

Introduction
Among many public health indexes, neonatal mortality rate (NMR) and infant mortality rate (IMR) are the two most important measures indicating the regional, national, and population status in various fields including health, demography, society, economy, biology, and culture. NMR and IMR are therefore very important indexes of a country's state and trends of health or development, and is a component of the physical quality of life index. A decrease in NMR and IMR results in the improvement of infant mortality and survival, which can positively influence the national public state of health.
In Korea, during the past 60 years there has been marked improvement in the management of maternity, pregnancy, delivery, birth, neonatal and infantile health care by a qualitative improvement in obstetric, perinatal, neonatal, and pediatric medical conditions. As a result, despite increasing trends of high-risk newborns including prematurity, neonatal survival rates are improving with the development of neonatal intensive care medicine. In addition, the development of infantile preventive medicine and treatment of infants had a big effect on the improvement of NMR and IMR in Korea, and has become a cornerstone in the development of national health.
Every year since 1993, there is an official announcement about IMR. There is a need for systematic review analysis on the recent changes and trends of NMR and IMR over the past 60 years in Korea, which makes it important to review the differences in the causes of neonatal and infantile death and understand the current state. Therefore, in this review, we attempted to analyze the changes and trends of NMR and IMR in Korea by understanding the current state of improved public health and we also analyzed changes in the causes of death accompanying improved NMR and IMR. We also attempted to provide basic data for neonatal and infantile health promotion.
Definitions
The following terms based on International Statistical Classification of Diseases (ICD) and Related Health Problems 10th revision of World Health Organization (WHO)1,2).
Neonate: infants 0 to 27 days of life, under 28 days of life.
Early neonate: infants 0 to 6 days (under 7 days) of age.
Late neonate: infants 7 to 27 days (under 28 days) of age.
Neonatal mortality rate: [annual number of death of infants 0 to 27 days of life / the annual number of live births] × 1,000.
Early neonatal mortality rate: [annual number of death of infants 0 to 6 days of age / the annual number of live births] × 1,000.
Late neonatal mortality rate: [annual number of death of infants 7 to 27 days of age / the annual number of live births] ×1,000.
Infant mortality rate: [annual number of death of infants under 1 year / the annual number of live births] × 1,000.
Data collection
1. NMR and IMR in Korea
From 1993 the official IMR of investigation by Korea Ministry of Health and Welfare (KMHW)3) has been published on a national scale. KMHW has enlisted the services of the Korea Institute for Health and Social Affairs (KIHASA) since 1993 and have been publishing data on Korean NMR and IMR4-7). These data are reported to the United Nations, WHO, Organization for Economic Cooperation and Development (OECD) and are used as reference guides on Korean statistics. A large amount of personal data has accumulated prior to 19938). Therefore, we used data by KHMW from 1993 and used data by Statistics Korea from 2007. We also used data by Chang et al.8) because they conducted organized analyses on Korean NMR and IMR in 2011.
2. Causes of neonatal and infant death in Korea
We classified the causes of neonatal and infant death in Korea from 1983 to 2009 into three categories by chapters and block categories based on the Korean Standard Classification of Diseases (KCD) (5th edition), classified by the Korean Medical Record Association based on the ICD and related health problems (10th edition) by WHO1,2). We used data on the cause of death based on Statistics Korea9) from 1983 to 2009, and data on the ten major causes of neonatal and infant death based on KIHASA from 1996 to 200810).
Changes in the NMR and IMR in Korea
1. Changes of NMR in Korea (1993 to 2009)
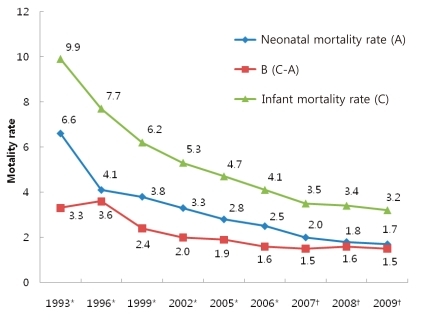
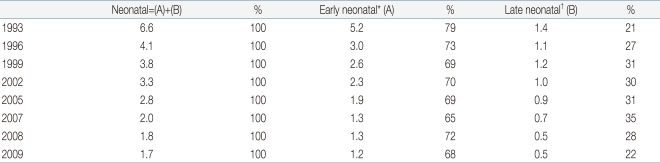
Overall, Korean NMR shows a decline: 6.6 in 1993, 4.1 in 1996, 3.8 in 1999, 3.3 in 2002, 2.8 in 2005, 2.5 in 2006, 2.0 in 2007, 1.8 in 2008 and 1.7 in 2009 (Fig. 1). The change of early and late NMR is shown in Table 1, and also shows a decline. The proportion of early NMR is 79% in 1993, 69% in 1999, 70% in 2002, 69% in 2005, 68% in 2009, exhibiting a reducing trend. However, early NMR contributes to more than two-thirds the proportion of large numbers in NMR (Table 1).
