Role of nonpharmacological concussion management in children: systematic review of randomized controlled trials
Article information

Abstract
Concussion is a global public health problem that affects many children worldwide. Most patients present with postconcussion syndrome and normal brain imaging findings. Despite the high incidence of concussion in children, published research on nonpharmacological management is lacking and much more often concerns pharmacological interventions. This systematic review aimed to evaluate the role of nonpharmacological interventions in managing concussion based on randomized controlled trials. The PubMed, Scopus, Web of Science, and Cochrane databases were extensively searched for articles published between January 2013 and July 2023. A modified patient intervention, comparison, and outcome framework was used to construct the search strategy and eligibility criteria. Risk of bias was assessed using the Risk of Bias-2 tool. A total of 16 studies conducted between January 2013 and July 2023 were analyzed. Three studies were conducted in an acute care setting (<24-hour postinjury) involving rest, computer time, and doing nothing, while the other 13 studies were conducted in a chronic care setting (>24-hour postinjury) and included aerobic exercise, collaborative care intervention, cervical spine rehabilitation, education by physiotherapists, a hyperbaric oxygen therapy protocol, family intervention therapy, virtual reality, traditional occupational therapy, virtual rehabilitation, oculomotor control exercises, vestibular rehabilitation, coordination exercises, and balance exercises. This systematic review highlights the importance of nonpharmacological therapy in pediatric concussion cases. Active rehabilitation may yield promising outcomes. Another interesting approach may be useful in pediatric concussion management. However, this systematic review shows a lack of high-quality literature supporting nonpharmacological pediatric concussion treatments.
Key message
The long-term effects of concussion for pediatric patient remains unclear. Children and teenagers do not experience or recover from concussion in the same manner as adults do. Concussions can cause a variety of anatomical and functional alterations. Nonpharmacological approach in pediatric concussion management is an understudied field of research with significant ability to affect prognosis and quality of life. Active rehabilitation and occupational therapy were especially promising.
Graphical abstract. Review of role of nonpharmacological management of concussion in children. HBOT, hyperbaric oxygen therapy.
Introduction
Traumatic brain injury (TBI) is among the most common causes of emergency department visits, with reported rates of 150–400 visits per 100,000 children [1,2]. Concussion affects 55.9 million individuals worldwide each year [3]. Although the majority of patients are classified as having a concussion despite normal brain imaging, many have postconcussion syndrome (PCS), which includes physical, cognitive, and emotional symptoms. In most individuals, PCS symptoms are predicted to disappear in the weeks following concussion. However, in certain cases, PCS does not resolve and the symptoms become chronic, a condition known as persistent PCS. Although its precise incidence in children is unknown, reports have cited PCS rates of 2.3%–33% [3,4].
The long-term effects of concussion are unclear [5-7]. Children and teenagers do not experience or recover from concussion in the same manner as adults do. Concussions can cause a variety of anatomical and functional alterations [8]. Nervous system immaturity may make the developing brain, which undergoes structural changes at this time, more vulnerable to damage [9]. From a cognitive standpoint, the development of crucial cognitive abilities in children and teenagers, including focus, problem solving, and memory patterns, does not occur linearly [10]. Thus, an injury sustained during a crucial growth period might have harmful long-term consequences, particularly in terms of learning and mental health. Adults and children were initially assessed for concussion using the same methods and equipment. However, the full extent of the effects of a concussion sustained in childhood are unknown [11]. Various pharmacological and nonpharmacological strategies have been proposed to reduce the risk and burden of PCS; however, evidence to guide optimal management is weak and particularly absent in pediatric populations [12].
Symptoms of PCS can persist long-term. Therefore, the use of pharmacological treatments is very dangerous for children due to side effects, possible dosage inaccuracies, and indications for their use. However, effort must be made to improve patient morbidity rates to ensure good quality of life and a productive future. Therefore, it is necessary to develop a nonpharmacological therapy for pediatric PCS that is both noninvasive and easily administered. Given the current state of knowledge and the unique characteristics of children and adolescents, this systematic review focused on the nonpharmacological management of acute concussion and PCS.
