




Graphical abstract
Introduction
It is well established that adhering to the recommended levels of physical activity, sedentary behavior, and sleep is associated with numerous health and well-being benefits among children and adolescents [1,2]. Collectively, these behaviors have been labeled 24-hour movement behaviors, as they span a continuum of intensity-based movement that is spread throughout the 24-hour period [3,4]. Based on evidence suggesting that 24-hour movement behaviors are associated with several health outcomes, internationally recognized guidelines, such as the world-first Canadian 24-Hour Movement Guidelines [1,2,5], provide specific cut-points for each behavior that are associated with health benefits.
Although evidence is largely lacking on the health benefits of 24-hour movement behaviors among children and adolescents in South Korea (Korea hereafter), an analysis of the 2016 Korea Youth Risk Behavior Web-based Survey (KYRBS) revealed that, among 50,987 adolescents aged 12–17 years, engaging in high physical activity and low sedentary behavior while obtaining adequate sleep was associated with favorable psychological well-being [6]. Despite these findings, low physical activity and high sedentary behavior have been consistently observed across the past decade among Korean children and adolescents [7-10]; these patterns were exacerbated by the coronavirus disease 2019 (COVID-19) pandemic [10]. Analysis of data from the 2019 (prepandemic) and 2020 (postpandemic) KYRBS [11] indicated a decrease in meeting physical activity (6.1% to 5.8%), sedentary behavior (32.2% to 20.2%), and sleep (19.6% to 19.4%) recommendations.
In addition to the impact of the COVID-19 pandemic, recent systematic reviews suggested that climate change may negatively impact the opportunity for physical activity [10,12]. Given the worsening air pollution in Korea, it is reasonable to anticipate a reduction in physical activity opportunities, with potential replacement by indoor sedentary activities, for Korean children and adolescents. This shift has been anecdotally described in the most recent Report Card of the physical activity of children and adolescents in Korea [10], which comprehensively evaluates physical activity–related indicators and sources of influence among Korean children and adolescents. In addition to the challenges associated with climate change, childhood obesity [13], environmentally induced health conditions such as allergic rhinitis and atopic dermatitis [14], deteriorating mental health [15], smartphone addiction [16], and antisocial behavior [17] are also emerging as major public health concerns for the Korean pediatric population.
With persistent and emerging public health challenges, thorough surveillance and monitoring of health-enhancing 24-hour movement behaviors and their interactions with various health and environmental outcomes can inform the development of future health promotion policies and practices for the pediatric population in Korea. However, up-to-date information is lacking that comprehensively summarizes the status of 24-hour movement behaviors among children and adolescents in Korea. Therefore, the objectives of this multiphase, multimethod, and integrative review were to: (1) summarize the global trends in the development of 24-hour movement guidelines, (2) investigate the status of the 24-hour movement behaviors in the Korean pediatric population, and (3) develop priorities and recommendations for future pediatric health promotion efforts in Korea.
Methods
1. Data sources
This integrative review included 3 phases involving different review methods to meet its objectives. Phase 1 was conducted in September and October 2023, while phase 2 was conducted in November and December 2023. Phase 3 was informed by the review data collected in 2021, with the results from the top-up database search conducted in January 2024 added to provide the most up-to-date information.
1) Phase 1: environmental scan
The first phase involved an environmental scan of literature to explore the global trend in the development of 24-hour movement guidelines. Because established guidelines to follow for conducting an environmental scan are lacking, we followed the “formal search” method first outlined by Choo [18] and used in previous studies [19]. For the environmental scan, we searched the scientific and grey literature in the MEDLINE and CINAHL databases that present 24-hour movement guidelines by country or organization of origin. Google Scholar was also searched to ensure that no relevant recent studies were excluded. The database search was conducted in September and October 2023 by one member of the research team (RJ) using the following keywords: 24-hour movement guidelines, movement behavio*, child*, youth, adolescen*, and movement behavio* recommendation. Only articles, reports, or websites published in English were retrieved.
2) Phase 2: rapid review
The second phase of this integrative review involved a targeted and rapid review of the comprehensive evaluation of the levels and trends of movement behaviors and sources of influence among Korean children and adolescents. Specifically, data from the Global Matrix Initiative in which Korea has been participating since 2016 were collected. Led by the Active Healthy Kids Global Alliance (AHKGA), a not-for-profit organization that promotes physical activity among children and adolescents worldwide, is a periodic initiative in which participating countries develop their own Report Cards on physical activity for children and adolescents [20]. Korea participated in the Global Matrix in 2016 [21], 2018 [22], and 2022 [20] (no initiative was conducted in 2020 because of the COVID-19 pandemic), in which 38, 49, and 57 countries participated in Report Card development, respectively. The Korean Report Card team primarily gathered evidence based on national surveys, independent studies, and government reports [8-10] to grade a number of common indicators, including physical activity, sedentary behavior, and sleep (2022 only) as well as sources of influence (i.e., family, peers, school, community, environment, and government). Briefly, a harmonized process was followed to provide grades for each indicator following the standardized grading framework and benchmarks provided by the AHKGA (Supplementary Tables 1 and 2). Detailed information about the Report Card and Global Matrix development processes is described elsewhere [20-23].
