Most downloaded
- Page Path
-
- HOME
- BROWSE ARTICLES
- Most downloaded
"Most downloaded" Articles are from the articles published in 2024 during the last six months.
- Review Article
- Infection
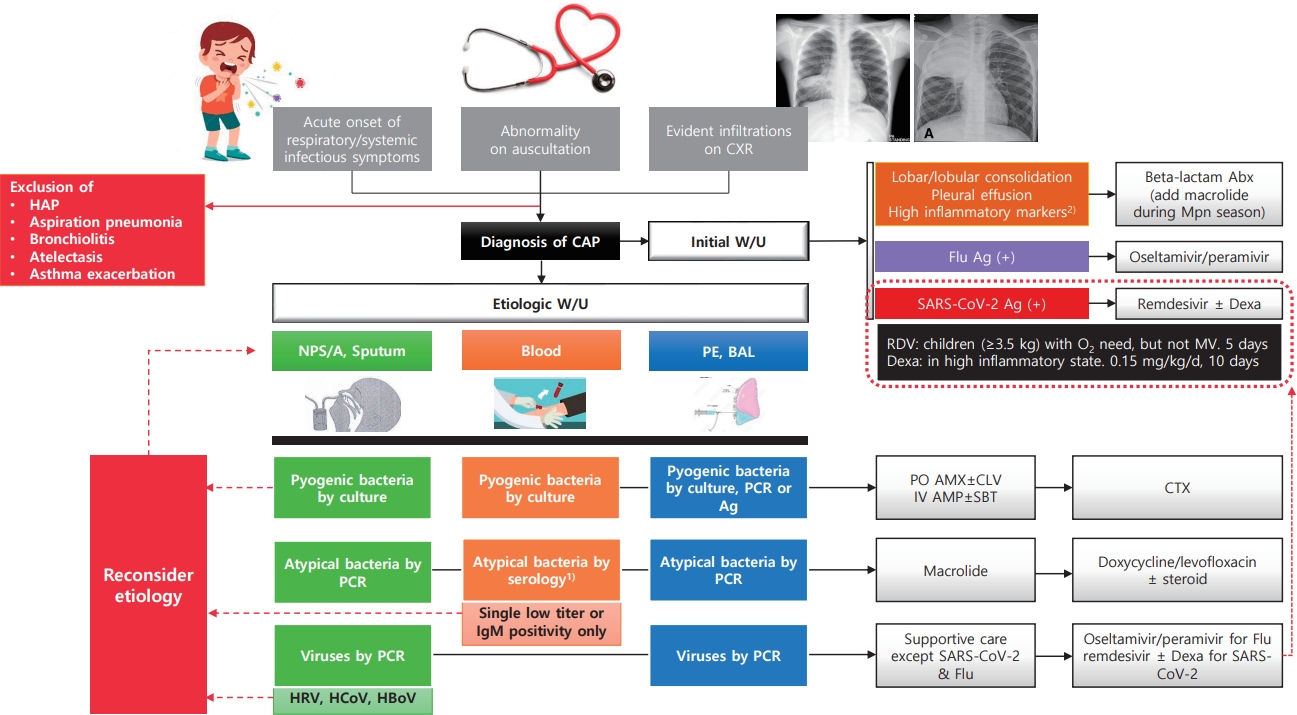
- Community-acquired pneumonia in children: updated perspectives on its etiology, diagnosis, and treatment
(372 times)
-
Ki Wook Yun
-
Clin Exp Pediatr. 2024;67(2):80-89. Published online June 14, 2023
-
|
· Most commonly confirmed causes of community-acquired pneumonia (CAP) in children are Mycoplasma pneumoniae (8%–40%) and respiratory syncytial virus (15%–20%).
· Pyogenic bacteria, most commonly Streptococcus pneumoniae (40%–50%) and Streptococcus pyogenes (10%–25%), are detected in 2%–5% of children hospitalized with CAP.
· CAP should be diagnosed conservatively according to clinical and radiological criteria.
· The etiology should be identified via appropriate test result interpretation. |
-
-
- Neonatology (Perinatology)
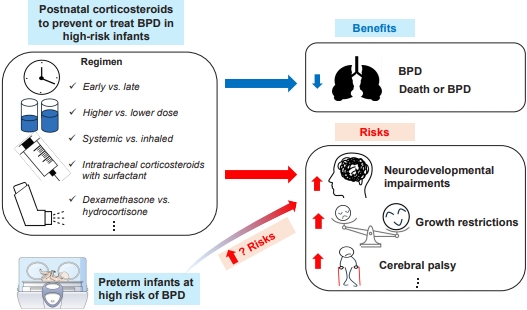
- Optimal postnatal corticosteroid regimens to prevent bronchopulmonary dysplasia with minimal adverse effects
(302 times)
-
Ga Won Jeon
-
Clin Exp Pediatr. 2026;69(4):293-300. Published online March 27, 2026
-
|
Postnatal corticosteroids facilitate ventilator weaning and reduce the risk of bronchopulmonary dysplasia (BPD). Despite being commonly used in high-risk infants, administration guidelines have not been established. Early dexamethasone may cause neurodevelopmental harm, and the optimal dosing remains uncertain. Inhaled corticosteroids show inconclusive benefits, whereas intratracheal administration with surfactant appears promising. Thus, corticosteroids should be used cautiously in high-risk, ventilator-dependent infants with severe BPD, and further high-quality trials are needed. |
-
-
- Original Article
- Developmental and Behavioral Medicine
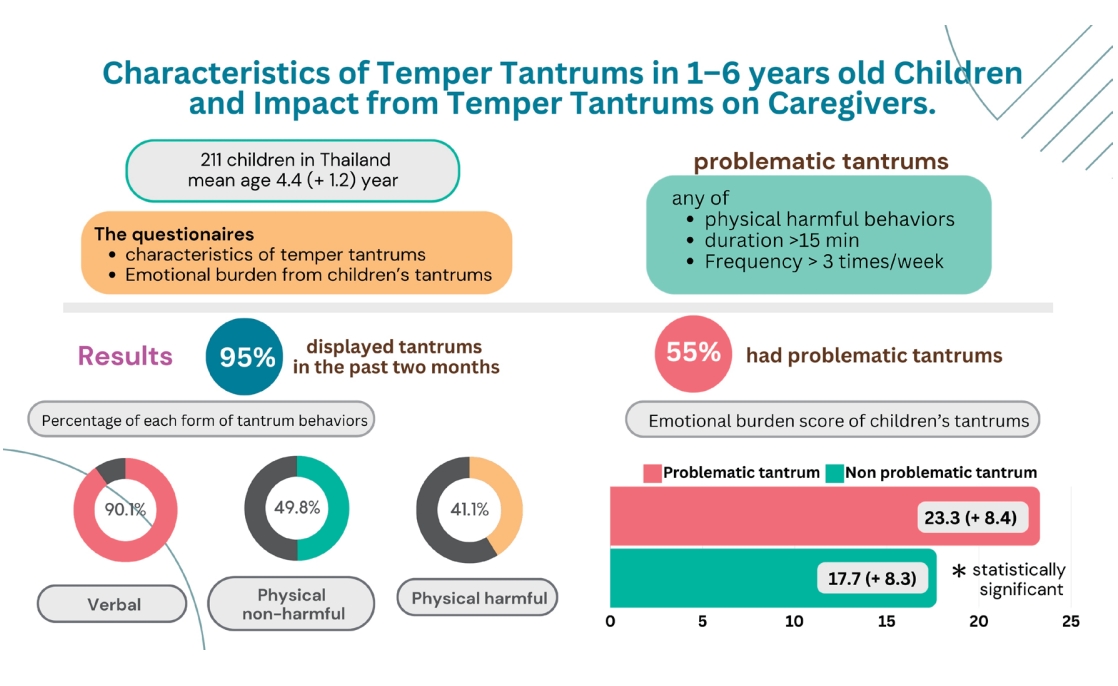
- Characteristics of temper tantrums in 1–6-year-old children and impact on caregivers
(274 times)
-
Warangkana Prutipaisan, Issarapa Chunsuwan, Tippawan Hansakunachai, Paskorn Sritipsukho
-
Clin Exp Pediatr. 2025;68(2):170-177. Published online November 13, 2024
-
|
Question: What are common tantrum behaviors in preschool children, and how frequently are problematic behaviors observed? Do problematic tantrums have a different emotional impact on caregivers compared to typical tantrums?
