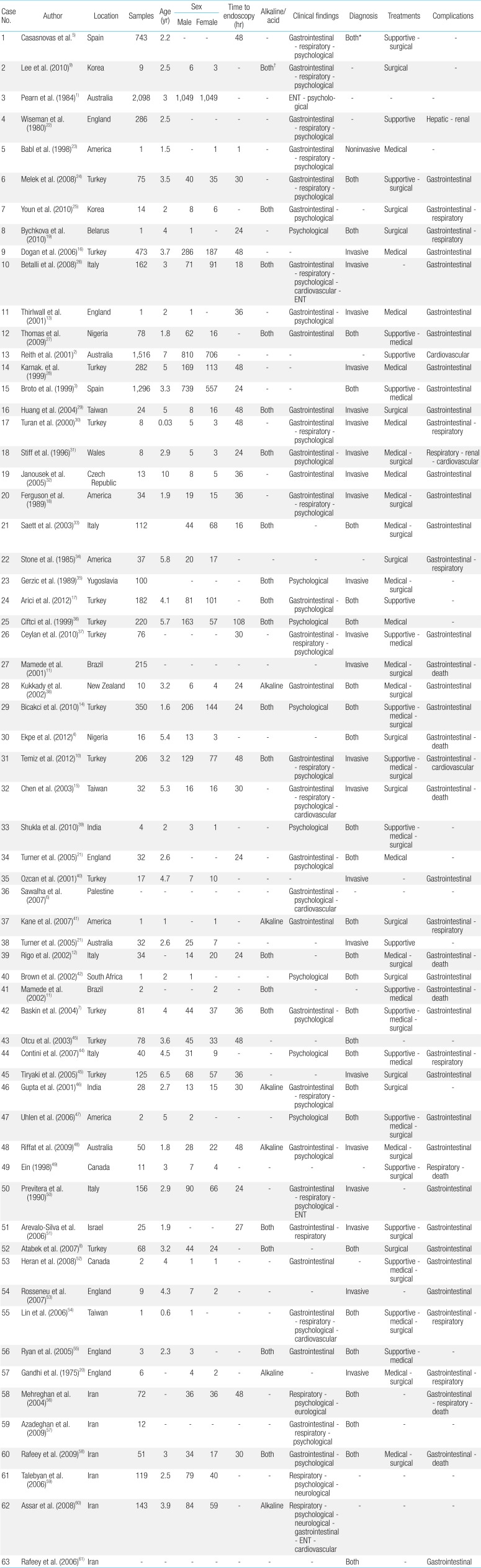
Each author independently extracted data on the checklist such as the rate of published articles, rate of ingested children, age, sex, type of ingested agents, symptoms, diagnostic protocols, therapeutic methods, complications, and the interval time between caustic ingestion and endoscopy. Authors used the SPSS ver. 18.0 (IBM Co., Armonk, NY, USA) to analyse the data using of descriptive statistical methods (mean, standard division, range, frequency, percentage, and ratio). We were not able to present data in a P value for this version of the review and we only described the data. Data was grouped into two parts (quantitative and qualitative) (Tables 1, 2). All data was summarized in Extraction Table of Excel Microsoft Office Software (Table 2).