2. Changes of IMR in Korea
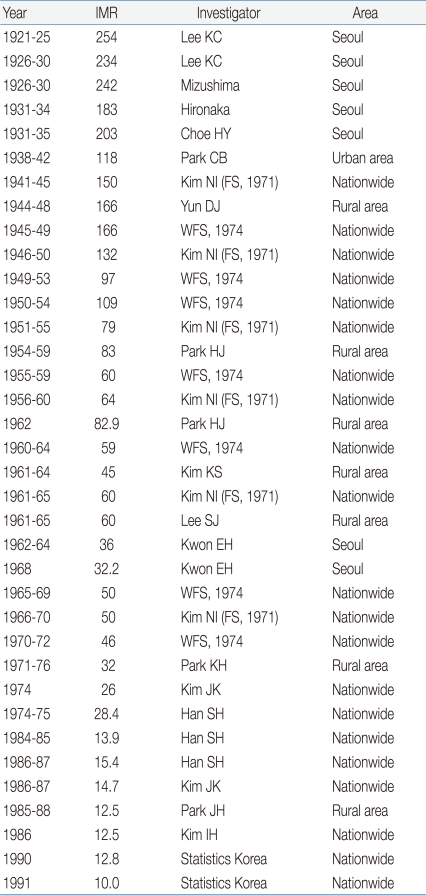
1) IMR before 1993
Korean research on IMR targeted regional or nationwide data before 1993. Chang et al.8) summarized data as follows in Table 2. We can recognize slowly reducing trends of IMR; 350 before 1920, 240 to 250 in the 1920s, 180 to 200 in the 1930s, 160 in the 1940s, 150 in the early 1940s, 160 in the late 1940s, 100 during the Korean War, 60 in the early 1960s, 50 in the late 1960s, 30 to 40 in the 1970s, and 15 in the late 1980s8).
3) Proportion of NMR of IMR
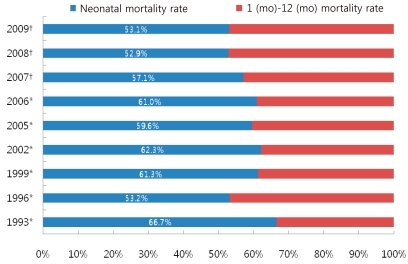
The ratio of NMR in IMR is shown in Fig. 2. The ratio has been decreasing slowly: 66.7% in 1993, 53.2% in 1996, 61.3% in 1999, 62.3% in 2002, 59.6% in 2005, 61.0% in 2006, 57.1% in 2007, 52.9% in 2008, and 53.1% in 2009. According to this data, the NMR still consists of approximately half the IMR, implicating the reduction in NMR could be one of the most important factors of improving IMR in Korea8).
Changes in causes of neonatal and infant death in Korea
1. Causes of neonatal death (2005, 2009)
1) Classified by chapters of KCD: causes and numbers of neonatal death9)
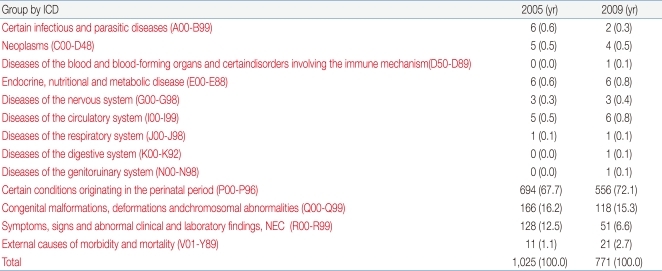
The numbers of neonatal deaths decreased from 1025 in 2005 to 771 in 2009. The causes and number of neonatal deaths in Korea in 2005 and 2009 by KCD are shown in Table 3. Certain conditions originating in the perinatal period (P00-P96) in 2005 (67.7%) and 2009 (72.1%) were the highest, followed by congenital malformations, deformations and chromosomal abnormality (Q00-Q99) in 2005 (16.2%) and 2009 (15.3%), and symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (NEC) (R00-R99) in 2005 (12.5%) and 2009 (6.6%). Certain conditions originating in the perinatal period and congenital malformations, deformations and chromosomal abnormalities are important causes, which means diseases in perinatal period and soon after of birth are the most frequent.
