


Introduction
It has been recognized for some time that significant cardiac arrhythmias may frequently be seen with epileptic seizure activity1). Ictal tachycardia and bradycardia are common arrhythmias, but ictal sinus pause and asystole are rare and more severe. Recently, ictal arrhythmia has become a notable warning sign of sudden unexpected death in epilepsy (SUDEP), which accounts for 15% of all epilepsy-related deaths2). Here, we present an interesting case of a child with ictal sinus pause and asystole.
Case report
A 27-month-old girl was hospitalized due to 5 episodes of convulsions during the past 2 days. The episodes were generalized, febrile or afebrile, and lasted for 30 seconds to 1 minute. In the interictal phase, her mental state was alert, without neurologic deficit. She exhibited symptoms of mild cough, sputum, and rhinorrhea. She did not vomit, and had no sign of meningeal irritation on neurologic examination. She had no specific problems in the perinatal period, but she had a history of simple febrile convulsion at 16 months of age. She appeared to be developing proper motor and language skills, without any known disease.
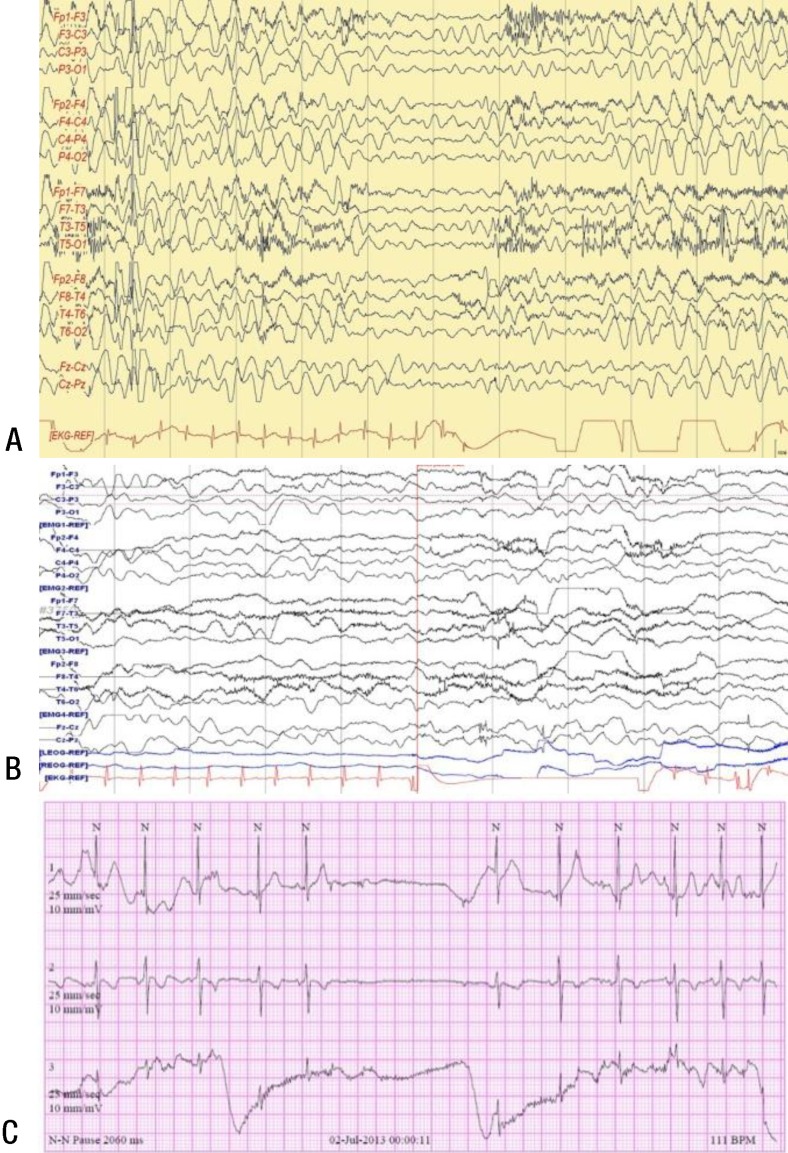
All investigations, including blood counts, electrolyte levels, glucose level, chest radiography, echocardiography (ECG), and brain magnetic resonance imaging (MRI), were normal. Routine sleep electroencephalography (EEG) was normal, but she experienced 1 generalized tonic seizure, lasting for 1 minute, every day for 3 days. During 24-hour video-monitored EEG, she showed frequent myoclonic seizures and generalized polyspike discharges with myoclonus followed by sinus pause for >4 seconds (asystole) starting about 5 seconds after myoclonus onset (Fig. 1A). One time of sinus pause was noted, which was not accompanied by myoclonus (Fig. 1B). Twenty-four-hour Holter ECG monitoring during the frequent seizure episodes revealed sinus arrhythmia and sinus pauses lasting for 2 to 3 seconds (Fig. 1C).
