

Adolescence is the transitional period from infancy to adulthood, in which a person experiences rapid physical growth, along with mental and social growth and development. During the early period of adolescence, the ability for abstract thinking, distinguished from concrete thinking, begins to increase gradually when solving problems or making decisions. In the middle stage of adolescence, the person reaches the peak of puberty, beginning to keep a distance from parents and trying to be independent in order to attain autonomy; friends play a central role in this process. Once the late period of adolescence is reached, abilities in abstract thinking develop fully, and as a result, the person thinks about his/her future roles and plans.
While undergoing these processes, adolescents achieve physical, mental, and social growth, and along with physical changes, experience rapid sociocultural changes. Over the course of adolescence, individuals establish their value systems and secure a social status associated with being an adult.
Most people experience these processes and changes without much trouble; however, some fail to adjust to a rapidly changing social life and associate with friends, becoming easily exposed to cigarettes or alcohol. This can potentially lead to drug addiction or other delinquencies.
Introduction
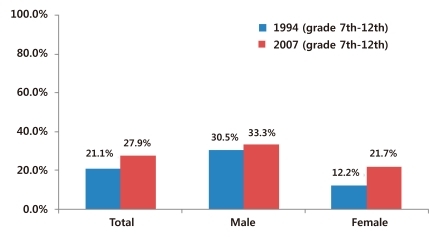
With the recent opening and westernization of our society, smoking in adolescents has increased and has become more common. Many adolescents start smoking at a young age, out of curiosity and a spirit of adventure, only to become addicted to it. Nevertheless, it is not easy to grasp trends in adolescent smoking in Korea because few systematic surveys and studies have been performed. According to surveys in 1994 and 20071,2), the overall smoking rate of adolescents in Korea changed from 21.2 to 27.9%. By gender, the rate increased from 30.5 to 33.3% in males, and from 12.2 to 21.7% in females (Fig. 1). Although the overall increase was not large, the smoking rate among female adolescents showed a relatively large increase.
Habitual smoking by adolescents can be a gateway to other types of drug abuse and can cause various health problems, including frequent upper respiratory infections, delayed lung development, decreased maximum vital capacity, and lung cancer. Thus, we should pay attention to the prevention of adolescent smoking, not only for public health but also from an economic perspective, and various efforts made should include intensified anti-smoking education in schools, prohibiting the sale of cigarettes to minors in the community, and a rise in cigarette tax and price3).
The smoking experience of adolescents
Approximately 90% of the people who smoke for the first time are adolescents younger than 18, and the rate of smoking in adolescents is rising steadily. In general, adolescents start smoking out of curiosity, and many become habitual smokers during this period. Factors related to habitual smoking include the perception of cigarettes, a combined use of alcohol and drugs, intrafamilial linkage, and smoking by friends and parents. In particular, along with alcohol, smoking is known to be a gateway to other types of drug abuse. For these reasons, it is crucial to prevent early smoking4,5).
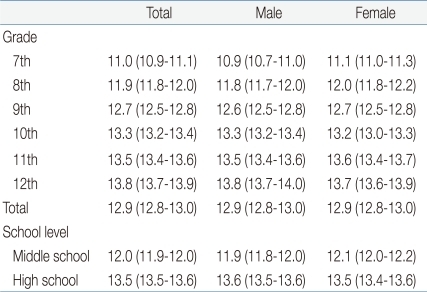
In 1976, Kandel et al.6) surveyed high school students in New York State and reported that 72.0% of these had experience of cigarette smoking. Moreover, according to a survey by Kokkevi and Stefanis7) in 1981, 70.2% of high school students in Greece had tried cigarette smoking, and 22.3% were habitual smokers. Bachman et al.8) reported that the smoking rate of American high school students had reached a peak in 1976 and 1977 and had been decreasing steadily since then. According to Baugh et al.9), 52.3% of American adolescents between the age of 8 and 17 had tried smoking, with 50.1% of that group trying it for the first time at an age younger than 12; in each age group, males experienced smoking earlier than females. The smoking rate of American 12th grade students decreased from 63.1 in 1992 to 57.2% in 2002. According to a survey on male and female adolescents by the Center for Disease Control and Prevention in 2007, 33.3% and 21.7%, respectively, had tried smoking, and students in higher grades showed a significantly higher smoking rate. Most smoking adolescents had smoked for the first time at the age of 12 or 13, and they usually smoked while associating with their friends (Table 1). Thus, peer relations and the surrounding environment are considered important factors of the smoking experience.
Among environmental factors, indiscrete salesmanship riding on the materialism of society is considered to play a role. For example, an increasing number of entertaining facilities instigating deviations and easy purchasability of cigarettes are believed to stimulate smoking in adolescents.
Risk factors that increase the smoking rate among adolescents
1. Family history
The frequency of adolescent smoking increases when there are many smokers in the family. Parents are particularly important because they are the adolescents' primary role models. The attitudes of parents toward smoking, their perception of smoking, and affection between parents and their children are all crucial factors that affect adolescent smoking. Frequent disagreements with parents, divorce between parents, abuse by family members, incest, immature parents, and poor intrafamilial linkage all contribute to the risk of adolescent smoking.