3) Phase 3: systematic review
The last source used to explore the current 24-hour movement behaviors among Korean children and adolescents was a systematic review of the relevant literature. The MEDLINE, PsycINFO, SPORTDiscus, Sports Medicine & Education Index, CHINAHL, and Embase databases were searched. The initial search was conducted in May 2021 as part of a major systematic review to investigate the levels and correlates of 24-hour movement behaviors among children and adolescents living in Asian countries [24]. Two top-up searches were conducted in January and June 2024 to identify the most up-to-date articles involving Korean children and adolescents regarding 24-hour movement behaviors. The search strategies used at each stage are listed in Supplementary Table 3. The study inclusion criteria were as follows: (1) participants aged 2–17 years and living in Korea, (2) provided adherence rate to the World Health Organization (WHO) or Canadian 24-Hour Movement Guidelines for children under the age of 5 years or for children and youth (5–17 years), and (3) published in a peer-reviewed journal in English. Studies were excluded if the sample or population had a known health condition except for being overweight/obese. Furthermore, studies were excluded if they did not report all 3 of the 24-hour movement behaviors. For example, if a study reported levels of physical activity and sedentary behavior but not sleep, it was excluded from the review.
2. Evidence synthesis
Data obtained from the environmental scan of scientific and grey literature on the existing 24-hour movement guidelines were synthesized with focus on key details such as country or organization of origin, year of launch/publication, and age-specific cut-points for physical activity, sedentary behavior, and sleep. Data from the Global Matrix, which included the 2016, 2018, and 2022 Korean Report Cards, were sourced from manuscripts published in peer-reviewed journals. The extraction process was conducted by one author (RJ), who systematically extracted and recorded the grades assigned to various common indicators with important background information. Specific details of the extracted data such as references, age groups, sample sizes, and indicators were comprehensively reviewed by the same author (RJ). To ensure accuracy and reliability, all of the extracted data were subjected to a rigorous verification process conducted by another author (EYL).
The levels of movement behaviors or adherence to any established age-specific movement guidelines identified in the first phase of this study (i.e., environmental scan) were summarized separately for physical activity, sedentary behavior, and sleep as well as the research articles identified through the systematic search. Sociodemographic correlates of meeting guidelines or movement behavior levels were also gathered during the data extraction process when provided by the searched articles. Two members of the research team (RJ, SP) conducted the data extraction with focus on key elements, such as representativeness (representative, nonrepresentative), age groups (7–12 years, 13–17 years, more than one age group), measurement method used (self-reported, proxy-reported, device-measured), sociodemographic correlates examined (yes, no), and study funding status (yes, no, unclear). Extracting information on funding availability aimed to shed light on the level of support for 24-hour movement behavior research within the nation.
All data used in this review were subjected to a two-step process encompassing both extraction (RJ and SP) and verification (SP or EYL) to ensure the robustness and integrity of the synthesized information. Averages were computed to indicate the levels of each movement behavior or adherence to the guidelines reported in multiple studies. In cases in which a study presented more than 2 values for different sociodemographic groups (e.g., adherence to guidelines among boys and girls separately, without overall adherence), a weighted average was calculated based on the sample size of each subgroup. The average adherence to the guidelines for each movement behavior was calculated by considering the varying sample sizes across studies. Consequently, the prevalence estimate derived from a study with a larger sample was assigned greater weight than that derived from a study with a smaller sample size.
Results
1. Phase 1: environmental scan
1) Summary of existing 24-hour movement guidelines worldwide
Table 1 provides an overall description of the existing 24-hour movement guidelines. Evidence supporting the 24-hour movement paradigm has led to the expanded development of integrated 24-hour movement guidelines. In 2016, Canada became the first country to release integrated 24-Hour Movement Guidelines for Children and Youth aged 5–17 years [1]. The development process was guided by 4 systematic reviews: 3 investigating the relationships between each movement behavior and health indicators [25-27] and one investigating the relationships between integrated movement behaviors and health indicators [28]. Shortly thereafter, governments of New Zealand [29] and Australia [30] released similar guidelines adapted from Canada’s guidelines that considered specific needs identified by a local research team [31]. Overall, although there are slight differences in the evidence used to inform the development, adoption, and/or adaptation of the guidelines and wording in examples or statements embedded within the guideline document, recommendations for healthy levels of physical activity, sedentary behavior, and sleep are essentially the same across countries. Specifically, for those aged 5–17 years, engaging in at least 60 minutes of moderate- to vigorous-intensity physical activity (MVPA) and no more than 2 hours of recreational screen time per day are recommended. Moreover, 9–11 hours of daily sleep for 5–13-year-olds and 8–10 hours of daily sleep for 14–17-year-olds is recommended.