Classification of characteristics of agents, clinical findings, methods of diagnostic and therapeutic, and complications

Comparison of the results of caustic ingestions in children among countries
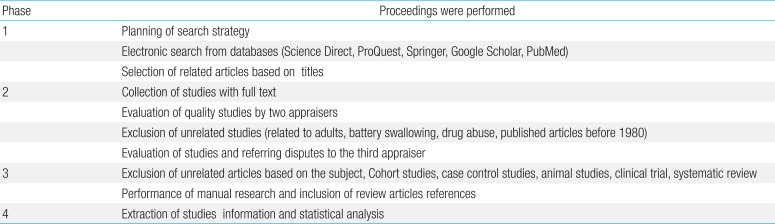
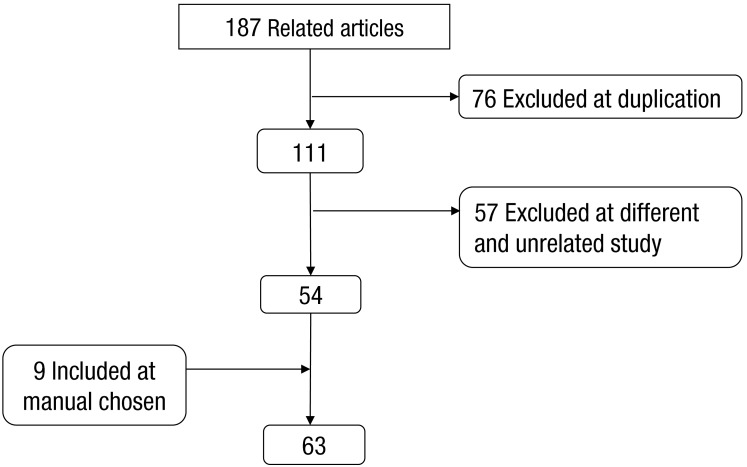
The summery of mentioned phases were shown in Table 3 and Fig. 1.

Summary of performed process for searching strategy
Summary of studies contributing to the systematic review.
Results
A total of 187 studies that were obtained in the process of database mining based on the exclusion criteria, 76 papers in phase 2 and 57 articles in phase 3 were excluded. Nine articles manually selected in phase 3 were included in our study. Finally, data of 63 articles were extracted (Table 2).
Results of this study were numbered as follow:
1. Demographic data
There were 63 articles with 53 cross-sectional articles (84.1%), 6 case reports (9.5%) and 4 case series (6.4%), the proportion of Africa 3 articles (4.8%), America 9 articles (14.3%), Asia 29 articles (46%), Europe 17 articles (27%) and Oceania 5 articles (7.9%).
This study consisted of 9,888 samples, where 95 samples from Africa (1%), 305 from America (3%), 2,780 from Asia (28.1%), 3,002 from Europe (30.4%), and 3,706 from Oceania (37.5%).
The average age of children was 3.38±1.75 years (range, 12 days-10 years), so that in Africa 3.07±2.02 years (range, 1.8-5.4 years), America 3.17±1.83 years (range, 1-5.8 years), Asia 3.34 ±1.58 years (range, 0.03-6.5 years), Europe 3.58±2.09 years (range, 2-10 years), and Oceania 3.52±2.02 years (range, 1.8-7 years).
There were 4,636 male (55.23%) and 3,758 females (44.77%) with (F/M ratio, 0.81). in Africa 76 males (0.91%) and 19 females (0.23%) with (F/M ratio, 0.25), America 49 males (0.58%) and 41 females (0.49%) with (F/M ratio, 0.84), Asia 1,575 males (18.76%) and 1,087 females (12.95%) with (F/M ratio, 0.69), Europe 1,018 males (12.13%) and 823 females (9.8%) with (F/M ratio, 0.81), and Oceania 1,918 males (22.85%) and 1,788 females (21.3%) with (F/M ratio, 0.93).
2. Common caustic agents
The caustic substances were varied. 63% of accidents were caused by alkalines, and 41% by acidic agents which in Africa was (33% alkaline, 33% acid), America (22.2% alkaline, 0% acid), Asia (48.3% alkaline, 41.4% acid), Europe (41.2% alkaline, 35.3% acid), and Oceania (40% alkaline) were recorded (Table 4).

Comparison of the results of caustic ingestions in children among continents
In Africa, Asia, and Oceania children were exposed by household and industrial agents but in America and Europe further household agents were responsible
The effective factors on the severity of injuries included physical and demographic characteristics of children, physical characteristics of materials, and the manner of agent consumption. The manner of agent consumption in Africa and America, physical characteristics of materials in Asia and Europe and demographic characteristics of children and the manner of agent consumption in Oceania were mentioned as effective factors.
3. Signs and symptoms
The majority of patients showed similar signs and symptoms such as digestive, respiratory, ENT (ear, nose, and throat) and psychological, which in Africa and Oceania digestive and psychological signs and symptoms, America and Europe digestive, psychological and respiratory symptoms and in Asia digestive, psychological and respiratory symptoms were reported.