2) Classified by block categories of KCD: causes and numbers of neonatal death9)
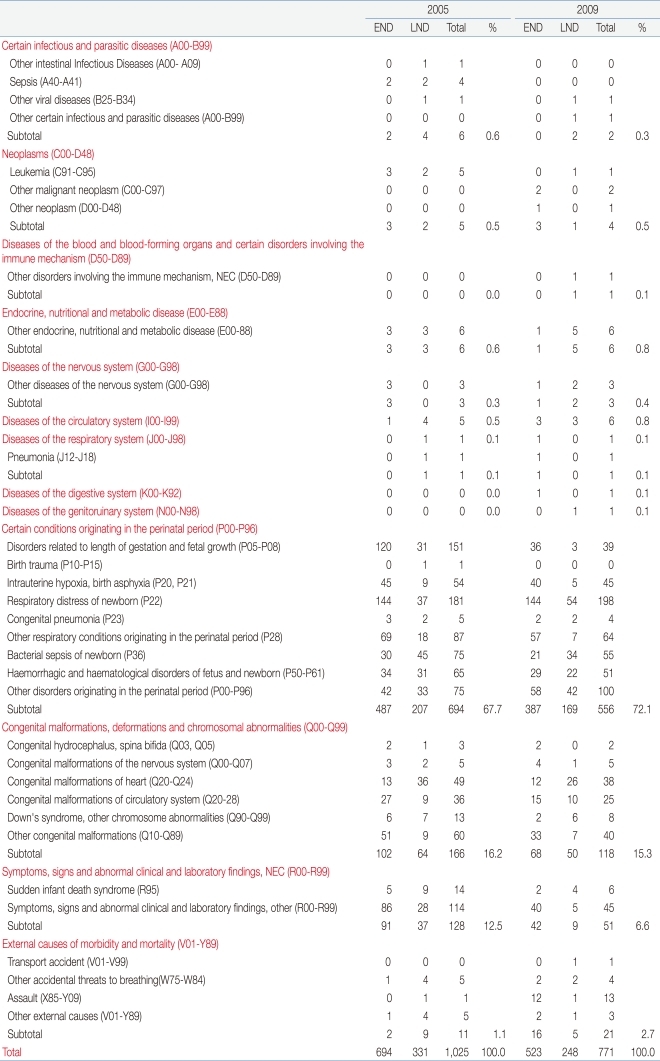
The block categories of KCD are shown in Table 4. In 2005, the following conditions originated in the perinatal period (P00-P96) in order of frequency, respiratory distress of newborns (P22), disorders related to length of gestation and fetal growth (P05-P08), other respiratory conditions originating in the perinatal period (P28), bacterial sepsis of newborns (P36), other disorders originating in the perinatal period (P00-P96), haemorrhagic and haematological disorders of fetuses and newborns (P50-P61), intrauterine hypoxia, birth asphyxia (P20, P21), congenital pneumonia (P23), and birth trauma (P10-P15). With regards to congenital malformations, the following conditions were observed in order of frequency: deformations and chromosomal abnormalities (Q00-Q99), other congenital malformations (Q10-Q89), congenital malformations of the heart (Q20-Q24), congenital malformations of the circulatory system (Q20-28), Down's syndrome, other chromosome abnormalities (Q90-Q99), congenital malformations of the nervous system (Q00-Q07), congenital hydrocephalus, and spina bifida (Q03, Q05).
With regards to symptoms, signs and abnormal clinical and laboratory findings, NEC (R00-R99), they are symptoms, signs and abnormal clinical and laboratory findings, other (R00-R99), sudden infant death syndrome (R95). Neonatal death according to early and late neonatal periods is shown in Table 4. The number of deaths decreased to 694 in the early neonatal period in 2005, and 523 in the late neonatal period. The ratio of deaths in the early neonatal period to total death was 69% in 2005 and 68% in 2009.