For young children (those 0–4 years), the first 24-Hour Movement Guidelines were developed by the Canadian researchers in 2017 [2]. Immediately after their launch, Australia [32] and New Zealand [29] adopted these guidelines in 2017. Additionally, in 2018, South Africa collaborated with the guideline development team in Australia [31] to adapt the guidelines while considering the context of South Africa, primarily given its income level differences and extreme income inequality and poverty [33]. Similarly, researchers in the United Kingdom (UK) proposed the development of 24-hour movement guidelines for children younger than 5 years. However, the chief medical officers in the UK did not accept the integrated approach, specifically the recommendations for sedentary behavior, screen time, and sleep; as a result, only physical activity recommendations were released [34].
Based on the need to develop global integrated recommendations and following the WHO's Global Action Plan on Physical Activity, 2018–2030 [35], in 2019, the WHO developed global 24-hour movement guidelines for children younger than 5 years [36]. Subsequently, in 2020, the WHO released global guidelines for physical activity and sedentary behavior for children and adolescents (5– 17 years) [37]. All existing 24-hour movement guidelines (Table 1) are fundamentally identical, with only minor alterations in sedentary behavior recommendations. Specifically, the WHO did not make specific recommendations about sedentary behavior because of insufficient evidence to determine the specific optimal dose for health and low certainty about the relationship between sedentary behavior and health outcomes [37].
2) Adoption of WHO 2020 guidelines and new Physical Activity Guidelines for Koreans (revised edition)
In 2021, the Korea Health Promotion Institute [38] responded to the global action of integrating 24-hour movement behaviors into health promotion efforts by publishing a translated version of the WHO’s latest guidelines from 2020 [39,40]. However, this report encompassed only physical activity recommendations for 3 age groups (5–17 years, 18–64 years, and 65 years and older); recommendations for the youngest age group (0–4 years) have not yet been released despite the WHO providing recommendations for this age group [36]. Furthermore, the translated report [38] exclusively focused on recommendations for physical activity, overlooking the health implications of sedentary behavior and sleep as well as the significance of considering the integrated nature of 24-hour movement behaviors.
In 2023, Korea revised its 2012 Physical Activity Guidelines for Koreans and published the revised edition [41], which included recommendations for physical activity and sedentary behavior for young children (3–5 years) as well as older children and adolescents (6–18 years) (Table 2). These recommendations differ slightly from the previous version [42] and the 2020 WHO recommendations [39] to accommodate the local context. For example, the age grouping was adjusted to align with the lunar calendar-based age classification used in the Korean education system until June 2023 (Please note that there was a shift to the Gregorian calendar on June 28, 2023). Recommendations for the early years do not include infants (<1 year) and toddlers (1 to <3 years), and physical activity recommendations for 3–5-year-olds do not include specific time amount recommendation; rather, they include only activity types.
2. Phase 2: rapid review
Korea participated in 3 rounds of the Global Matrix, which provided a comprehensive evaluation of physical activity–related behavioral indicators and sources of influence. The main data sources used for grading are described in Table 3, while the grades assigned to each indicator for each round of the Global Matrix are listed in Table 4. As described in Table 3, data for 24-hour movement behaviors were derived solely from the most recent KYRBS in each round of the Global Matrix; therefore, it is important to acknowledge that the results of this review are only pertinent to children and adolescents aged 12–18 years. Furthermore, this study discusses only the changes in the indicators that provide grades across the 3 rounds of the Global Matrix. The sleep indicator, first considered in the 2022 Report Card, is not a formal part of the Global Matrix list of common indicators [20]. The grading rubrics and specific benchmarks for each indicator are available in Supplementary Tables 1 and 2.
1) Behavioral indicators
Among the 6 indicators included across 3 Global Matrices (2016–2022) [20-22], generally low or no grades due to incomplete data (“F” to “B+” with 5 “Incompletes”) were observed for Korean children and adolescents [8-10]. Of them, sufficient data were available for only 3 behavioral indicators over 3 rounds of the Global Matrix. Grades for overall physical activity dropped from a “D-” (20%–26% meeting the benchmark) in 2016 to an “F” (<20% meeting the benchmark) in 2018. The grade increased back to a “D-” in 2022, but this change was mainly attributable to the benchmark changes from ≥60 minutes of MVPA daily to ≥4 days per week to accommodate for when average per week data could not be estimated [10]. Active transportation generally received higher grades than other behavioral indicators because of the proximity between homes and schools for most children living in metropolitan cities [8]. Also, the grades for this indictor showed a ~20% net increase, progressing from a grade of “C+” (prevalence, 54%–59%) in 20168) to “B+” (prevalence, 74%–79%) in 2018 [9] and 2022 [10].