Methods
1. Search strategy and selection criteria
A systematic review was conducted to analyze the role of nonpharmacological management of pediatric concussion. The included studies were identified through a search of studies indexed in the PubMed, Scopus, Web of Science, and Cochrane Database of Systematic Reviews databases between January 2013 and July 2023.The 2020 version of the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines was used [13]. The search string used included "mild head injury," "post-concussion syndrome," "pediatric," and non-pharmacological treatment–related terms such as "rest," "physical activity," "vestibular therapy," "vision therapy," "acupuncture," "hyperbaric oxygen therapy protocol," "family intervention," "conventional occupational therapy," "mindfulness and yoga," "collaborative care intervention," "cervical spine rehabilitation," "blue light therapy," and "gaming computer." This study was registered within an Open Science Framework.
The scope of this study was restricted to randomized controlled trials (RCTs) that explored the effect of nonpharmacological treatment on pediatric concussion in an acute or chronic care stages as stated in the Patient, Intervention, Comparison, Outcome, Timing, and Study Design framework (Table 1). "Acute" was defined as nonpharmacological management administered in the first 24-hour following impact. The terms "concussion" and "mild traumatic brain injury" are used interchangeably in this review. All studies that met the following criteria were included: (1) RCT design; (2) focus on children (0–18 years); (3) investigation of the efficacy of nonpharmacological treatment for acute and persistent postconcussive symptoms; and (4) inclusion of eligible outcome measures, including any clinical symptoms and outcome measures involving the acute and chronic treatment periods. We excluded studies of conditions not related to TBI, that were not published in English, for which the full text was unavailable, and that were not included in an RCT. Systematic reviews and meta-analyses were also excluded, but a manual search of the reference lists of the relevant primary studies was conducted.
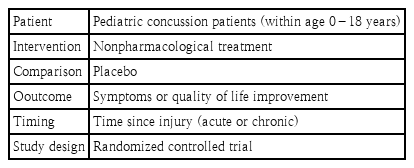
PICOTS framework within the systematic review
2. Data extraction and analysis
After removing duplicates, 2 independent authors screened all titles and abstracts of the retrieved records. Two independent authors then retrieved and assessed the full texts of all shortlisted abstracts. All disagreements were resolved through discussions with the full team. The following data were extracted: (1) year of publication, (2) author names, (3) study design, (4) definition of concussion, (5) primary injury cause, (6) participant characteristics, (7) intervention, (8) duration between concussion and intervention, (9) duration of intervention, and (10) primary outcome. The data extraction was conducted by one author and cross-checked by the main author (Fig. 1).
PRISMA (Preferred Reporting Items for Systematic Review and Meta-analysis) flow diagram.
3. Quality assessment
The Cochrane risk of bias tool for randomized trials version 2 (Risk of Bias-2 tool, RoB 2) was used to evaluate the risk of bias of the included studies [14]. Studies were categorized as having a low risk of bias, some concerns, or a high risk of bias based on the 5 domains.
Results
1. Study selection
A flowchart of the study is shown in Fig. 1. The initial search yielded 110 titles. A total of 64 records were screened; of them, 18 were excluded and 46 were screened for eligibility. Of the 41 reports assessed for eligibility, only 16 met the inclusion criteria.
2. Study characteristics
We identified 16 RCTs that addressed nonpharmacological interventions (Fig. 2) across pediatric populations (Table 2). The terms "concussion" and "mild traumatic brain injury" were used interchangeably, and concussion-defining criteria differed slightly across studies; however, we adopted the definition offered by the 5th International Conference on Concussion in Sport held in Berlin and endorsed by the American Association of Pediatrics of “a traumatic brain injury induced by biomechanical forces [15]. They further elaborated on 5 criteria: concussion may be caused by a direct blow to the head, face, neck, or elsewhere on the body with an impulsive force transmitted to the head; concussion typically results in the rapid onset of short-lived impairment of neurological function that resolves spontaneously; concussion may result in neuropathological changes, but its acute clinical signs and symptoms largely reflect a functional disturbance rather than a structural injury; concussion involves a lack of visible abnormalities on standard neuroimaging studies; and concussion causes a range of clinical signs and symptoms that may or may not involve a loss of consciousness. The above signs and symptoms cannot be explained by other causes.
Flow diagram of evidence-based findings. yo, years old; HBOT, hyperbaric oxygen therapy.