3) Changes in the ten major causes of neonatal death (1996 to 2008)10)
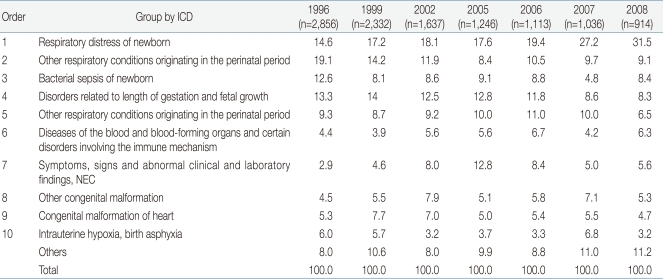
Changes in the ten major causes of neonatal death in 1996, 1999, 2002, 2005, 2006, 2007, and 2008 in Korea by Choi's study10) of KIHASA are shown in Table 5. The respiratory distress of newborns, diseases of the blood and blood-forming organs as well as certain disorders involving the immune mechanism, symptoms, signs and abnormal clinical and laboratory findings, NEC, Other congenital malformation, and others increased in ratio. In contrast, other respiratory conditions originating in the perinatal period, bacterial sepsis of newborns, disorders related to length of gestation and fetal growth, other respiratory conditions originating in the perinatal period, congenital malformation of heart, intrauterine hypoxia, birth asphyxia were decreased in trend
2. Causes of infant death (1983 to 2009)
1) Classified by chapters of KCD: causes and numbers of infant death9)
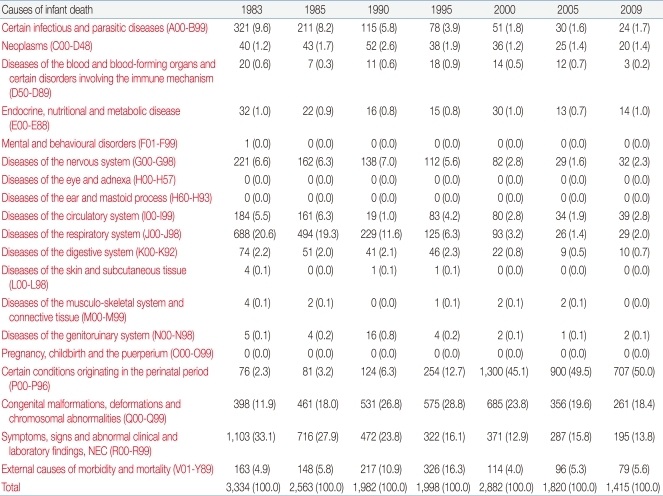
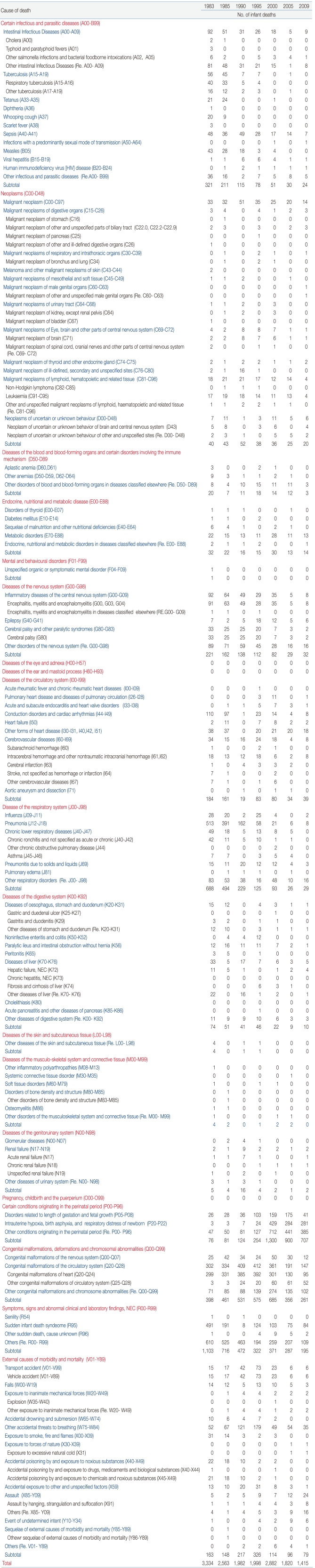
The causes and numbers of infant death by the classification of chapters of KCD in Korea from 1983 to 2009 are shown in Table 6. In order of frequency in 1983, they included symptoms, signs and abnormal clinical and laboratory findings, NEC (R00-R99) 33.1%, diseases of the respiratory system (J00-J98) 20.6%, congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) 11.9%, certain infectious and parasitic diseases (A00-B99) 9.6%, diseases of the nervous system (G00-G98) 6.6%, diseases of the circulatory system (I00-I99) 5.5%, external causes of morbidity and mortality (V01-Y89) 4.9%, certain conditions originating in the perinatal period (P00-P96) 2.3%, diseases of the digestive system (K00-K92) 2.2%, neoplasms (C00-D48) 1.2%, endocrine, nutritional and metabolic diseases (E00-E88) 1.0%, diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50-D89) 0.6%, diseases of the genito-urinary system (N00-N98) 0.1%, diseases of the skin and subcutaneous tissue (L00-L98) 0.1% and diseases of the musculoskeletal system and connective tissue (M00-M99) 0.1%. On the other hand, in order of frequency in 2009, the causes included certain conditions originating in the perinatal period (P00-P96) 50.0%, congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) 18.4%, symptoms, signs and abnormal clinical and laboratory findings, NEC (R00-R99) 13.8%, external causes of morbidity and mortality (V01-Y89) 5.6%, diseases of the circulatory system (I00-I99) 2.8%, diseases of the nervous system (G00-G98) 2.3%, diseases of the respiratory system (J00-J98) 2.0%, certain infectious and parasitic diseases (A00-B99) 1.7%, neoplasms (C00-D48) 1.4%, endocrine, nutritional and metabolic diseases (E00-E88) 1.0%, diseases of the digestive system (K00-K92) 0.7%, diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50-D89) 0.2% and diseases of the genito-urinary system (N00-N98) 0.1%.