For sedentary behavior, the “F” (>20% meeting the benchmark) reported in 2016 resulted from inconsistencies in defining and operationalizing sedentary behavior [8], which was resolved in 2018 and 2022 based on updated benchmarks from the AHKGA (Global Matrix 3.0 in 2018 [22] and Global Matrix 4.0 in 2022 [20], respectively). Although the grades for sedentary behavior increased over time from “F” in 2016 to “D” in 2018 and 2022, it is important to note that smartphone use–based sedentary behavior was not considered in the grading because of the potential overlap with the recreational screen time items measured in the KYRBS. The amount of time spent on smartphone use is alarmingly high among Koreans, with an average of 315.3 min/d among 52,669 adolescents with significant gender differences (285.0 minutes/day for boys and 346.7 minutes/day for girls) [10]. In accordance with the 24-hour movement behavior paradigm, high levels of screen time may contribute to lower sleep levels among Korean children and adolescents. Thus, sleep was added as a new indicator for Korea’s Report Card in 2022 given its interrelationship with other behaviors within the 24-hour movement behavior paradigm [3]. In the 2022 Report Card, an “F” was given for the sleep indicator, with only 14% of children and adolescents the sleep recommendation [10].
2) Sources of influence
Of the 4 sources of influence indicators evaluated across the 3 rounds of the Global Matrix, school and government had complete grades over time, ranging between “D” and “A.” The school and government indicators improved significantly from the 2016 (“D” and “C,” respectively) and 2018 (“D+” and “D,” respectively) to the 2022 (“A” for both indicators) Report Card [8-10]. The improvement in the School indicator may be due to the newly developed curriculum of the Ministry of Education in 2018, which mandated the number of physical education (PE) classes for different age groups [9]. For the school and government indicators, the use of a standardized evaluation tool, the health-enhancing physical activity policy audit tool [43], which systematically evaluates school policies for the 2022 Report Card, likely contributed to the higher grades. However, assessing the quality of physical activity promotion programs and policies, as well as the translation of policy into action, would be beneficial for the future evaluation of these