Finding: Temper tantrums are common in preschool children, and verbal tantrums are the most common type.
Meaning: Problematic tantrums, defined as tantrums exhibiting aggressive physical behavior, long duration (>15 minutes), or frequent occurrence (>3 days/wk), significantly affected caregivers’ emotions. |
-
-
- Review Article
- Gastroenterology
- Ingestion of foreign bodies and caustic substances in children: a narrative review on clinical evaluation and management update
(250 times)
-
Maria Rogalidou
-
Clin Exp Pediatr. 2026;69(1):11-21. Published online December 10, 2025
-

|
Foreign body and caustic substance ingestion in children aged 1–5 years can feature to severe and, sometimes life-threatening complications. High-risk items include batteries, magnets, and corrosive chemicals. Severity depends on object type, location, and ingestion timing. Prompt diagnosis and early endoscopic intervention are crucial. Individualized management, high clinical suspicion, and parental education are essential to improving outcomes and preventing immediate and long-term complications affecting a child’s quality of life. |
-
-
- Original Article
- Neonatology (Perinatology)
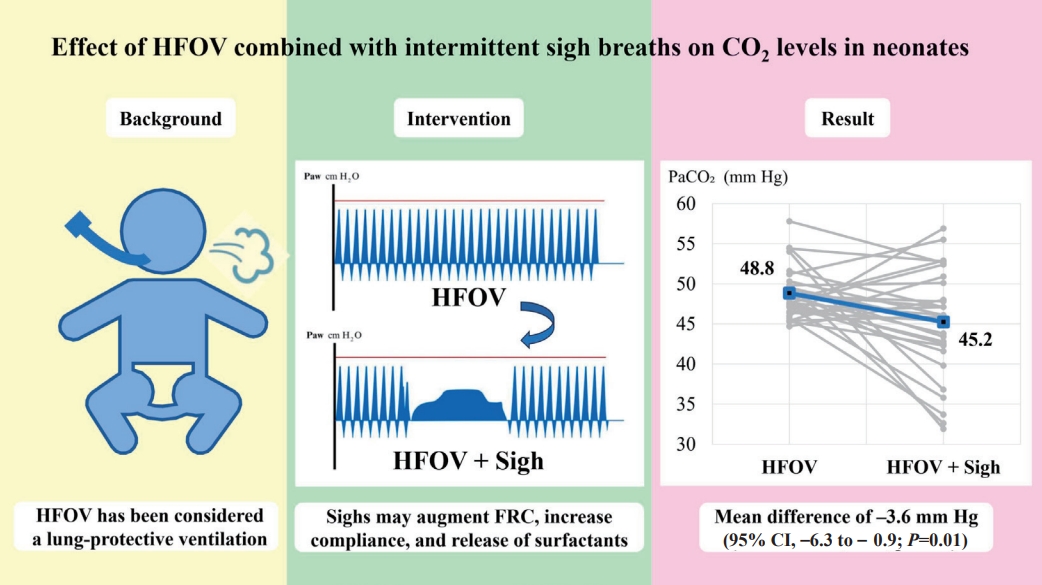
- Effect of high-frequency oscillatory ventilation with intermittent sigh breaths on carbon dioxide levels in neonates
(244 times)
-
Kulthida Baingam, Anucha Thatrimontrichai, Manapat Praditaukrit, Gunlawadee Maneenil, Supaporn Dissaneevate
-
Clin Exp Pediatr. 2025;68(2):178-184. Published online November 13, 2024
-
|
Question: Can sigh breaths (Sighs) application during high-frequency oscillatory ventilation (HFOV) decrease partial pressure of carbon dioxide (PaCO2) levels?
Finding: The mean PaCO2 level after Sighs during HFOV was significantly decreased compared to that after HFOV alone (mean difference, -3.6 mmHg).
Meaning: HFOV plus Sighs functionality can reduce PaCO2 levels. However, further studies are required to conclusively determine the effects of Sighs. |
-
-
- Characterization of gut microbiota in very low birth weight infants with versus without bronchopulmonary dysplasia
(224 times)
-
Anucha Thatrimontrichai, Manapat Praditaukrit, Gunlawadee Maneenil, Supaporn Dissaneevate, Kamonnut Singkhamanan, Komwit Surachat
-
Clin Exp Pediatr. 2025;68(7):503-511. Published online February 26, 2025
-

|
Question: Does the gut microbiota differ between very low birth weight (VLBW) infants with versus without bronchopulmonary dysplasia (BPD)?
Finding: Common respiratory pathogens were notably elevated in the BPD group, whereas anaerobic and butyrate-producing taxa, key components of postbiotics, were dominant in the non-BPD group.
Meaning: In gut-lung communication, the interplay between the intestinal and respiratory systems may implicate pro- and postbiotics in VLBW infants with BPD. |
-
-
- Review Article
- Developmental and Behavioral Medicine
- Comprehensive evaluation of the child with global developmental delays or intellectual disability
(222 times)
-
Abdullah Nasser Aldosari, T. Saeed Aldosari
-
Clin Exp Pediatr. 2024;67(9):435-446. Published online May 29, 2024
-

|
· A detailed history and comprehensive physical examination remain the cornerstones for establishing a diagnosis of global developmental delay/intellectual disability (GDD/ID).
· Comprehensive surveillance and screening programs play a significant role in the early detection of GDD.
· Whole-exome sequencing is highly recommended as first- or second-line testing for individuals with idiopathic GDD/ID.