The next day, she was initially given valproic acid 20 mg/kg/day. After antiepileptic treatment, she experienced no myoclonus or generalized tonic seizures. Repeat EEG revealed no epileptiform discharges. However, 5 days later, she voluntarily stopped taking the anticonvulsant due to a rash on her trunk and back. Seven weeks later, she experienced a generalized tonic febrile seizure that lasted for 15 seconds. Video-monitored EEG revealed an occasional high-voltage generalized spike and wave or polyspike discharges. Twenty-four-hour Holter ECG monitoring revealed a sinus block for 1 second, which was not accompanied by clinical seizure. After the valproic acid was restarted, she did not experience any more seizures.
In the following 6 months, EEG and 24-hour Holter ECG monitoring were normal. At 36 months of age, she experienced a generalized tonic febrile seizure and myoclonus. At that time, we did not perform EEG or 24-hour Holter ECG monitoring. Results of an SCN1A gene study were normal. At 44 months of age, she maintained the antiepileptic medication and had no seizures, ictal arrhythmias, or developmental delays.
Discussion
Our patient experienced frequent myoclonic seizures accompanied by sinus pause lasting for 2 to 3 seconds, resulting in asystole. Accidentally an interictal sinus pause was found on the video-monitoring not accompanying by clinical sign. After antiepileptic treatment, there were not any ictal events, interictal epileptiform discharges nor sinus pause on the repeat 24-hour video-monitored EEG and 24-hour Holter ECG.
Seizure-related cardiac arrhythmias are frequently reported in adult: Asystole, tachycardia, bradycardia, atrioventricular conduction block, atrial flutter/fibrillation, and ventricular fibrillation. Ictal tachycardia is frequently reported and may occur in up to 80% of seizures. Sinus pause, asystole and arrest are relatively rare and can be fatal3,4). But there is only rare information about cardiac changes during seizures in children.
Asystole was defined as an relative risk interval of >3 seconds or >4 seconds in several reports4). In a recent retrospective study by van der Lende et al.4) mean prevalence of ictal asystole in all people with refractory focal epilepsy admitted for a video-monitored EEG recording was 0.318%. In a study from Rocamora et al.5) 5 out of 1,244 patients (0.4%) had 11 asystole events. Ictal asystole clinically often presented syncope, cyanosis, loss of consciousness, and subsequent falls.
Especially in children, reports of ictal asystole were rarely reported. Until recently, ictal asystole was recorded in about 5 pediatric patents5,6). Three of the 5 patients with ictal asystole had temporal lobe epilepsy, 2 had extratemporal lobe epilepsy, and none had generalized epilepsy. Unlike previous reports about ictal asystole in focal epilepsy, this is the first case of a child with myoclonus seizure and asystole recorded on a video EEG and ECG.
One recent prospective study reported that ictal apnea and bradycardia occurred more often in children than in adults, whereas ictal tachycardia occurred more often in adults than in children1). In another study, ictal apnea and bradycardia were seen in younger boys with lesions on brain MRI, whereas ictal tachypnea and tachycardia were seen in older children and in those without lesions on brain MRI7). However, only a few cases were reported.
Cardiac arrhythmias have been suggested to play a prominent role in the pathogenesis of SUDEP in many studies, though the relationship is still unclear7,8). SUDEP accounts for as much as 15% to 17% of all epilepsy-related deaths3,9). Sinus pauses and bradycardia mediated by vagal cardiac activation may proceed to cardiac asystole10,11). In addition to cardiac arrhythmias, hypoventilation and hypoxia, central apnea, and cerebral shutdown around seizures can contribute to sudden unexpected death12). Our patient presented with frequent sinus pauses and did progress to cardiac asystole, but not to SUDEP.
According to van der Lende et al.4) ictal asystole was considered to self-limiting arrhythmia. But there was one severe case of ictal bradycardia and asystole in infant, where the death could not be evitable despite anticonvulsant therapy and pacemaker implantation. In newly diagnosed patients with epilepsy, antiepileptic drug (AED) is recommended13). Cardiac pace maker implantation should be considered in patients with refractory epilepsy or recurrence of asystole episodes. However, a pacemaker implantation was debated due to possibility of adverse events such as infection and unclear effectiveness on mortality rate. Our patient presented with ictal sinus pauses and asystole. We quickly started AED therapy and her prognosis was good. It is important to be alert to the occurrence of ictal arrhythmia and SUDEP and use a low threshold in cardiac monitoring and investigations. It seems reasonable to assume that the best way to identify the risk factors for SUDEP, especially occurring in young age and maintain a therapeutic antiepileptic AED level9).
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