indicators. Although the community and the environment indicator was only evaluated in 2022 (“B-”), it is noteworthy that Korea is generally equipped with well-maintained and accessible indoor and outdoor physical activity facilities. However, climate change–related factors such as air pollution are mentioned as threats to physical activity participation among Korean children and adolescents [10].
3. Phase 3: systematic review
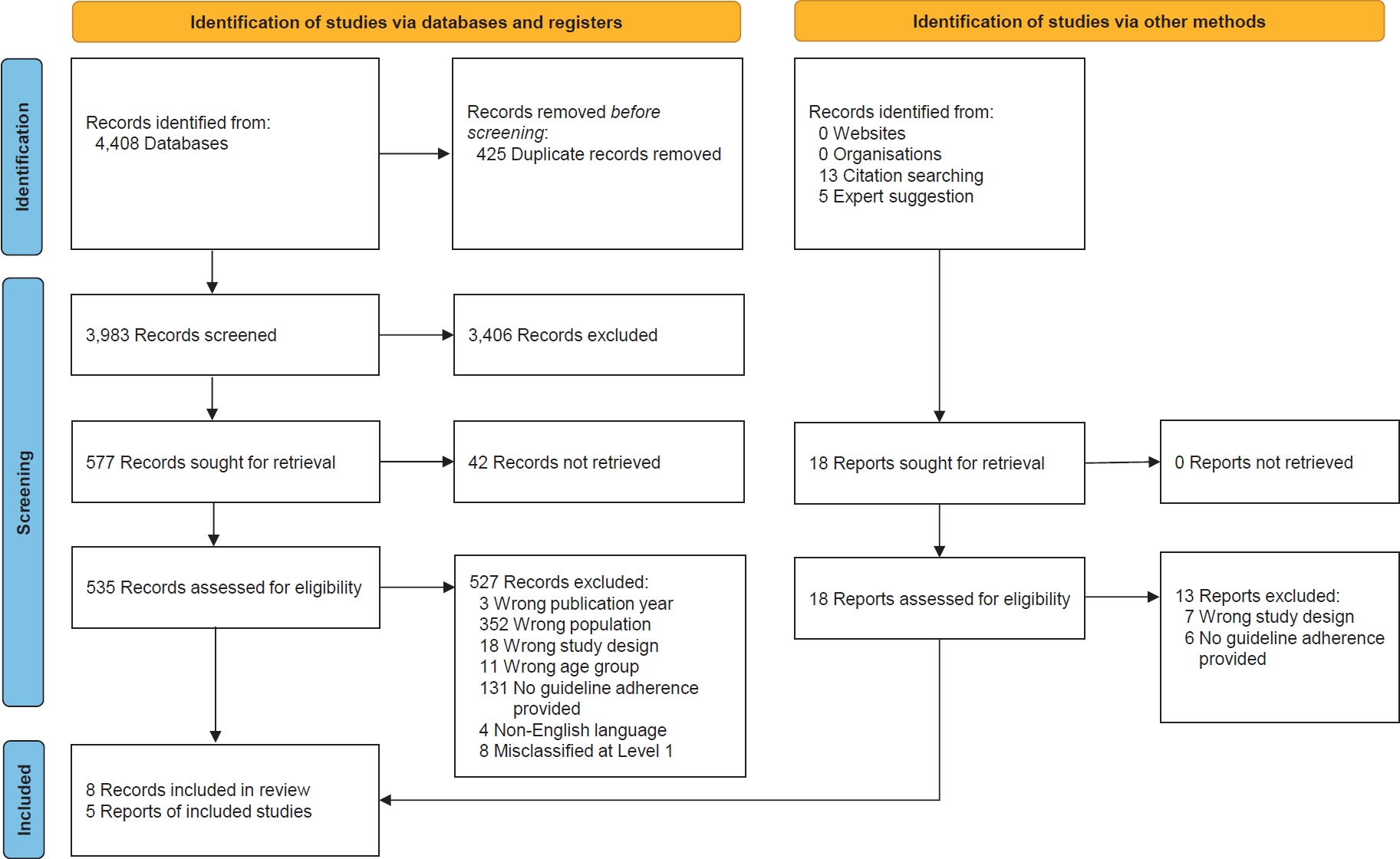
This review used data from an unpublished 2021 systematic review of the 24-hour movement behaviors among children in Asian countries [24] as well as a targeted top-up search conducted in January 2024. Of the 4,408 articles, 13 studies [6,7,44-54] involving data from 1,507,892 Korean children and adolescents aged 0–18 years met the inclusion criteria (Fig. 1). As shown in Table 5, 92% of the studies used representative data, such as the KYRBS or the Korea National Health and Nutrition Examination Survey (KNHANES), whereas one study used nonrepresentative data [52]. All 13 studies were either self-reported, proxy-reported, or a combination of the 2. Two studies involved children aged 0–11 years [52,53] whereas 11 involved children and adolescents aged 12–18 years [6,44-46,48-51,54]. Only 3 studies reported adherence to all 3 behavioral recommendations individually and collectively (i.e., meet physical activity, sedentary behavior, and sleep separately and together) [6,7,51]. Nearly half the publications stated that their respective studies received financial support.
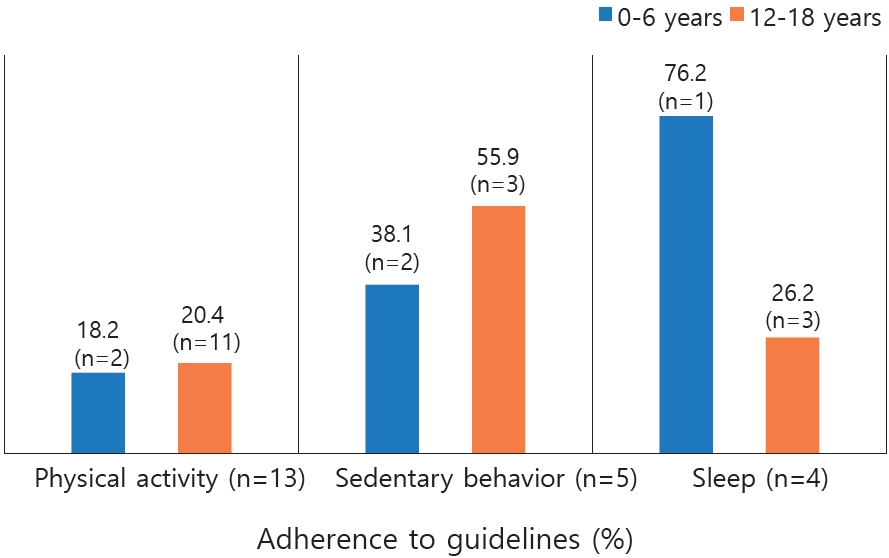
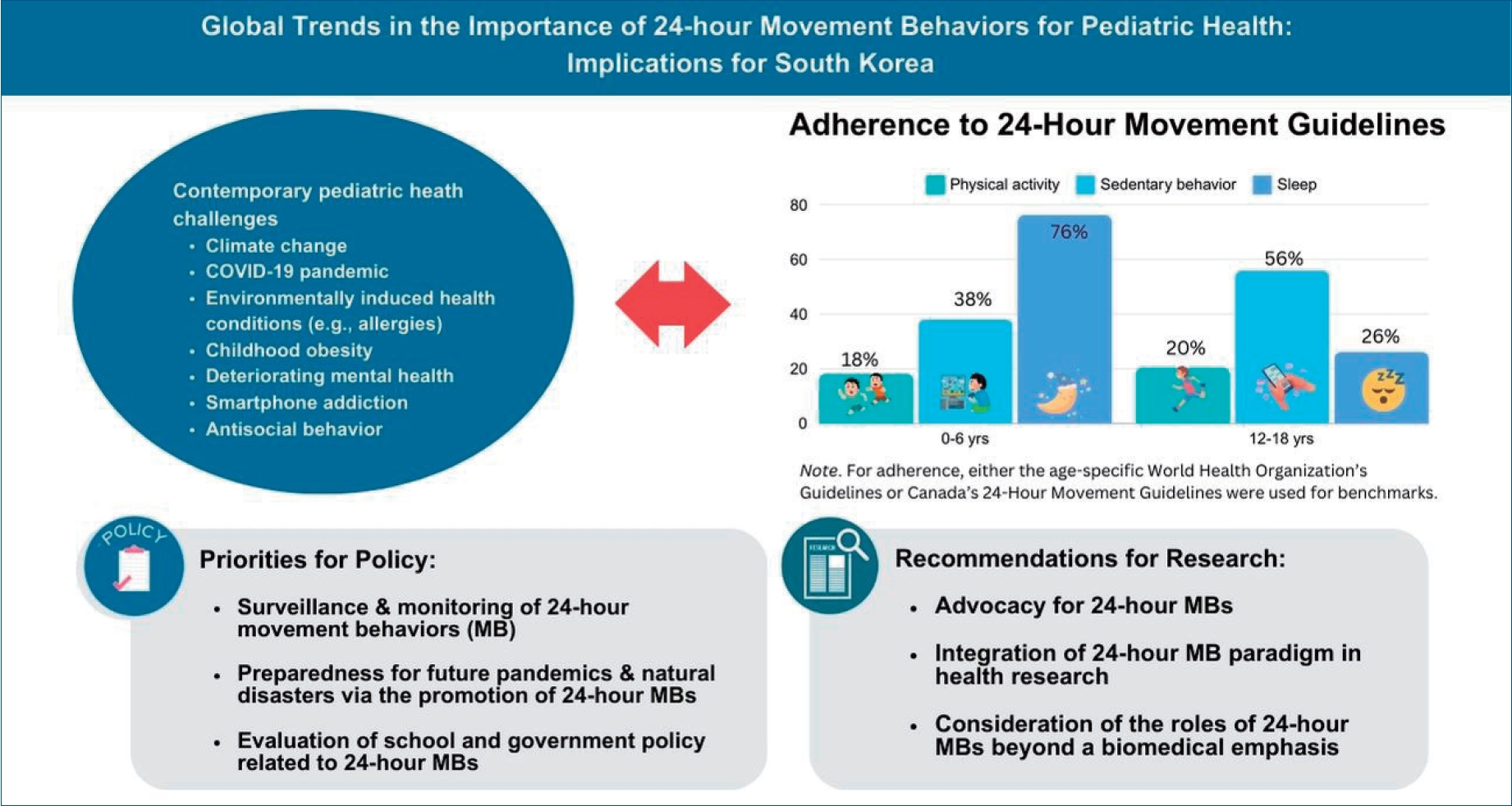
Fig. 2 shows the adherence to either the age-specific WHO [36] or Canadian guidelines [2]. Among individuals aged 0–6 years, the weighted averages for guideline adherence were 18.2% for physical activity, 38.1% for sedentary behavior, and 76.2% for sleep. For those aged 12–18 years, the weighted averages for guideline adherence were 20.4% for physical activity, 55.9% for sedentary behavior, and 26.2% for sleep.
Discussion
This multiphase multimethod integrative review aimed to provide an overview of global trends in movement behavior guidelines developed for pediatric population health (phase 1: environmental scan) and discuss the current status of 24-hour movement behaviors among Korean children and adolescents (phase 2: rapid review and phase 3: systematic review). Drawing on the insights gained from the 3 phases, this review presents the key priorities and recommendations for shaping future pediatric health promotion initiatives in Korea.