· Early intervention by a well-versed multidisciplinary team can significantly improve the outcomes and prognosis of GDD/ID. |
-
-
- Original Article
- General Pediatrics
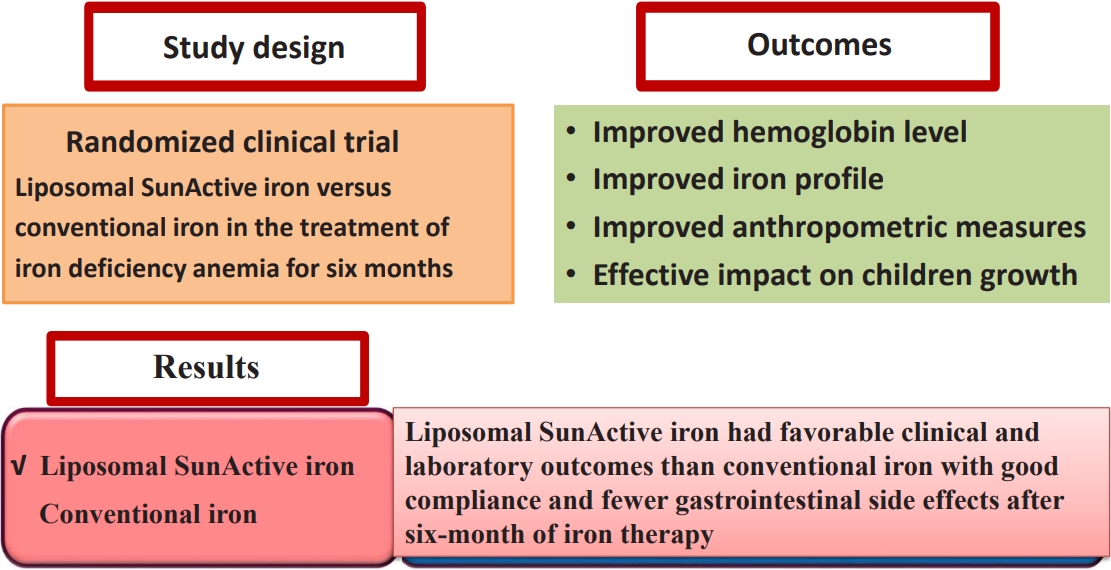
- Liposomal SunActive versus conventional iron for treatment of iron-deficiency anemia in children aged 2–12 years: a prospective randomized controlled trial
(214 times)
-
Wael A. Bahbah, Yasmin A.H.S. Younis, Hanan Salama Elbelouny, Asmaa A. Mahmoud
-
Clin Exp Pediatr. 2025;68(8):608-615. Published online July 18, 2025
-
|
Background: Liposomal iron, a novel oral formulation of ferric pyrophosphate that demonstrates improved gastrointestinal absorption and bioavailability with fewer side effects than conventional iron, represents a significant advancement in the treatment of iron-deficiency anemia (IDA).
Purpose: To conduct an in-depth comparative study of liposomal SunActive and conventional iron supplements (iron polymaltose complex) for treating IDA in children aged 2–12 years
Methods: This... |
-
-
- Original Article
- Neonatology (Perinatology)
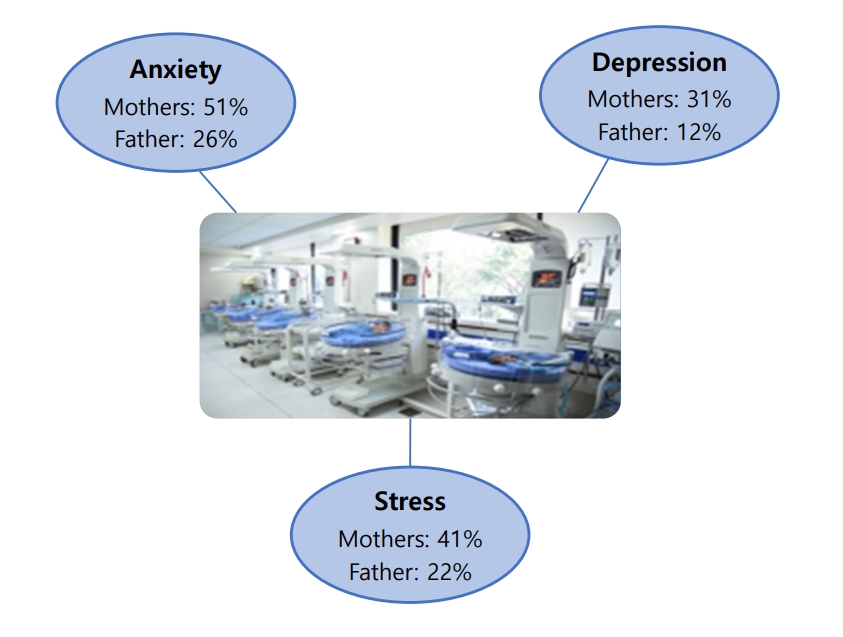
- Prevalence of anxiety, depression, and stress among parents of neonates admitted to neonatal intensive care unit: a systematic review and meta-analysis
(158 times)
-
Asha P. Shetty, Kurvatteppa Halemani, Alwin Issac, Latha Thimmappa, Sanjay Dhiraaj, Radha K, Prabhaker Mishra, Vijai Datta Upadhyaya
-
Clin Exp Pediatr. 2024;67(2):104-115. Published online November 14, 2023
-
|
Question: What emotions do parents experience when their newborns are admitted to the neonatal intensive care unit (NICU)?
Finding: Mothers experienced more anxiety (51%), depression (31%), and stress (41%) symptoms than fathers (26%, 12%, and 22%, respectively).
Meaning: Parents often experience anxiety, stress, and depression following NICU admission. Healthcare workers are responsible for providing regular parental counseling. |
-
-
- Review Article
- Developmental and Behavioral Medicine
- Clinical practice guidelines for attention-deficit/hyperactivity disorder: recent updates
(146 times)
-
Tae Hoon Eom, Young-Hoon Kim
-
Clin Exp Pediatr. 2024;67(1):26-34. Published online June 14, 2023
-

|
· Primary pediatricians should play a key role in the diagnosis and treatment of attention-deficit/hyperactivity disorder (ADHD).
· The Diagnostic and Statistical Manual of Mental Disorders, fifth edition, has lowered the diagnostic threshold for older teens and adults and a comorbid diagnosis with autism is now allowed.
· The American Academy of Pediatrics had added recommendation-related comorbid conditions in its guideline and the Society of Developmental and Behavioral Pediatrics recently developed a complex ADHD guideline.
· The European ADHD Guideline Group recently developed a guideline for managing ADHD during the coronavirus disease 2019 pandemic. |
-
-
- Original Article
- Neurology
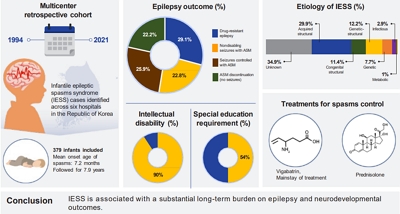
- Long-term outcome in children with infantile epileptic spasms syndrome: a multicenter retrospective study in Korea
(141 times)
-
Sun Ah Choi, Minhye Kim, Hye Jin Kim, Woo Joong Kim, Byung Chan Lim, Ji Yeon Han, Hunmin Kim, Min-Jee Kim, Mi-Sun Yum, Jiwon Lee, Jeehun Lee, Hyewon Woo, Jon Soo Kim
-
Clin Exp Pediatr. 2026;69(5):386-393. Published online February 19, 2026
-
|
Question: How have epilepsy and cognitive outcomes of children with infantile epileptic spasms syndrome (IESS) evolved over the past 20 years?