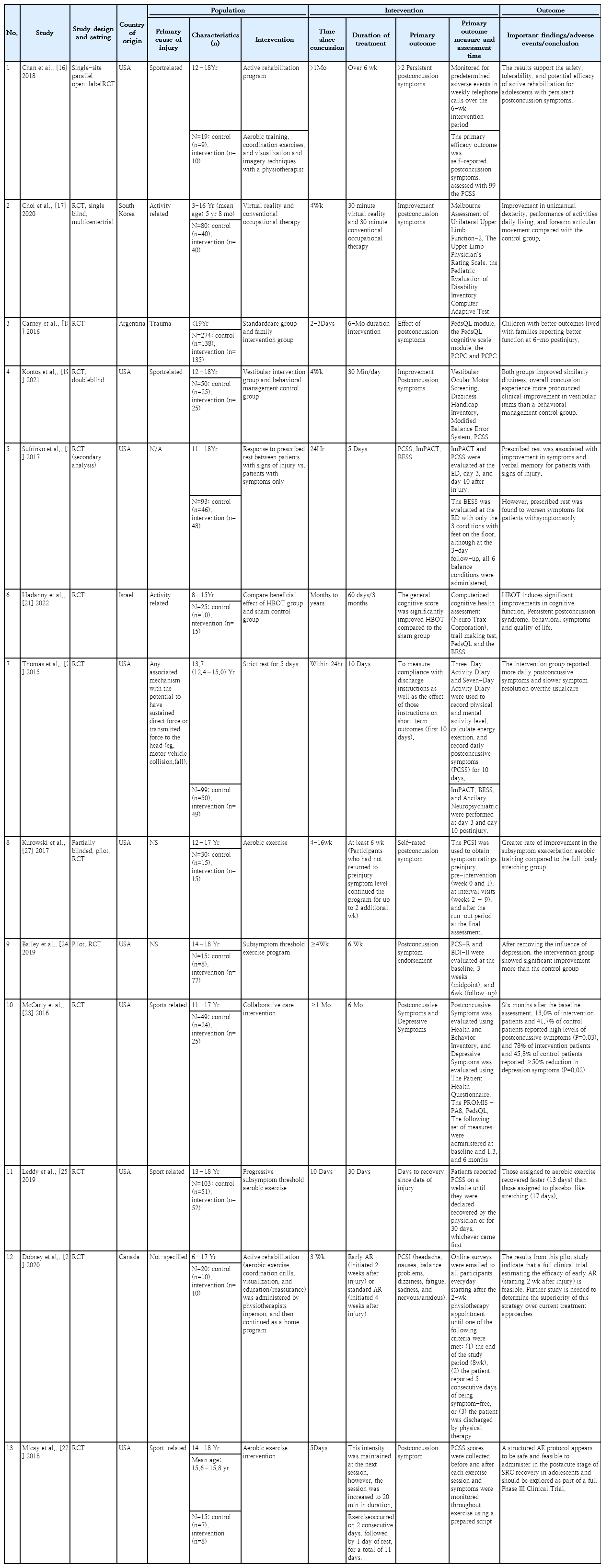
Characteristics and findings of studies of pediatric concussion management included in systematic review
Our review further elaborates on concussion symptoms as being both global and specific. Global symptoms can range from a loss of consciousness, fatigue, and drowsiness to other symptoms that are not limited to a single organ system. Specific symptoms were defined as those that could be identified in a single organ system, such as vertigo, hearing impairment, visual difficulties, cognitive problems (difficulty learning), or psychotic symptoms (changes in personality). While unconventional, these symptom definitions are important in this review in the identification of specific nonpharmacological treatments.
Based on this definition, a large number of studies were included in this review. The included studies comprised 1,069 subjects, of whom 535 received nonpharmacological interventions and 534 were enrolled as controls. The most frequent mechanism of injury was sports-related. Three studies were conducted in the acute (<24-hour postinjury) setting, whereas the other 13 were conducted in the chronic or persistent setting (>24-hour postinjury). The study characteristics and key findings of the individual reports are summarized in Table 1.
3. Description of study outcomes
Postconcussive symptoms were assessed as an outcome measure in nine of 16 studies. Eight studies used the postconcussion symptom scale (PCSS) score as the main outcome [16-23]. Other outcomes included medical clearance to return to sports, severity of depression, quality of life, performance of daily activities, balance, dizziness, and cognitive function [17-26]. Most studies used multiple outcomes, including both patient or parent reports and objective performance measures. The measures were typically assessed pre- and postintervention.