The growing recognition of embracing the integrated approach of the 24-hour movement behavior paradigm in pediatric health promotion [3] has led to the establishment and adoption of 24-Hour Movement Guidelines in different countries [1,2,31-33] and globally [36]. In response, the Korea Health Promotion Institute and Ministry of Health and Welfare took proactive measures by releasing a translated report of the WHO guidelines for physical activity and sedentary behavior [38] and the 2024 update of the Physical Activity Guidelines for Koreans [41]. A notable difference between global and other national guidelines [1,31,55] is the sedentary behavior recommendation. Specifically, guidelines developed in Korea do not provide specific cutoff points for sedentary behavior or screen time, potentially due to their link with the societal emphasis on education, which often involves prolonged sitting. Moreover, the absence of contextually relevant literature reflecting different types (e.g., active vs. passive) and domains (e.g., academic vs. nonacademic vs. leisure) of screen time among Korean children and adolescents might contribute to this omission.
Continuous surveillance and monitoring efforts of 24-hour movement behaviors in Korea spearheaded by governmental initiatives are ongoing. Utilizing nationwide data sources such as the KYRBS or KNHANES, a team of researchers, policymakers, practitioners, and stakeholders have developed biennial Report Cards on physical activity behaviors and factors of influence since 2016 (except for 2020 due to the COVID-19 pandemic) [8-10]. In the synthesis of previous Report Card data in 2016–2022 [8-10], both Overall Physical Activity (“D-” to “F”) and Sedentary Behavior (“D” to “F”) consistently received the lowest grades. Sleep, measured only for 2022 Report Card, also received an “F.” Persistently low grades for 24-hour movement behavior indicators were further emphasized in an analysis of Report Card grades in Asian countries [23]. Compared to the 17 Asian countries that provided Report Card grades [23], Korea consistently stood out for having lower grades across the 3 Global Matrix rounds for both Overall Physical Activity and Sedentary Behaviors.