Finding: Approximately 78% of children developed chronic epilepsy, and one-third progressed to drug-resistant epilepsy, while 90% of them exhibited intellectual disabilities.
Meaning: Given the poor outcomes associated with IESS, consensus guidelines tailored to Korean clinical practice are required to ensure timely treatment and improve outcomes. |
-
-
- Review Article
- Neonatology (Perinatology)
- Updates in neonatal resuscitation: routine use of laryngeal masks as an alternative to face masks
(138 times)
-
Eun Song Song, Ga Won Jeon
-
Clin Exp Pediatr. 2024;67(5):240-246. Published online July 11, 2023
-

|
In neonatal resuscitation:
· Laryngeal masks are recommended when endotracheal intubation or positive-pressure ventilation fails.
· Laryngeal masks are useful even during chest compressions.
· Laryngeal masks aid neonates >34 weeks’ gestation and/or with a birth weight >2 kg.
· Main usage barriers include limited experience (81%), preference for endotracheal tubes (57%), and lack of awareness (56%).
· Second-generation laryngeal masks have a built-in esophageal drainage tube that prevents regurgitation into the glottis, and an orogastric tube can be inserted within the esophageal drainage tube to protect against gastric inflation. |
-
-
- Other
- Artificial intelligence in pediatric healthcare: current applications, potential, and implementation considerations
(135 times)
-
Taejin Park, In-Hee Lee, Seung Wook Lee, Sek Won Kong
-
Clin Exp Pediatr. 2025;68(9):641-651. Published online June 25, 2025
-

|
Artificial intelligence (AI) offers potential benefits in pediatric care, but its real-world adoption requires clinician literacy, ethical and legal safeguards, and cautious implementation. Large language models are emerging across healthcare, but their use in pediatric clinical practice remains premature. Thus, the cautious and accountable implementation of AI is crucial to preventing unintended harm and realizing its potential. |
-
-
- Neonatology (Perinatology)
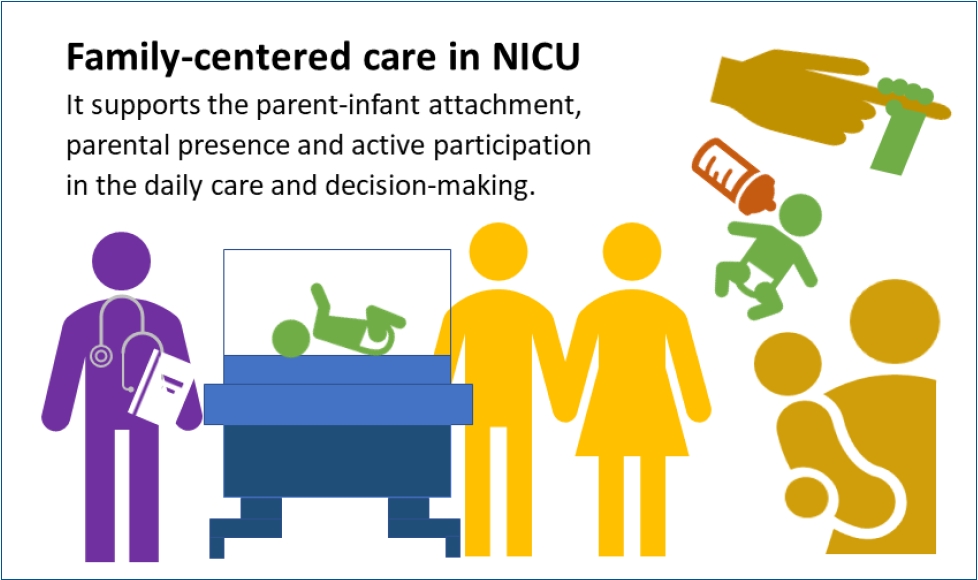
- Neonatal family-centered care: evidence and practice models
(133 times)
-
Juyoung Lee
-
Clin Exp Pediatr. 2024;67(4):171-177. Published online June 14, 2023
-
|
· Concrete evidence exists of early parent-infant attachment supported by family-centered care (FCC) in the neonatal intensive care unit.
· FCC involves the parents’ presence and participation in the infant’s care and decision-making.
· A private and comfortable space should be provided. A single-family room is ideal; however, a quiet space with a recliner can be a good alternative.
· Care culture changes and staff training are required. |
-
-
- Need for national guidance regarding proactive care of infants born at 22–23 weeks' gestation
(131 times)
-
Ga Won Jeon
-
Clin Exp Pediatr. 2025;68(1):53-61. Published online November 13, 2024
-

|
With advancements in neonatal intensive care, the limit of viability has shifted to 22–23 weeks' gestation, whose survival rates vary across countries and institutions. These rates are not static and can be improved through the proactive and centralized care guided by national protocols, including maternal transfer to high-activity regions with better neonatal intensive care practices before delivery. |
-
-
- Editorial
- General Pediatrics
- Artificial intelligence in pediatric healthcare: bridging potential, clinical practice, and ethical considerations
(125 times)
-
Yoon Lee, Seohyun Hong, Dong Keon Yon
-
Clin Exp Pediatr. 2025;68(9):652-655. Published online August 28, 2025
-

|
· Artificial intelligence (AI) holds transformative potential for pediatric healthcare, with applications spanning prevention, diagnosis, treatment, and follow-up across diverse subspecialties; however, ethical concerns, scarcity of pediatric- specific data, and limited funding remain significant challenges.
· International consensus on pediatric AI guidelines, expanding child-specific datasets, and incorporating explainable AI are essential to ensure safety and trust.