2. Companionship
If the frequency of smoking is high among friends or family members of a similar age, an individual is more likely to follow the same course. The risk is particularly high when a student is transferred from one school to another or joins a new circle of friends. The risk of long-term smoking increases when an adolescent can easily access cigarettes or has been exposed to cigarettes at a young age.
3. Personal characteristics and psychopathological problems
Each adolescent has a different value system, attitude, surrounding environment, and personal literacy (toward study and society). Children who are antisocial, rebellious, isolated from school and society, or show poor family relationships or academic performance are highly likely to begin smoking. Some adolescents try to overcome depression or fear through smoking. In addition, the rate of smoking is higher in men than in women.
4. Psychosocial problems
While it has decreased in recent years, offering someone a cigarette has been regarded as etiquette in Korean society, and adolescents may learn this custom. Additionally, young adolescents may smoke, thinking that smoking can make them appear more mature and adult-like. Female students have recently begun smoking more frequently than before out of resistance to gender-based discrimination. In addition, adolescents sometimes start smoking as a way to emulate television or mass media celebrities and sports stars.
The impacts of smoking on the health of infants and adolescents
The neonates of smoking parents suffer chronic hypoxia from the fetal stage, which causes growth and developmental disorders, resulting in low birth weight, small height, small head and bust circumference, and delayed development of the shoulders. In addition, miscarriage and premature birth occur more frequently. Neonates and infants who are exposed to passive smoking, as a result of parental smoking, have an increased incidence of serious respiratory diseases, such as bronchitis and pneumonia. According to a survey, the risk of hospitalization for respiratory diseases, particularly asthma and stridor, is over 28% higher in infants with smoking mothers than in those with non-smoking mothers. Another survey reported that medical problems, such as asthma, chronic otitis media, and sudden infant death, were more common in children of smokers than in those of non-smokers.
Adolescent smoking causes dysfunction of the peripheral airway. One study found that the forced expiratory volume in a second (FEV1) of smoking adolescents decreased significantly; specifically, their forced vital capacity (FVC) was approximately only a half that of non-smoking adolescents. According to a report by Berlin-Breman, the ratio of FEV1/FVC decreased with an increasing concentration of carbon monoxide on expiration, a method of checking smoking, in adolescent smokers. In addition, the study found that high-density lipoprotein-cholesterol decreased in adolescents who had been smoking for less than 2 years.
Smoking is known to damage pulmonary functions through changing the airway and pulmonary parenchyma, which increases the risk of respiratory and systemic infection, as a result of structural changes and immunological responses of the respiratory system. Smoking generates various substances that cause bronchial inflammation, fibrosis, and the increased permeability of airway mucous membrane; these substances also decrease the mucociliary clearance of airway mucous membrane, making it difficult to remove pathogens, thereby leading to infection. Smoking also affects respiratory immunity by decreasing blood immunoglobulin, weakening antigen-antibody reactions, inhibiting cytokine secretion by weakening the function of phagocytes, and decreasing the count of CD4+ lymphocytes. As a result, smoking increases bacterial infection and viral infection in the respiratory system.
Overall, these reports suggest that adolescents who smoke may be exposed to various smoking-related diseases within a few years of starting smoking.
Problems and psychosocial aspects of adolescent smoking
Naturally, the younger a person begins smoking, the longer the period and the larger the quantity of smoking. In particular, people who start smoking younger than the age of 15 are 4 times more likely to develop lung cancer than those who start at the age of 25 or later.
In the U.S., the rate of new smokers is around 3,000 a day or 1 million a year, and 80% of these are children or adolescents10). The American Academy of Pediatrics11) recently classified cigarettes as one of the most addictive drugs and argued for strict inhibition of smoking by including smoking in the category of infant diseases. Considering the impact of smoking on the body, it is important to establish active preventive measures against exposure to harmful cigarettes in growing adolescents.
Lee et al.1) reported that male students tried smoking earlier than female students, and the smoking rate was higher among older students. In 2002, the Department of Pediatrics at the Medical School of Korea University12) indicated that the smoking rate among adolescents was higher in older students, academic underachievers, those from low-income families, and those living apart from their parents. Further, it was significantly related to the academic qualification of the mother, with a greater frequency (36.5%) among students with less educated mothers. It is of interest that a mother's educational background is correlated with the likelihood that her child will smoke, since mothers in Korea are more involved in the children's life than the fathers. It seems likely that the mother's educational level is interconnected to the education and occupation of her spouse, and mothers of lower socioeconomic standing, who are more likely to take part in economic activities to maintain family finances, have less time to take care of the children. According to Kim13), smoking is the most important predictor of adolescent delinquency and criminal behavior, which is supported by the fact that the smoking rate is only 15.3% among average adolescents but 96.3% in delinquent adolescents. This demonstrates that smoking is the first gateway to juvenile delinquency.
Discussion
Adolescents usually start smoking not out of physiological need but out of a desire for social self-growth, to be treated as an adult in society, or out of resistance to established regulations14). In anti-smoking education for adolescents, rather than simply forcing the social norm that adolescents should not smoke, it is better to fully explain the harmful effects of smoking on physical growth and mental soundness. Additionally, by convincing adolescents that cigarette abuse causes social problems and can become a gateway to the use of other drugs, they may establish specific norms at their own discretion and not become addicted to cigarettes and the consequent moral corruption and various delinquencies.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