These alarming results were evident in the systematic review conducted in phase 3 that consistently pointed out low adherence to guidelines among Korean children and adolescents, particularly to the physical activity recommendation for all age groups and the sleep recommendation only for those aged 12–18 years. Although not the focus of this review, complex relationships between 24-hour movement behaviors and prevalent contemporary behavioral and health issues have been noted. Specifically, smartphone use is negatively associated with physical activity [16,45,56]. Problematic smartphone use is a growing public health concern in South Korea. According to the 2020 KYRBS data involving those aged 12–18 years [45], 21.2% of boys and 30.0% of girls were at risk of excessive smartphone use. The COVID-19 pandemic may have also exacerbated addictive Internet use among Korean adolescents [57]. A 3-year longitudinal study indicated that as children aged, a reduction in physical activity contributed to increased smartphone dependency, which was subsequently associated with decreased subjective well- being [56]. This finding indicates that smartphone use, which serves as a proxy for sedentary behavior, and physical activity collectively and interdependently influence the subjective well-being of Korean children and adolescents.
In the following sections, we present the key priorities and recommendations derived from the outcomes of this comprehensive integrative review aimed at guiding future efforts to promote pediatric health in the context of health movement behaviors.
1. Priorities for health promotion policy and practice
Advancing assessments of 24-hour movement behaviors in surveillance and monitoring: Regularly assessing and reporting the prevalence and trends of 24-hour movement behaviors aligned with established behavioral recommendations is crucial for informing pediatric health promotion efforts. While the KYRBS and KNHANES provide valuable data, certain questionnaire items related to sedentary behavior deviate from internationally recognized recommendations with 2 significant implications. The KYRBS includes items that measure sedentary time, screen-based activities, and chatting with friends. However, evidence is lacking that sitting while engaging in in-person social behaviors, such as chatting with friends, is negatively associated with health outcomes; in fact, in-person social interactions are linked to improved health outcomes [58]. Not specifying the type of sedentary behavior in national surveillance may obscure data and prevent researchers from accurately identifying sedentary time that is potentially beneficial (e.g., social interactions) versus harmful (e.g., recreational screen time) to health. Second, the KYRBS includes separate questions on Internet and smartphone use. While this aids in capturing information on different types of screen-based sedentary behaviors, the lack of a clear distinction between overall sedentary time questionnaire items (which encompass time spent in front of a screen and chatting with friends, Internet use, and smartphone use) may contribute to the inaccurate reporting of each distinct aspect of sedentary behavior. Therefore, clarifying and refining these questionnaire items in future national surveys is essential to ensuring the accurate and meaningful reporting of sedentary behaviors and recreational screen time use in line with established guidelines. Improved surveillance will help identify at-risk groups needing more targeted support.
Evaluating the implementation of physical activity and sedentary behavior in schools and government policies: Previous Report Card findings indicated that existing national school and government policies support physical activity. Despite this, Korean children and adolescents consistently showed an unfavorable behavioral profile based on 2 decades of data. Due to the societal emphasis on educational success, a considerable amount of time is spent in schools and private institutions. Therefore, it is important to consider implementing comprehensive interventions in school environments to encourage active lifestyles. This includes enhancing PE programs and expanding physically active extracurricular activities. Indeed, the evidence provided in previous Global Matrix data serves as advocacy for the recent increase in PE hours among elementary and junior high school students [59]. Therefore, there is a need to evaluate the actual implementation of these programs and their direct impact on the health and well-being of children and adolescents in South Korea.
Building preparedness for future pandemics and natural disasters via healthy 24-hour movement behaviors: Our results indicate that the COVID-19 pandemic likely exacerbated the unfavorable behavioral profiles of Korean children and adolescents (i.e., decreased physical activity, increased sedentary behavior and screen time, and inadequate sleep). Furthermore, climate change–induced factors such as air pollution and extreme weather events are emerging barriers to physical activity since they interfere with outdoor activities that provide opportunities for structured (e.g., PE class) or non-structured (e.g., walking, playing) physical activity while promoting indoor-based sedentary behavior. To ensure timely and comprehensive pediatric health promotion efforts, it is important to establish robust strategies that enable children and adolescents to engage in healthy 24-hour movement behaviors, even in challenging circumstances. For example, developing contingency plans is crucial for guaranteeing the continuity of physical activity on days with poor air quality and extreme weather conditions. In addition, there is a need to integrate health promotion measures that are flexible and adaptable to ensure effectiveness under diverse challenging scenarios. Further more, resilience-building components through physical activity can be incorporated into health promotion programs aimed at equipping children and adolescents with coping mechanisms and preparing them to navigate stressors and challenges that may impact their movement behaviors, particularly via physical activity. This is pertinent given emerging evidence suggesting that physical activity may offer benefits for both health promotion and climate change mitigation efforts [60-62]. Improved 24-hour movement behaviors will yield Korean children and adolescents who are more physically fit, which in turn is associated with enhanced physical and mental resilience as ammunition against future pandemics and disaster challenges [63].