· Multicenter collaboration and increased investment can address these gaps, enabling equitable, reliable, and pediatric- centered AI solutions. |
-
-
- Neonatology (Perinatology)
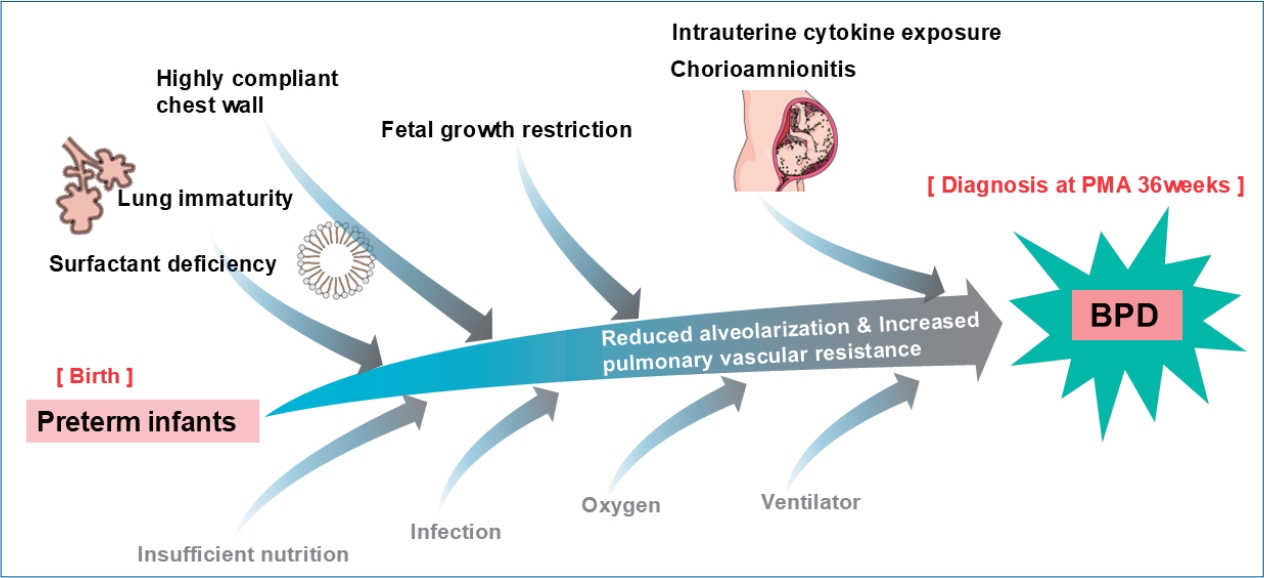
- Early prediction of bronchopulmonary dysplasia using new classification in high-risk preterm infants
(122 times)
-
Ga Won Jeon
-
Clin Exp Pediatr. 2026;69(3):211-213. Published online February 25, 2026
-
|
The definition of bronchopulmonary dysplasia (BPD) has continued to evolve. Recently, newer definitions based on respiratory support at 36 weeks’ postmenstrual age better predict long-term outcomes but diagnose BPD relatively late. To address this limitation, the New Japanese Classification uses early postnatal factors, including small for gestational age and bubbly or cystic chest radiographic findings, to predict severe BPD and enable early targeted interventions. |
-
-
- Review Article
- Gastroenterology
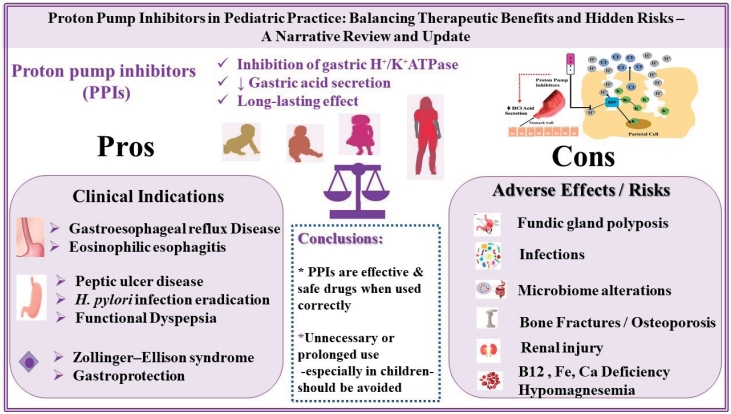
- Balancing therapeutic benefits and hidden risks of proton pump inhibitors in pediatric practice: a narrative review and update
(121 times)
-
Maria Rogalidou, Alexandra Papadopoulou
-
Clin Exp Pediatr. 2026;69(3):186-196. Published online February 25, 2026
-
|
Proton pump inhibitors (PPIs) effectively treat acid-related disorders, including gastroesophageal reflux disease, eosinophilic esophagitis, peptic ulcers, and Zollinger-Ellison syndrome. Long-term use, particularly in children, may lead to microbiome alterations, nutrient deficiencies, infections, renal injury, osteoporosis, fractures, and other gastrointestinal changes. PPI therapy should be guided by clear clinical indications, prescribed at the lowest effective dose for the shortest necessary duration, and regularly reassessed to minimize risks in young children. |
-
-
- Other
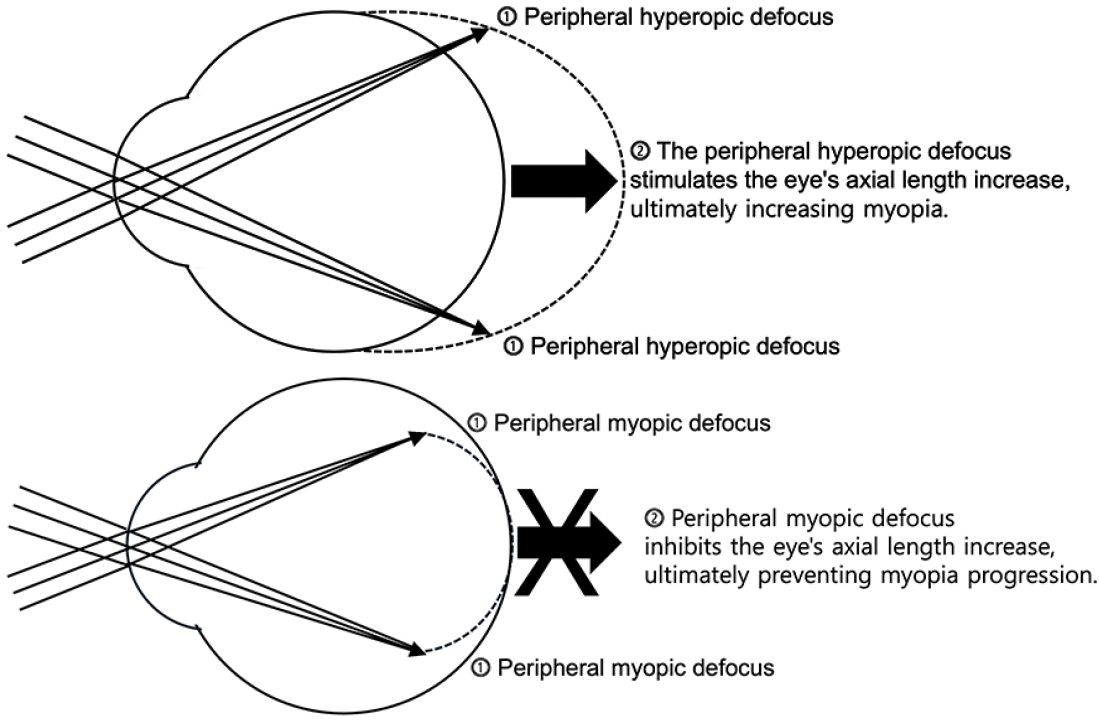
- Myopia: a review of current concepts, association with nonophthalmological conditions, and treatment strategy in children and adolescents
(120 times)
-
Yeon Woong Chung
-
Clin Exp Pediatr. 2025;68(8):554-565. Published online April 1, 2025
-
|