4. Management, treatment, and complications
Noninvasive techniques such as physical examination, blood tests and graphs and invasive techniques such as endoscopy, esophagoscopy, gastroscopy, bronchoscopy, pharyngoscopy, esophageal biopsy and laparotomy were carried out to detect and evaluate lesions. Invasive techniques such as endoscopic examination and noninvasive techniques such as physical examination were mostly used in Africa, Asia, Europe, and Oceania. Invasive techniques were widely used in America.
The mean initiating time of endoscopic examination was 35 hours so that in America 18.5 hours, Asia 42 hours, Europe 27 hours, Oceania 36 hours, and Africa not mentioned.
Therapeutic protocols included medical treatments such as antibiotics, systemic steroids, H2 blockers, protein pump inhibitors, antiacids and topical injection of mitomycin and steroid, surgical therapies such as esophageal dilatation, esophageal replacement and resection of esophagus, implantation of stent and catheter in esophagus and conservative managements so that surgical therapies, medical and conservative therapies in Africa, America, Asia, and Europe were performed respectively. All methods mentioned above were also used in Oceania.
Finally, lesions included digestive (esophageal stricture, esophageal perforation, and esophageal stenosis), respiratory, renal, hepatic, cardiovascular complications and death, that digestive, respiratory and death complications in Africa, America, Asia, and Europe and digestive and cardiovascular complications in Oceania were reported respectively. So, caustic ingestion was more common in Oceania and Europe.
Discussion
Caustic substances, which are widely used for household cleaning products, are frequently swallowed by children.
Corrosive injury caused by these agents is worldwide pediatric emergency problem. Many children suffer from corrosive esophageal burns16). The aim of this systematic review misevaluation and comparison caustic ingestion in children among different continents as follow:
1. Demographic characteristics
The most published articles were in decreasing order related to Asia, Europe, America, Africa, and Oceania; the most samples are related to Oceania, Europe, Asia, America, and Africa. This indicates that cleaners were used widely in Oceania and Europe.
Overall, the majority of preschool boys which had mean age of 3.38±1.75 years, were involved and the comparison of mean age was in that order to Europe, Oceania, Asia, America, and Africa. Baskin et al.7) studies showed that the number of children who ingested caustic agents was 44 boys and 37 girls with a mean age of 4 year respectively.
The high average age in Europe, in comparison with Africa and Asia presumably indicates tendency for intentional actions and insecure storage of caustic reagents and family's recklessness. Also issues of suicide among children should be handled.
In this study, 4,636 males (55.23%) and 3,758 females (44.77%) were analyzed. Our findings indicated that most boys were subjected to caustic ingestion. This ratio in Africa, Asia, and Oceania, America was in the highest and the lowest range respectively. This finding suggests that African and Asian boys need more attention and care for ingestion prevention. At the Wales's University Hospital, from 1974 to 1995, of children admitted in Department of Pediatrics Surgery the ratio of male to female was approximately 2:1, and 85% of ingesting happened in children less than 5 years. In a study, suicide attempt was observed in older children (13-18 years)17).
2. Common caustic agents
In this report, most accidents were caused by alkaline household agents which in Africa, Asia, and Oceania both industrial and household agents were equally used. In America and Europe mostly alkaline household agents were used.
Also in Africa/America, Asia/Europe, and Oceania the manner of consumption, physical characteristics of materials, and demographic characteristics of children were effective factors on severity of injuries respectively. However, these products using for health promotion, they can cause various types of poisoning6). In Africa, Asia, and Oceania, frequent consummation of industrial agents by children may imply the excessive use and inappropriate storage of these agents by families6) and or, employment of child labor in these continents.
3. Signs and symptoms
In this study, the most common signs and symptoms had associated with digestive, respiratory and psychomotor systems. In the 4 continents, digestive symptoms were dominant but psychological symptoms were mostly observed in Asia and America. In Europe and Asia, respiratory symptoms also were observed in many cases.
