Association between maternal weight gain during pregnancy and child’s body mass index at preschool age
Article information

Abstract
Background
Recent studies reported that prepregnancy body mass index (BMI) and weight gain during pregnancy affect birth weight and contribute to childhood obesity. However, no such data are available in Korea.
Purpose
This study gathered data on weight gain during pregnancy and its impact on birth weight and childhood obesity in Korea.
Methods
We reviewed 1,753 singleton full-term babies born at CHA Bundang Medical Center in 2014–2016. We first review each maternal and baby factor based on prepregnancy BMI (underweight, normal, overweight/obese) and then divided them into low, normal, and excess gestational weight gain (GWG) groups based on the American Institute of Medicine (IOM) guidelines. We reviewed the characteristics of each group and analyzed the association between maternal GWG based on IOM guidelines and child BMI after 6 years.
Results
The maternal prepregnancy BMI group showed a significant difference in birth weight and child BMI at 6 years. As the prepregnancy BMI increased, the birth weight and BMI at 6 years also increased (P<0.001). Mean birth weight and child BMI at 6 years differed significantly among the GWG groups. Furthermore, excess postpartum weight gain increased the risk of childhood overweight and obesity (odds ratio, 2.21; 95% confidence interval, 1.40–3.49).
Conclusion
Excess weight gain during pregnancy should be avoided due to its short- and long-term association with childhood obesity. Owing to the high prevalence of excess GWG and childhood obesity, excess weight gain during pregnancy can have significant public health implications.
Key message
Question: What are the risk factors of newborn birth weight? Does gestational weight gain and prepregnancy body mass index affect childhood weight?
Finding: Excess maternal weight gain increases the risk of overweight/obesity, newborn birth weight, and child body mass index at 4–6 years.
Meaning: Maternal weight control before and during pregnancy should be well controlled.
Graphical abstract. BMI, body mass index; CI, confidence interval.
Introduction
Globally, the prevalence of overweight and obesity in childhood and adulthood is increasing. Hence, further research is needed to understand the origins and the critical time periods that could increase the risk of obesity and adverse health outcomes later in life. Over the many years in America, overweight and obesity rates in women of reproductive age have increased rapidly [1]. The prevalence of overweight and obesity before pregnancy among women who gave birth increased from 23.2% in 1993–1994 to 44.8% in 2009 [2,3]. Another important issue for pregnant women is that excessive pregnancy weight gain is becoming more common among women with high prepregnancy body mass index (BMI) [4].
Evidence shows that maternal overweight and obesity have long-term health consequences on the offspring’s later health. These associations are stronger with maternal than paternal obesity, suggesting that they cannot solely be explained by a common genetic background. Maternal and fetal well-being is directly coupled. The optimal fetal growth is influenced by several factors. These factors control the fetal metabolic signaling pathways and guide “fetal programming” through an intricate mechanism. Recent studies suggest that “fetal origin” effects can be extended to a wider range of lifelong outcomes, particularly poor health at birth is a major pathway by which insufficient or excessive nutritional intake exerts lasting effects during fetal development [5,6]. This study will shed new light on such a pathway since GWG is a good measure of nutrition in utero and both high birth weight and low birth weight are the crucial indicators of poor infant health.
Many studies have shown that both prepregnancy BMI and GWG are the 2 key determinants of infant health [7]. There is a growing association between prepregnancy BMI and large gestational age (LGA) outcomes which have also been observed in other studies. Furthermore, BMI>85th percentile at birth is independently associated with being overweight at 4 years [8]. Newborn overweight is perhaps superior to newborn macrosomia in predicting overweight at age 4. This suggests that early ‘adiposity rebound’ may lead to adult obesity. We want to know that an LGA newborn of obese mothers has the potential to track into later life and confer negative effects on their future body composition and, thus, metabolic health.
So firstly, we intended to evaluate the effects of prepregnancy BMI and GWG on the infant’s birth weight. Secondly, we wanted to investigate such programming using the body composition data from birth and at ages 4–6 of Korean children born to obese mothers.
Methods
1. Study population
We reviewed the data of 6,669 babies born at the Bundang CHA Medical Center from January 2014 to December 2016. We excluded 1,761 preterm babies (under gestational age [GA], 37+0 weeks) and 1,245 twin babies from the study. We collected the medical data of 1,753 normal singleton and full-term babies eligible for this study (Fig. 1). We obtained information about the maternal and baby factors via electronic medical records. For the maternal factors, we collected age, weight before the pregnancy, total weight gain during the pregnancy, height, and BMI before and after the pregnancy. Prepregnancy weight and height were self-reported by mothers, and during pregnancy, body measurements were taken on the first day of pregnancy and the day of delivery at the hospital. We collected the birth weight and height, infant sex, and the delivery method for the baby factors. Furthermore, out of 1,753 babies, we confirmed a BMI of 473 at ages 4–6 years during their vaccination visit.