Myopia is a major ophthalmological disorder with increasing prevalence worldwide, particularly in East Asia. Evidence indicates that its development involves complex interactions between genetic and environmental factors. Body stature, sleep patterns, and nutritional status significantly influence the progression of myopia during childhood and adolescence. Its treatment and prevention strategies include optical correction, atropine therapy, increased outdoor activity, decreased near work, and regular retinal monitoring. |
-
-
- Cardiology
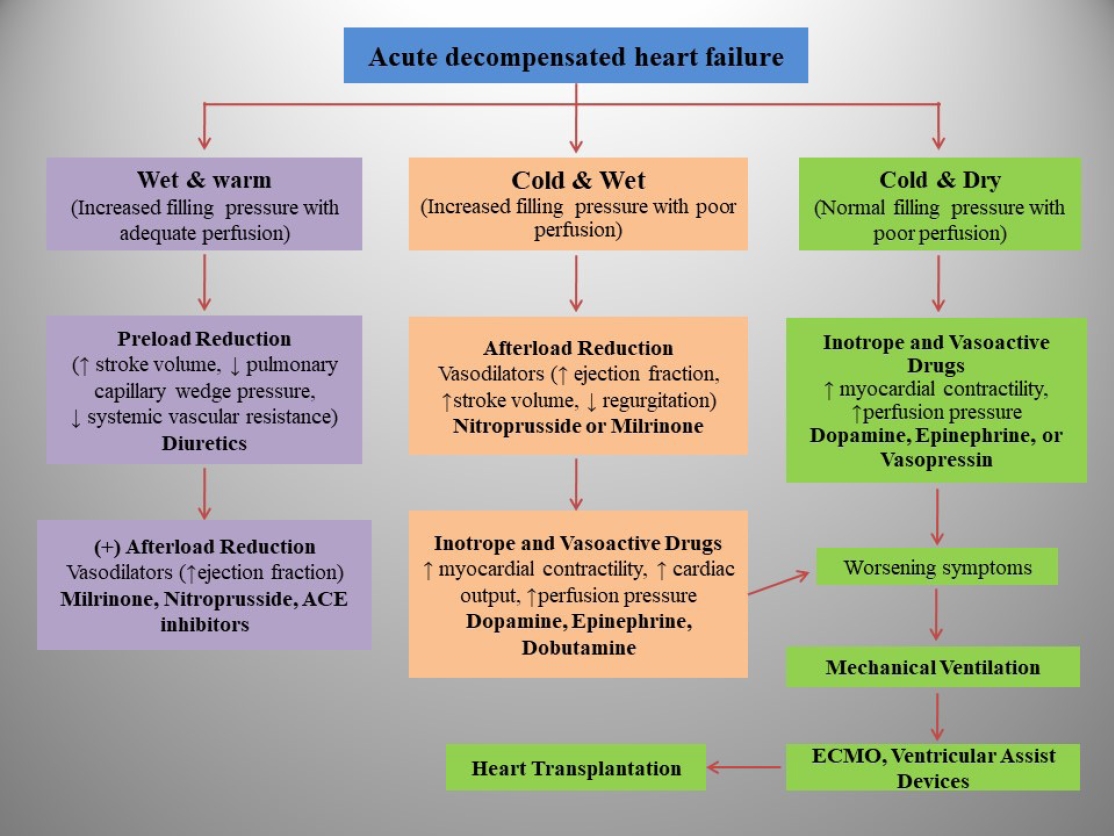
- Heart failure in children and adolescents: an update on diagnostic approaches and management
(105 times)
-
Amit Agrawal, Dalwinder Janjua, Abdulrahman Ahmed Alsayed Ali Zeyada, Ahmed Taher Elsheikh
-
Clin Exp Pediatr. 2024;67(4):178-190. Published online June 19, 2023
-
|
· Pediatric heart failure (PHF) is a clinical syndrome featuring various symptoms (shortness of breath, ankle swelling, fatigue) and signs (pulmonary crackles, peripheral edema).
· Congenital heart diseases are the most common underlying etiology of PHF, whereas myocarditis and primary cardio-myopathies are common in children without structural ab-normalities.
· PHF pathophysiology is complex and multifactorial and varies by etiology and age.
· PHF management includes decongestive therapy, treatment of underlying causes, preventing progression, and managing pulmonary or systemic obstructions.
· Drugs should be chosen based on pharmacodynamics, clinical manifestations, hemodynamic state, and renal function. |
-
-
- Review Article
- Genetics and Metabolism
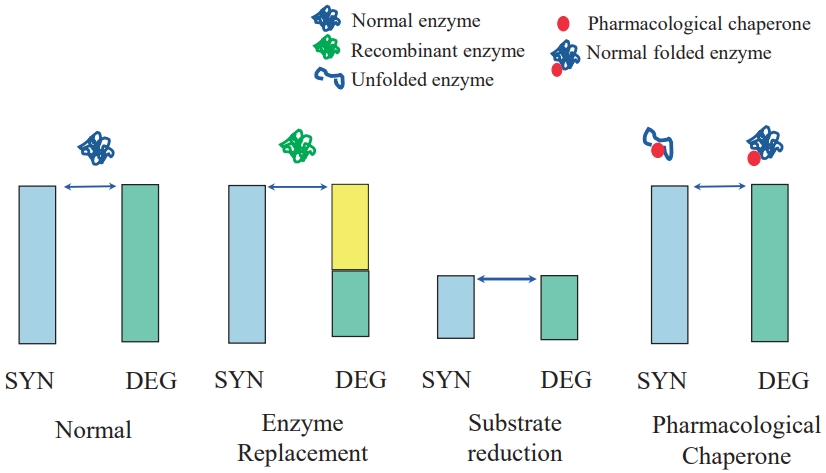
- Development of orphan drugs for rare diseases
(103 times)
-
Han-Wook Yoo
-
Clin Exp Pediatr. 2024;67(7):315-327. Published online June 28, 2023
-
|
· Orphan disease is a rare disease, primarily affecting newborn and children. Vast majority of orphan diseases has genetic background.
· Orphan disease is individually rare. But as a whole, it is not rare, becoming a great socioeconomic burden.
· The diagnosis of rare genetic disease has been problematic, but recent progress of genome analysis technologies makes it faster and more precise.
· There are many unmet needs as to the curative treatment. However, the number of treatable rare diseases is growingly increasing owing to the development of biotechnology.