4. Management, treatment, and complications
In the current study, noninvasive techniques especially, physical examination and invasive techniques especially, endoscopy were used nearly for all patients in majority of continents. Invasive techniques using mainly in America seems to be effective for accurate evaluation of injuries of organs for decreasing the mortality rate.
The mean of initiating time of the endoscopic examination was 35 hours which in America, Asia, Europe, and Oceania was 18.5, 42, 27, and 36 hours respectively. This time was not reported in Africa. Early endoscopic examination was performed in America and Europe. In Chicago, Ferguson et al.18) suggested the early endoscopy is the best mean to evaluate injuries of upper respiratory tract and esophagus. However, Bicakci et al.14) were not in agreement. Furthermore, no esophagoscopy was suggested for caustic reagent ingested patients without any problem. Finally, because of unpredictability of injury progression on the basis of symptoms and physical examination, endoscopy could be effective18).
In Africa, America, Asia and Europe, surgical treatments, medical and conservative therapies were applied respectively. These methods also were equally used in Oceania. We consider that management of all children that are suspected to ingest caustic agents becomes a necessity to conduct precisely because of prognosis, ranging from asymptomatic state to intractable complications19).
In our study, medical therapies such as oral antibiotics, systemic steroids and H2 blockers, surgical therapies such as esophageal dilatation and conservative treatments were utilized to limit the severity of inflammation and infection4). In New York, Gandhi et al.20) reported similar results. Although the benefit of each treatment did not determine by investigators, therapeutic methods should be able to develop as the child growth4).
Esophageal stricture, ulcer, perforation, and nutritional problems were frequently observed. Respiratory symptoms were uncommon, although the presence of respiratory symptoms potentially should be considered serious and managed accurately. Malignancy in long-term follow-up and death were also reported. Ingestion of caustic agents is associated with a low mortality21). Complications associated with ingestion of caustic agents secondarily were seen in long-term stricture formation with a high morbidity mostly in gastrointestinal tract13).
5. Strength and limitation
The advantage of this study is the use of a proper number of valid studies which have been performed by outstanding investigators from diverse origins. In this study, for the first time, different continents were compared with adverse subjects of caustic ingestion. The other benefit is adequate sample size in each study. This study had some limitations. Articles were limited to descriptive articles in English and Persian. Because of scientific sanctions on Iran, several international articles were ignored. Therefore, it may not be enough for us to portray conclusions from our study results.
6. Policy and strategy for prevention
Safety rules as regards caustic agents are as follows: (1) care the children especially, boys when contacted to "danger areas"; (2) never keep caustic agents to other container; (3) buy cleaning agents through formal market with labels show clearly contents; (4) buy products with unattractively appearance and childproof containers; (5) never store cleaning substances extensive daily use; (6) store these agents in availability places; (7) manufactures must consider concentration of caustic agents; (8) media can show lectures to the general public on safe methods of storage and primary proceedings after ingestion; (9) parents must consider earlier reference to hospital after ingestion; (10) doctors correctly manage ingested patients and do not ignore long-term complications in children567).
However, the comparison and evaluation of caustic ingestion can be effective in application of legality and habitual changes leading to decrease of these accidents. Furthermore, increasing communication and using of other views can be effective in suitable management of ingested patients. In conclusion, attention to preventive measures seems as the most applicable and simplest way to prevent of caustic ingestion in children. So, reduction these accidents can be achieved by collaborative efforts carried out by parents, media, and governmental agencies with designation to a tightening of legislative controls on manufacture and packing, public education programs, and to increased public awareness. Therefore, the results of this study would be helpful for providing of prevention strategy and different treatment protocols among continents.
In the other hand, efforts should be made towards an earlier and more correct diagnosis and a suitable treatment of the corrosive substance ingestion. The management modalities of the patients should be changed and increased the success rate of treatment. Finally, multicenter trial with cooperation other countries would be recommended.
Acknowledgments
We would like to thank Liver & Gastrointestinal Disease Research Center.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.
References
Supplementary materials
References of Table 2 can be found via http://www.kjp.or.kr/src/sm/kjp-58-487-s001.pdf as supplementary material.