Schema of participant selection process. BMI, body mass index; GA, gestational age (weeks). a)BMI 25–29.9 kg/m2 and BMI >30 kg/m2 groups combined.
2. Measurements
We used the prepregnancy weight and height self-reported by mothers to calculate the BMI (kg/m2). We categorized it according to the World Health Organization guidelines [9] as group 1: underweight (BMI<18.5 kg/m2), group 2: normal weight (BMI 18.5–24.9 kg/m2), group 3: overweight (BMI 25.0–29.9 kg/m2) and obese (BMI≥30 kg/m2) (Fig. 2). The weight at delivery was measured at the hospital and used to calculate the GWG by subtracting it from woman’s prepregnancy weight. For further statistical evaluations, we combined the overweight and the obese groups due to the small sample size in the obese group. The proper GWG for underweight, normal weight, overweight and obese women is 12.5–18 kg, 11.5–16 kg, 7–11.5 kg, and 5–9 kg, respectively, based on the American Institute of Medicine (IOM) recommendations [10]. We divided them into 3 groups based on gestational weight gain specified in the IOM guidelines: low GWG, normal GWG, and excess GWG (Fig. 2).
Percentage of women in each body mass index class based on the American Institute of Medicine (IOM) gestational weight gain category.
3. Statistical analysis
The data are presented as mean, standard deviation, number, and rate (%). The chi-square test conducted comparisons of mean values of the categorical variables. The Kruskal-Wallis test was performed to show the relationship between prepregnancy BMI, maternal factors, and birth height. We used the Mann-Whitney test for post hoc analysis as the data showed nonnormal distribution. We used analysis of variance analysis for normal distribution variables to find the association between the prepregnancy BMI group and the birth weight and childhood BMI. The Bonferroni test was used for post hoc analysis. Furthermore, we used linear regression with log gamma function to calculate beta coefficients (β) and 95% confidence intervals (CIs) and odds ratio (OR) to describe the association between the prepregnancy maternal BMI, GWG, birth weight, and BMI at age 4–6. Adjusted β (aβ) were calculated to describe the relative risk and adjusted for GA (day), sex, maternal height, and birth weight. All analyses were performed using IBM SPSS Statistics ver. 26.0 (IBM Co., Armonk, NY, USA). In this study, probability (P)≤0.05 (2-sided) was considered statistically significant.
Results
1. Baseline characteristics
In this study, we had data from 1,753 mothers and newborn infants and 473 4–6-years-old children. Table 1 shows the different characteristics of a maternal and newborn infant by the prepregnancy BMI status. In the underweight, normal, and overweight/obese groups, the median prepregnancy BMI was 17.65±0.72, 21.02±1.63, and 28.19±2.93 kg/m2 (P<0.001), respectively, and the average birth weight was 3.08±0.35 kg, 3.19±0.37 kg, 3.33±0.39 kg (P<0.05), respectively. Both of these things in each group showed statistically significant differences. There was no significant difference in the infant sex (P=0.971) between the 3 groups. However, the ratio of cesarean section (c/sec) delivery was significantly higher than normal spontaneous vaginal delivery, which showed a statistical difference in group 3 (P<0.001).