· Most orphan drugs are extremely expensive because of numer ous hurdles during the process of drug development as well as small number of patients. |
-
-
- Original Article
- General Pediatrics
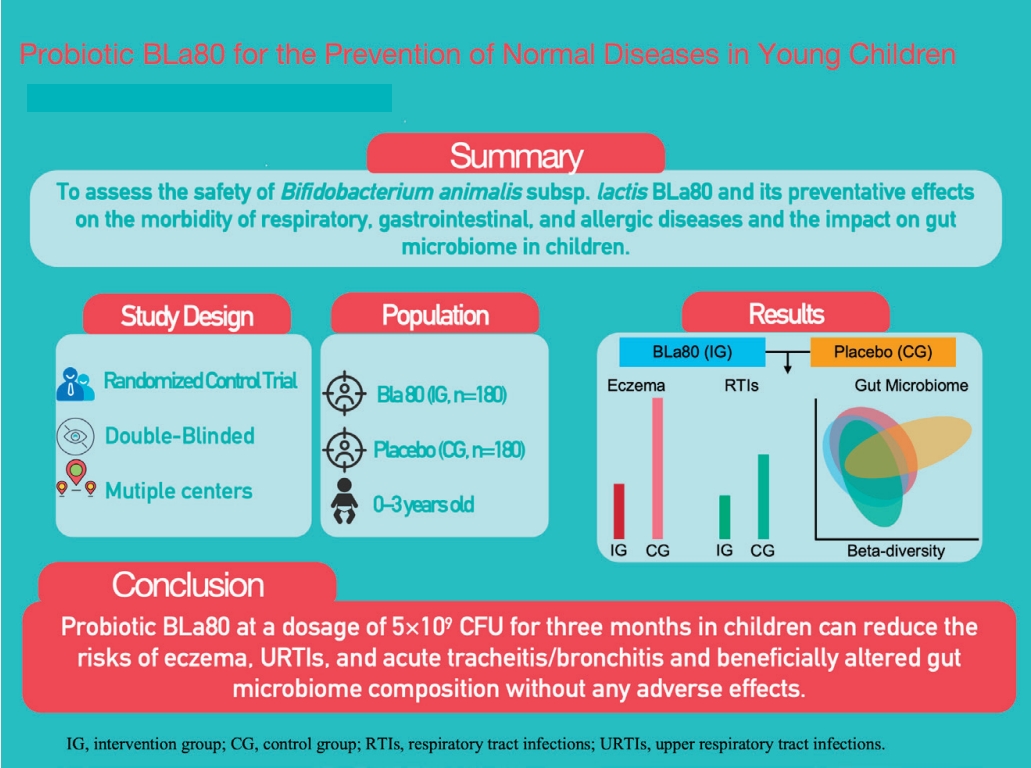
- Bifidobacterium animalis subsp. lactis BLa80 for preventing allergic, respiratory, and gastrointestinal diseases in young children in China: a randomized double-blind placebo-controlled trial
(102 times)
-
Ke Chen, Xi Zhang, Kaihong Zeng, Jiayi Zhong, Shanshan Jin, Yang Nie, Ping Yang, Nianyang He, Haixia Chen, Yanmei Cao, Yunrong Fu, Ziji Fang, Wei Jiang, Changqi Lium
-
Clin Exp Pediatr. 2026;69(2):150-162. Published online October 30, 2025
-
|
Question: Can probiotic BLa80 bring long-term benefits to the health of young children?
Finding: This trial demonstrated that the daily administration of s BLa80 at 5×109 colony-forming units for 3 months in children can reduce the risk of eczema, upper respiratory tract infections, and acute tracheitis/bronchitis as well as beneficially improve the gut microbiome without any adverse effect.
Meaning: Bla80 can bring definite health benefits to young children. |
-
-
- Review Article
- Neonatology (Perinatology)
- Demographic transition in South Korea: implications of falling birth rates
(100 times)
-
Chae Young Kim, Sung-Hoon Chung
-
Clin Exp Pediatr. 2024;67(10):498-509. Published online June 27, 2024
-

|
· Since 1960, South Korea's TFR decreased from 6.33 to 0.78 in 2022, below the 2.1 replacement level since 1983, with women's average age at first marriage rising to 31.3 in 2022.
· Policies needed: financial incentives, longer parental leave, better childcare.
· The U.S. (15.3% immigrants) and Germany (18.8%) use immigration to maintain demographic stability, a strategy South Korea is considering. |
-
-
- Allergy
- Global burden of asthma among children and adolescents with projections to 2050: a comprehensive review and forecasted modeling study
(100 times)
-
Tae Hyeon Kim, Hyunjee Kim, Jiyeon Oh, Soeun Kim, Michael Miligkos, Dong Keon Yon, Nikolaos G Papadopoulos
-
Clin Exp Pediatr. 2025;68(5):329-343. Published online April 22, 2025
-

|
Pediatric asthma can persist to adulthood and must be effectively managed. This review examined the prevalence of asthma among individuals younger than 20 years and revealed a decline from 1990 to 2021, higher rates in males, and a peak in children aged 5–9 years. Despite a projected continued decrease in prevalence by 2050, asthma will remain a significant health concern for children and adolescents. |
-
-
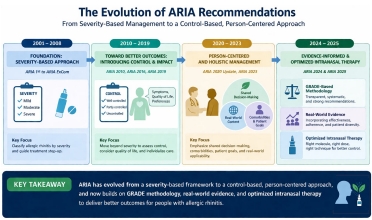
- Update on pediatric allergic rhinitis: narrative review based on guideline updates
(100 times)
-
Jung Yeon Shim
-
Clin Exp Pediatr. 2026;69(6):473-483. Published online May 28, 2026
-
|
Intranasal corticosteroids remain the cornerstone treatment for moderate to severe allergic rhinitis. The 2024–2025 Allergic Rhinitis and its Impact on Asthma guideline update suggests that fixed intranasal antihistamine–intranasal corticosteroid combinations may provide greater symptom control in allergic rhinitis than either agent alone. A control-based patient-centered approach that incorporates real-world evidence is essential for optimizing treatment outcomes in children. |
-
-
- Nephrology (Genitourinary)
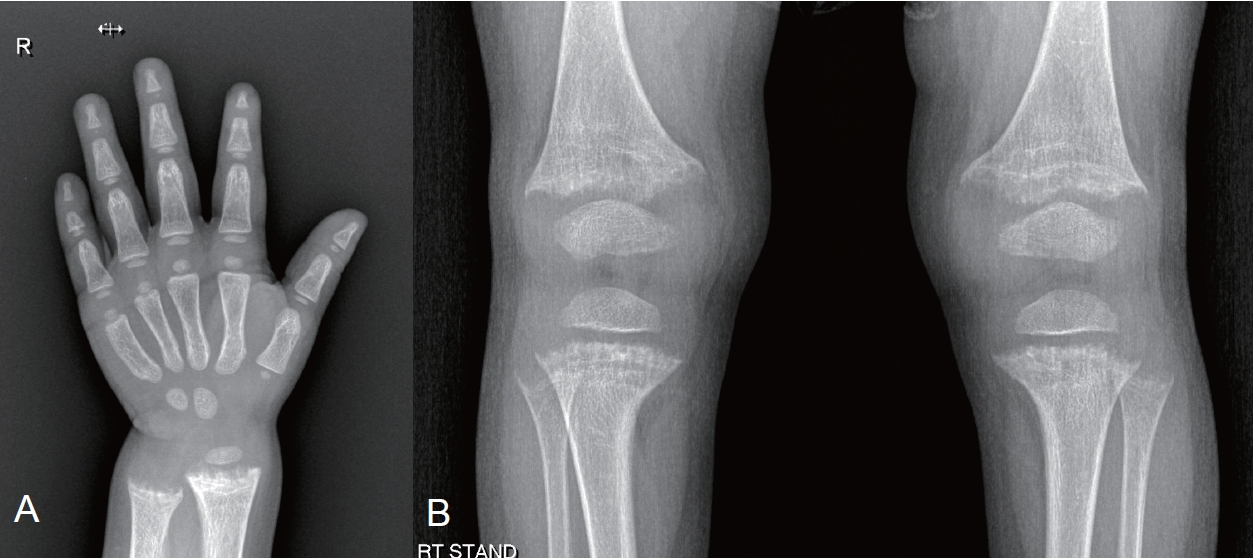
- X-linked hypophosphatemic rickets: from diagnosis to management
(94 times)
-
Eujin Park, Hee Gyung Kang
-
Clin Exp Pediatr. 2024;67(1):17-25. Published online June 14, 2023
-
|
· X-linked hypophosphatemia (XLH), the most common cause of hypophosphatemic rickets, affects 1/20,000 people.