2. Recommendations for future research
Enhanced research funding and advocacy for 24-hour movement behaviors: These systematic review results indicate that less than half of the research projects secured funding. There is a critical need to pursue funding support for multifaceted initiatives spanning research, education, and community-based programs aimed at promoting healthy lifestyles among children and adolescents. This effort is essential for addressing existing gaps in knowledge and implementation. Moreover, it is important to engage in the robust advocacy of policies that prioritize and support pediatric health. This advocacy emphasizes the critical role of healthy movement behaviors in the holistic well-being of children and adolescents. Establishing a comprehensive framework that aligns financial support, research, and policy development will be instrumental in fostering healthy lifestyles among children and adolescents.
Embracing the 24-hour movement behavior paradigm in health research: Given that sedentary behavior recommendations within the updated Physical Activity Guidelines for Koreans [41] do not have specific cut-points, further investigation of the associations between sedentary behavior and varying health outcomes is warranted to inform future updates of the national guidelines. Considerations must be made regarding the nuances within different types of sedentary behaviors (e.g., sitting, screen-time academic vs. non-academic), different types of screen-based sedentary behaviors (e.g., academic vs. non-academic, social media use, TV watching, video-game playing), and screen-based behaviors performed while sitting or not sitting. This is particularly relevant, as the impact on health may vary based on specific behaviors, platforms, or contexts, emphasizing the need to disentangle the effects of screen-based activities from the broader category of sedentary behavior. For instance, the health implications of using social media while sitting might differ significantly from those of sitting alone, requiring nuanced exploration to inform comprehensive guideline updates.
Considering the role of 24-hour movement behaviors beyond biomedical emphasis: Recognizing the intricate interconnections between 24-hour movement behaviors and diverse health outcomes, it is important to extend our focus beyond the individual-focused biomedical emphasis of physical activity. Recent commentaries [60,64] on the contextualization of physical activity highlight the significance of behavioral scientists in transcending the traditional biomedical approach in research. There is growing emphasis on investigating the broader societal implications of physical activity by encompassing its potential role in addressing pressing social and environmental issues [60]. This expanded perspective considers how healthy movement behaviors may contribute to tackling challenges such as climate change, mental health concerns, social isolation, economic inequality, and community disconnection. Moreover, by aligning with fundamental health promotion goals [65] and fostering healthy community building, social cohesion, intergenerational bonding, and sustainability, physical activity emerged as a multifaceted catalyst for enhancing overall well-being and fostering resilient communities. Corresponding evidence for sedentary behavior and sleep is largely lacking and requires further development.
This integrative review provided a comprehensive overview of the 24-hour movement behavior paradigm and its implications for pediatric health promotion efforts in Korea as well as the most up-to-date evidence on the status of 24-hour movement behaviors among Korean children and adolescents. Nevertheless, it has at least a few limitations that must be acknowledged. First, our rapid review exclusively incorporated data derived from the Global Matrix Initiative. The development of each round of the Report Card engaged several researchers, policymakers, practitioners, and stakeholders in a comprehensive examination of the available evidence. However, it is essential to recognize that the process did not directly involve children and adolescents to capture their experiences and perspectives regarding various indicators. The inclusion of children and adolescents in future research could address this gap by providing valuable insights into the evaluation of policy implementation from their perspectives. Second, despite focusing on Korean children and adolescents as the target population, our systematic review did not include articles published in Korean. This decision on eligibility criteria was made to align data collection with phase 2 (rapid review). A brief search using the Korea Information Service System search engine on January 28 yielded 2 potentially relevant articles [66,67]. Upon closer examination, it was determined that the same data were utilized in the research articles [46,52]. included in this review. Consequently, articles in Korean were not included in this systematic review segment of this study.
To address the contemporary challenges confronting pediatric health in Korea, there is a compelling need to adopt the 24-hour movement behavior paradigm and integrate it into future health promotion efforts for children and adolescents. This was reinforced by the launch of the updated Physical Activity Guidelines for Koreans in 2023 [41], marking a critical milestone in shaping the approach to pediatric health. Combined with the unfavorable patterns of 24-hour movement behavior and worsening health outcomes frequently observed among Korean children and adolescents, it is important to provide sustained healthy promotion efforts to foster children and adolescents, encouraging them to incorporate consistent and healthy patterns of movement behaviors into their daily lives. This comprehensive integrative review, based on a thorough evaluation of the available literature, proposed 3 key priorities for policies and practices aimed at promoting pediatric health. Moreover, it postulated 3 recommendations for research aimed at providing the necessary evidence to build a healthier future for Korean children and adolescents.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