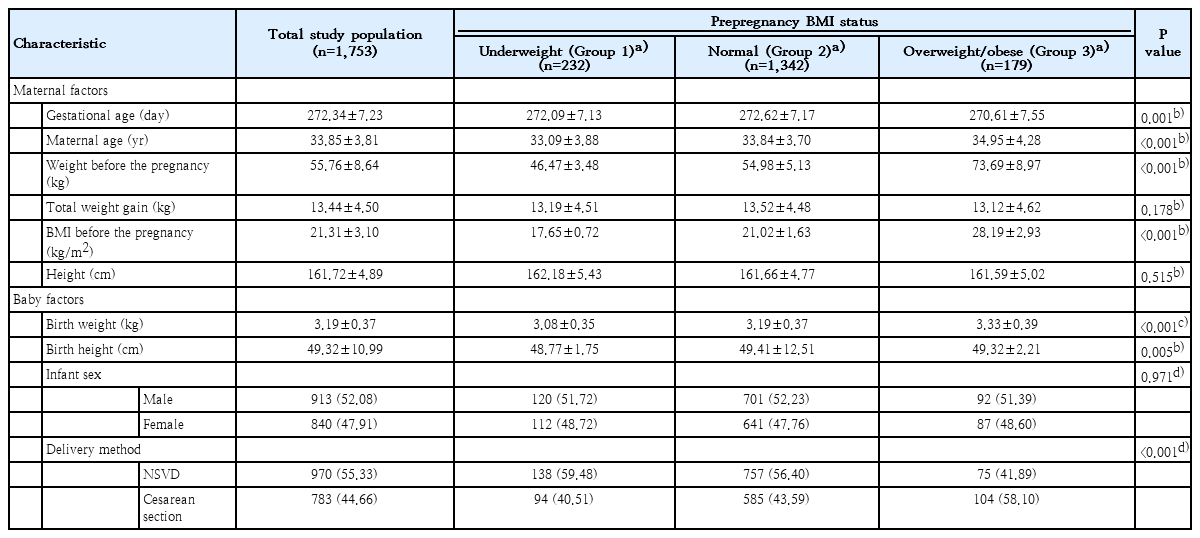
Characteristics and maternal prepregnancy BMI status of total study population
2. Maternal prepregnancy BMI vs. 4–6-years BMI
Table 2 shows the correlation between the maternal prepregnancy BMI and the child’s BMI at 4–6-year-old as well as the newborn infants’ birth weight. As the mother’s prepregnancy BMI increases, the infants’ birth weight increased (aβ=0.054; 95% CI, 0.037–0.072; P<0.001). BMI at 4–6-year-old also showed a positive correlation with the prepregnancy maternal BMI (aβ=0.059; 95% CI, 0.031-0.087; P<0.001).
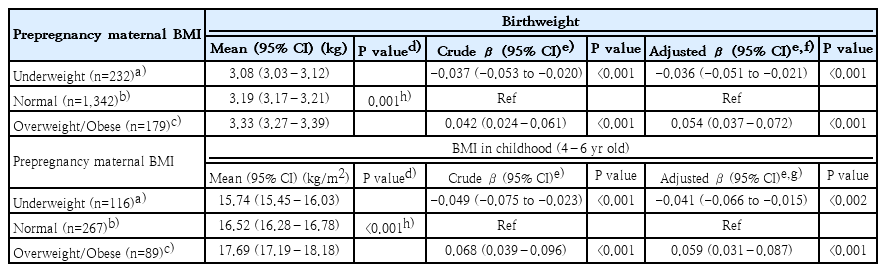
Association between maternal prepregnancy BMI and child’s BMI at 4–6 years (N=1,753)
3. Maternal GWG vs. newborn birthweight and 4–6-year-old BMI
The association between birthweight and BMI at 4–6 years of age and GWG based on the IOM guidelines are demonstrated in Table 3. Maternal weight gain during pregnancy shows a relationship between birthweight and BMI at age 4–6 years. Indeed, our data showed a relationship between GWG and birthweight and BMI at 4–6 years of age. GWG based on the IOM guidelines and the birthweight significantly increased in the excess GWG group than in the low and the normal GWG groups (aβ=0.050; 95% CI, 0.036–0.064; P<0.001). Also, the BMI at 4–6 year of age also showed the relationship with the excess GWG group (aβ=0.025; 95% CI, 0.005–0.045; P<0.015) (Table 3). The proportion of 4–6-year-old overweight/obese children showed the highest value in the excess GWG group and was statistically significant. After correcting for confounding variables such as GA (day), sex, maternal height, prepregnancy BMI, and birthweight, the overweight/obese ratio of children 4–6 years of age was statistically significantly higher in the excess GWG group (aOR 1.77; 95% CI, 1.09–2.88; P<0.021) (Table 4).
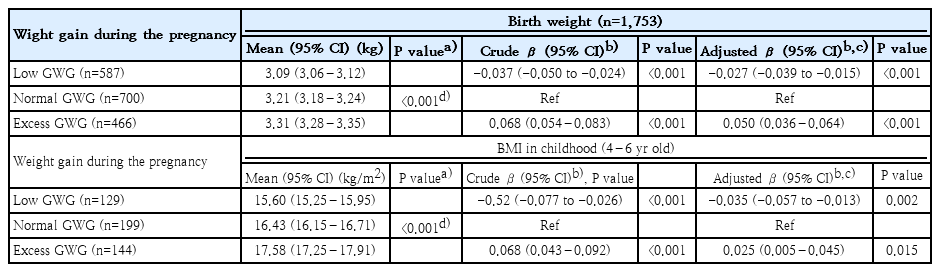
Association between weight gain during pregnancy, birth weight, and child’s BMI at 4–6 years
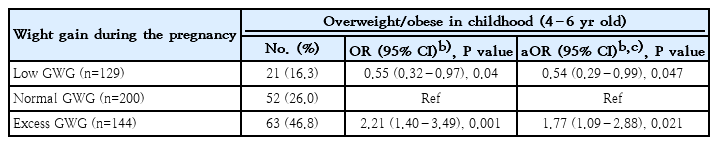
Association between weight at age 4–6 years and maternal gestational weight gain based on Institute of Medicine (IOM) guidelines
Discussion
Our study examined the associations between the maternal prepregnancy BMI and the infant’s weight at birth or the child’s BMI in childhood and between the maternal GWG and the infant birthweight or their child’s BMI in childhood. As the prepregnancy BMI increases, the birth weight significantly increases, even after adjusting for confounding factors. Furthermore, this study investigated the effect of the maternal prepregnancy BMI and GWG on the BMI at 4–6 years of age when the early adiposity rebound occurs. The overweight/obese children ratio in the excess GWG group was higher than in the low and normal GWG groups.