· XLH is caused by a loss-of-function mutation of the PHEX gene.
· Its main pathogenesis is elevated fibroblast growth factor-23 (FGF23) level.
· Burosumab, an FGF23 inhibitor, was developed in the early 2000s.
· Burosumab was approved in Korea in 2020 for XLH patients aged 1+ years with radiographic evidence of bone disease. |
-
-
- Original Article
- General Pediatrics
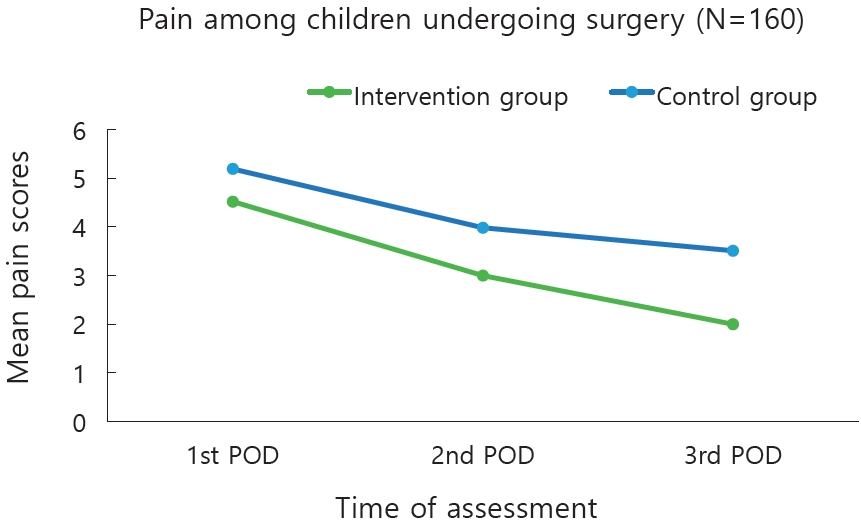
- Nonpharmacological interventions for managing postoperative pain and anxiety in children: a randomized controlled trial
(90 times)
-
Edlin Glane Mathias, Mamatha Shivananda Pai, Vijay Kumar, Dinesh Narayanakurup, Malavika Kulkarni, Vasudeva Guddattu, Ann-Cathrine Bramhagen, Baby S Nayak, Anice George
-
Clin Exp Pediatr. 2024;67(12):677-685. Published online October 31, 2024
-
|
Question: What is the effect of nonpharmacological interventions on postoperative pain and anxiety among children.
Finding: Nurse-provided distraction interventions reduce pain and anxiety among pediatric surgical patients.
Meaning: The findings suggest that nonpharmacological interventions provided postoperatively to children reduce their pain and anxiety levels. |
-
-
- Review Article
- General Pediatrics
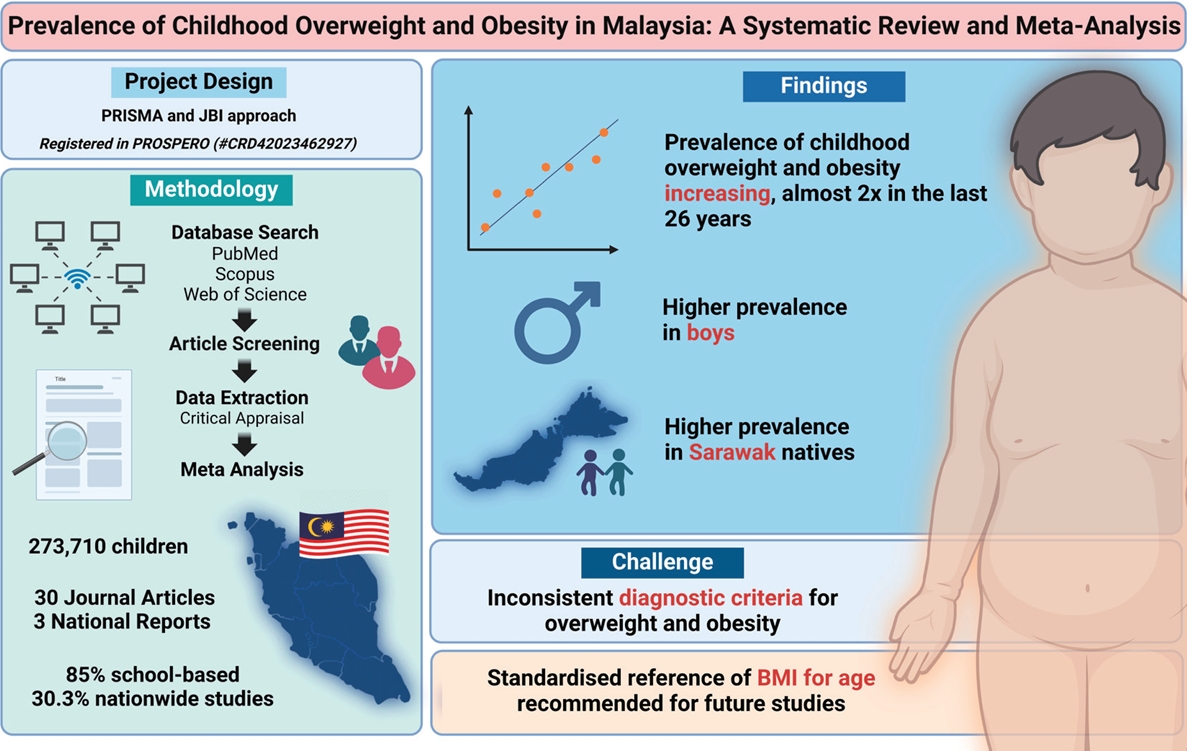
- Prevalence of childhood overweight and obesity in Malaysia: a systematic review and meta-analysis
(85 times)
-
Ker Yang Chua, Ker Yung Chua, Karuthan Chinna, Chooi Ling Lim, Maheeka Seneviwickrama
-
Clin Exp Pediatr. 2025;68(2):115-126. Published online November 13, 2024
-
|
The incidence of childhood obesity is increasing worldwide. National surveys in Malaysia have shown similar trends. This review aimed to increase our understanding of the prevalence and associated factors of childhood overweight, obesity, and excess weight in Malaysia. A systematic review and meta-analysis were conducted of studies reporting the prevalence of overweight and obesity in Malaysian children aged <18 years.... |
-
-







")