4. Meta-analysis
To further enhance the quality of this review, a meta-analysis was performed whenever possible. The meta-analysis was performed using Review Manager ver. 5.4 (RevMan 5, Cochrane Collaboration, Oxford, UK). A heterogeneity test was first performed to reveal data variability using the I2 test. I2 >50% signifies heterogeneous data; thus, further analysis should employ a random-effects model, whereas I2 50% signifies homogenous data, which allows for a fixed-effects model. Continuous data were analyzed by examining the mean difference, whereas categorical data were analyzed by examining the risk ratio. A funnel plot was created to ensure the absence of publication bias.
5. Acute nonpharmacological management of concussion
Three studies were RCTs conducted in an acute setting (24 hours). Two were evaluated at rest, including prescribed rest and strict rest, while the others were evaluated on permitted screen time and abstinence. The most frequently reported consequence was an acute headache (2 of 2 reports) [20,26].
In an RCT of 93 subjects, Sufrinko et al. [20] showed that rest was associated with improvements in symptoms and verbal memory in patients with signs of injury. Immediate postconcussion assessment and cognitive test and PCSS were used to assess patients on days 3 and 10 for 11–18-year-olds who were tested for 5 days. In an RCT of 99 subjects, Thomas et al. [26] found that enforced rest for 5 days resulted in higher daily postconcussive symptoms and slower symptom recovery than normal treatment. However, the risk of bias associated with this study affects the strength of the evidence. Due to the heterogeneity of the 3 included studies, no meaningful meta-analysis could be performed.
6. Chronic nonpharmacological management of concussion
Thirteen reports from 16 RCTs investigated nonpharmacological therapies for chronic or persistent mild TBI. The most frequently evaluated outcomes (13 of 13 reports) were postconcussive symptoms, visual impairment, vestibular problems, depression, and neurocognitive impairment [16-28].
The literature has described nonpharmacological interventions for global symptoms, such as aerobic exercise, collaborative care intervention, cervical spine rehabilitation, and education by physiotherapists [17,23,25-28]. There are also several nonpharmacological treatments for specific symptoms. In essence, patients with acute headache after concussion may benefit from 3 days of rest. Patients with global symptoms should consider aerobic exercise, collaborative care intervention, and cervical spine rehabilitation, while those with specific symptoms may benefit from symptom-based treatments. Patients with cognitive symptoms require hyperbaric oxygen therapy control or family intervention, whereas patients with psychotic symptoms may only benefit from family intervention. Finally, patients with visual symptoms could use 30-minute virtual reality and conventional occupational therapy or virtual rehabilitation, and patients with vestibular symptoms could benefit from vestibular rehabilitation, coordination exercises, and balance exercises. This is further summarized in the flow diagram of the evidence-based findings (Fig. 2).
Chan et al. discovered the safety, tolerability, and potential efficacy of active rehabilitation, including aerobic training, coordination exercises, and visualization and imagery techniques with a physiotherapist among 19 adolescents with persistent postconcussive symptoms lasting >1 month after sports-related injuries compared to controls [16]. Choi et al. [17] found a significant ability of 30 minutees of virtual reality and 30 minutes of conventional occupational therapy to improve unimanual dexterity, activities of daily living, and forearm articular movement among 80 subjects versus controls. Carney et al. [18] found no significant difference between the standard care and family intervention group in terms of pediatric TBI postdischarge care. However, the children with better outcomes lived with their families and had better function at 6-month postinjury.
Kontosetal. [19] reported no significant changes in vestibular rehabilitation or control in 50 subjects. However, while both groups recovered similarly in terms of dizziness, the overall concussion versus behavioral management control group showed a more dramatic clinical improvement in vestibular items.