Worldwide, the prevalence of excessive gestational weight gain in women has increased, and much research about weight gain during prepregnancy increases body fat and birth weight [11-13]. Zhao et al. [13] found that overweight and obese women had a higher risk of developing macrosomia and LGA compared to women with normal weight. Nehab et al. [14] also found that children of mothers who gained excessive weight during pregnancy had increased body fat and birth weight. There have not been many studies about the relationship between weight gain during pregnancy and the child’s weight at 4–6 years when an early adiposity rebound occurs. So, in this paper, we tried to confirm that weight gain during pregnancy is associated with BMI at 4–6-year-old.
Several studies have linked fetal macrosomia with a higher risk of developing type 2 diabetes mellitus, obesity, and metabolic syndrome in childhood or adulthood, perpetuating this cycle in the next generation. Increasing maternal glucose and free fatty acids levels are related to maternal overweight and obesity proposed by the overnutrition hypothesis [15,16]. This may lead to permanent fetal body composition changes, in the long run, increasing the risk of obesity-related health outcomes later in the future [17]. Maternal body size closely relates to the infant’s birth size and also reflects maternal nutritional status long term [18].
Our study shows a relationship between the delivery mode and prepregnancy BMI. This demonstrates that the larger the baby higher the chance of being born by c/sec, which is consistent with previous studies. In a recent study from the United Arab Emirates, the prevalence of c/sec delivery (OR, 2.3) was higher in birth weight, more than 4,000 g (OR, 3.9) [19]. Sebire et al. [20] showed that the c/sec delivery rate in the very obese group was more than 20%, whereas it was only close to 10% in the normal weight group. Rutayisire et al. [21] reported the chance of overweight (OR, 1.24; 95% CI, 1.07–1.44; P=0.003), and obesity (OR, 1.29; 95% CI, 1.13–1.49); P<0.001) was remarkably related to c/sec in preschool children. In other words, as the mothers’ BMI increases, the possibility of c/sec increases, and c/sec affects childhood obesity as an independent factor; it may be predicted that the mother’s weight gain is the most important factor in preventing childhood obesity.
Sex differences in body weight and body fat development at a young age have been shown in previous studies [22,23]. Eriksson et al. [18] confirmed that a higher percentage of body fat in adulthood is associated with a higher birth weight in men born in women with high maternal BMI. However, Voerman et al. [24] studies did not reveal gender differences; this is maybe because fat and lean mass are not distinguished by BMI. Further studies on the causal relationship and underlying mechanisms of these relationships are needed [25].
As a result of this study, it was statistically confirmed that the maternal age increased as the prepregnancy BMI increased. It should be considered that the number of elderly mothers in Korea is recently increasing, which is also an important risk factor for childhood obesity in the future.
The present study has several limitations. First, the sample size of 4–6-year-old was relatively small either due to loss of follow-up after birth or because the child’s body weight data was missing. Second, the prepregnancy weight and height were self-reported, producing recall error and leading either to underestimation or overestimation of GWG. Third, it was a single-center study; hence the results may only represent Bundang CHA Medical Center. And finally, we did not consider gestational diabetes and other maternal medical issues which may affect the fetus. The strength of this study is that it was a long-term longitudinal study, and the sample size of the newborn baby was large.
In this study, we confirmed that the prepregnancy BMI and the maternal weight gain during the pregnancy affect the birth weight and the BMI at 4–6 years of age. GWG increases the risk of later childhood overweight or obesity at ages 4–6. Overall, it is worth noting that excess GWG may significantly impact public health due to the prevalence of obesity in children.
Acknowledgements
The authors are grateful to all participants in this study. We also thank the Department of Pediatrics, Bundang CHA Medical Center, for help with testing our study participants.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: SJJ; Formal Analysis: JS, YK; Investigation: JS, YK, JHK; Methodology: JS, JHK; Project Administration: JS, SJJ; Writing – Original Draft: JS; Writing – Review & Editing: YK, JHK, SJJ