Hadanny et al. [21] reported that hyperbaric oxygen treatment and sham treatment improved cognitive performance, persistent PCS, behavioral symptoms, and quality of life in children aged 8–15 years. In another RCT, Kurowski et al. [27] reported a greater rate of improvement in the subsymptom exacerbation aerobic training group among 30 subjects versus controls. Bailey et al. [24] found significant improvement in the subsymptom threshold exercise program and control group at 6 weeks after removal of the influence of depression. McCarty et al. [23] showed that, after a collaborative care intervention reported 6 months after the baseline assessment, 13.0% of intervention patients versus 41.7% of controls reported high levels of postconcussive symptoms (P=0.03), and 78% of intervention patients and 45.8% of control patients reported a 50% reduction in depressive symptoms. Leddy et al. [25] reported that after aerobic exercise, children aged 13–18 years recovered faster (13 days) than those assigned to placebo-like stretching (17 days) (P=0.009). Dobney et al. [28] reported the feasibility of active rehabilitation (aerobic exercise, coordination drills, visualization, and education or reassurance) offered early (starting 2-week postinjury). Micay et al. [22] reported that the administration of an aerobic exercise intervention protocol appears safe and feasible for adolescents in the postacute stage of sports-related concussion recovery.
A further meta-analysis was performed of the 5 studies that reported postintervention PCSS results. Interestingly, the data were homogeneous. This was quite rational as all 5 studies employed a similar intervention (active intervention or occupational therapy). Fig. 3 reveals that active rehabilitation improved the PCSS score by 4.14 points, a statistically significant difference (P≤0.05). The I2 homogeneity test revealed homogeneity; therefore, a fixed-effects model was used. Fig. 4 shows that no publication bias existed in atleast 5 studies describing chronic intervention using rehabilitation or occupational therapy.
Forrest plot comparing active rehabilitation and control groups. SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom.
Funnel plot of publication bias detected in meta-analysis. SE, standard error; MD, mean difference.
7. Risk of bias
The risk of bias assessment is shown in Fig. 5. Of the 16 RCTs assessed using the RoB 2, 10 had a low risk of bias, 4 had some concern of bias, and 2 had a high risk of bias in at least 1 domain. The results are summarized in Fig. 5.
Risk of bias assessments of randomized controlled trials by Cochrane risk of bias tool for randomized trials.
Discussion
Pediatric TBI is a global phenomenon, with concussion constituting >80% of cases. More children are affected by concussions than adults, mainly owing to the different activities and behaviors of children and adolescents [29]. Despite the high incidence of concussions in children, published research on the nonpharmacological management of this common medical condition is lacking; thus, management more often involves pharmacological interventions. This review aimed to evaluate the role of nonpharmacological interventions in managing concussions based on RCT findings. The heterogeneity of concussions is the main obstacle to a clinically meaningful recommendation; however, we summarized several nonpharmacological interventions that might be beneficial for treating concussions in the acute or chronic phase.
1. Nonpharmacological management of concussion in acute care setting
Based on the findings of the current and previous RCTs, rest is important in the acute management of pediatric patients [20,24]. Two RCTs recommended strict rest for 5 days as an intervention in pediatric patients who had symptoms following acute concussion. However, strict rest did not improve outcomes and may have contributed to increased daily symptoms and slower symptom resolution. Rather, the best strategy is the current usual care (rest for 1–2 days with a stepwise return to activity). However, the International Concussion in Sports Group and the Centers for Disease Control and Prevention recommend complete cognitive and physical rest for the first 24–48 hours after sustaining a concussion, followed by a structured return to activity. The manner in which activities are considered cognitive rest during the acute recovery period is subject to variations in practice and guidelines, e.g., screen time abstinence is often interpreted as an example of cognitive rest.
Concussions cause a cascade of complex, overlapping, and disintegrative processes in the brain. These changes are caused by numerous pathophysiological processes, inluding ionic fluctuations, neural structural damage, neuroinflammation, an increased release of extracellular neurotransmitters, and reduced cerebral blood flow. Although recent human studies have shown that these processes may return to normal, the recovery of each may occur over a specific period and is probably affected by several factors [30].
Adequate recovery time following concussion should occur; however, early integration into regular physical activity that does not worsen outcomes should be considered to facilitate a proper healing environment. The possible adverse effects of prolonged activity restrictions should be considered when prescribing rest for more than a few days, such as in school-aged children. It is logical that a long rest period, especially in adolescents, can lead to deconditioning, which in turn can lead to changes in cerebrovascular control. However, these changes lead to other symptoms independent of the initial injury [31].
2. Nonpharmacological management of concussion in chronic care setting
Thirteen RCTs investigated the effects of nonpharmacological treatments on concussions. Studies have reported the efficacy of aerobic exercise, active rehabilitation, vestibular rehabilitation, virtual reality, family intervention, hyperbaric oxygen therapy, collaborative care, soft-tissue release, mobilization and/or thrust manipulations, oculomotor control, neuromotor control, and balance exercises.
Based on these findings, aerobic exercise is the most commonly reported nonpharmacological approach to managing concussion. Three reports showed that patients assigned to aerobic exercise (intervention group) had significant symptom improvement compared with those assigned to stretching (control group) [22,25,27]. All 3 studies had a low risk of bias; nonetheless, 2 were relatively small. Moreover, all studies used different methods of aerobic exercise, interventions, and follow-up durations.
Two RCTs used active rehabilitation consisting of aerobic training, coordination exercises, visualization, and imagery techniques with a physiotherapist [16,28]. Chan et al. [16] showed the safety, tolerability, and potential efficacy of active rehabilitation for adolescents with persistent postconcussive symptoms. According to Dobneyetal. [28], active rehabilitation can be started as soon as 2-week postinjury.
The efficacy of vestibular rehabilitation was demonstrated in one RCT in the context of vestibular dysfunction [19]. Vestibular rehabilitation uses central mechanisms of neuroplasticity (adaptation, habituation, sensorial, and functional substitution) to increase static and dynamic postural stability and improve visual–vestibular interactions [32].
Four RCTs found that visual rehabilitation improved visual symptoms. Vision therapy improves communication between the eyes and brain through various exercises led by the provider. Vision therapy involves a range of techniques aimed at promoting binocular vision and enhancing visual processing, tracking, and perception using diverse approaches and exercises. Most of these therapies lack specificity, and a subset of vision therapy practitioners assert that these visual impairments serve as underlying factors for numerous learning problems observed in youngsters [23]. The implementation of vision therapy can enhance several visual skills, including eye tracking, focus, eye-teaming, depth perception, and hand-eye coordination.
The strength of our study was its limited meta-analytical design. We demonstrated the interesting roles of rehabilitation and occupational therapy in pediatric concussion management. We also identified several interesting nonpharmacological approaches. This was an improvement on the scoping review performed by Dobney et al. in 2017 [33]. We confirmed the conclusion of Dobney in that anaerobic exercise is a promising concussion treatment strategy. Finally, further research with robust methodologies, larger samples, and a multicenter design is necessary to enhance the level of evidence.
3. Study limitations
The main limitation of this review was the notable interstudy heterogeneity in the outcome measures, diagnosis, duration of intervention, and treatment, which limited the meta-analysis. Nevertheless, we were able to pinpoint a possible approach to performing a meta-analysis that revealed an interesting finding. In addition, most of the studies were performed at single centers. The diagnosis of concussion is largely based on clinical competence, which includes an assessment of the patient's history of present illness, a comprehensive systems review, and a thorough physical examination. Numerous assessment tools were used in these studies, such as the Sports Concussion Assessment Tool (SCAT), now in its fifth edition, and the associated Child SCAT5 (for use for children aged 5–12 years). These tools may be used on the sidelines or in the clinic to support or refute the diagnosis of concussion. Although such essential tools may greatly assist decisions, they are neither essential nor conclusive for diagnosing concussions. Moreover, the eligibility criteria were limited to studies published in English and a comprehensive search being conducted of only 4 databases.
Conclusion
This systematic review highlights the importance of nonpharmacological therapy in managing pediatric concussion. Active rehabilitation in the chronic care setting may enhance patient prognosis. We also identified several interesting approaches that could be employed to ensure improving patient quality of life. However, this systematic review highlights the scarcity of high-quality literature substantiating the present therapeutic practice in the nonpharmacological care of pediatric concussions. Although there have been some instances in which nonpharmacological interventions have shown effectiveness, the variability in their implementation and the range of outcomes they target make it difficult to translate their use into clinical practice. Thus, there is a need to promote multicenter research in multiple countries to address this pervasive global health issue.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contribution
Conceptualization: AMPS, RSI, ST; Data curation: AGMG, MG, FK, E; Formal analysis: AI, AGMG, MG, FK, E; Funding acquisition: None; Methodology: AMPS, RSI, ST, AI; Project administration: AMPS, AGMG, MG, FK, E; Visualization: AMPS, AGMG, MG, FK, E, AI; Writing - original draft: AMPS, AGMG, MG, FK, E, AI; Writing - review & editing: AMPS, AI, RSI, ST, AGMG, MG, FK, E