2) Classified by block categories of KCD: causes and numbers of infant death9)
The causes and numbers of infant death classified by block categories of KCD are shown in Table 7. In order of frequency, they are symptoms, signs and abnormal clinical and laboratory findings, NEC (R00-R99) 33.1%, diseases of the respiratory system (J00-J98) 20.6%, congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) 11.9%, certain infectious and parasitic diseases (A00-B99) 9.6%, diseases of the nervous system (G00-G98) 6.6%, diseases of the circulatory system (I00-I99) 5.5%, external causes of morbidity and mortality (V01-Y89) 4.9%, certain conditions originating in the perinatal period (P00-P96) 2.3%, diseases of the digestive system (K00-K92) 2.2%, neoplasms (C00-D48) 1.2%, and endocrine, nutritional and metabolic diseases (E00-E88) 1.0%. On the other hand, a change was observed in 2009. In order of frequency, the causes were conditions originating in the perinatal period (P00-P96) 50.0%, congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) 18.4%, symptoms, signs and abnormal clinical and laboratory findings, NEC (R00-R99) 13.8%, external causes of morbidity and mortality (V01-Y89) 5.6%, diseases of the circulatory system (I00-I99) 2.8%, diseases of the nervous system (G00-G98) 2.3%, diseases of the respiratory system (J00-J98) 2.0%, certain infectious and parasitic diseases (A00-B99) 1.7%, neoplasms (C00-D48) 1.4%, endocrine, nutritional and metabolic diseases (E00-E88) 1.0%, and diseases of the digestive system (K00-K92) 1.0%.
3) Changes in the ten major causes of infant death (1996-2008)10)
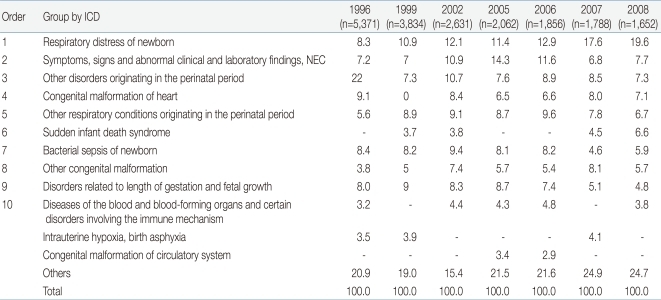
The changes in the ten major causes of infant death in 1996, 1999, 2002, 2005, 2006, 2007, and 2008 in Korea by Choi's study10) of KIHASA are shown in Table 8. Common causes of infantile death in 2008 had decreased compared with those in 1996 such as other disorders originating in the perinatal period, congenital malformation of the heart, bacterial sepsis of newborns, disorders related to length of gestation and fetal growth, intra-uterine hypoxia, birth asphyxia. However, some other causes are on the increase, such as respiratory distress of newborn, symptoms, other respiratory conditions originating in the perinatal period, other congenital malformation, diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism.
Discussion
The NMR of Korea decreased from 6.6 in 1993 to 4.1 in 1996, 3.8 in 1999, 3.3 in 2002, 2.8 in 2005, 2.5 in 2006, 2.0 in 2007, 1.8 in 2008 and 1.7 in 2009, showing a remarkably decreasing trend. Despite the recent high risk of neonatal morbidity due to increasing premature birth rates, the remarkable advances in NMR were partly influenced by highly advanced neonatal intensive care technique during the last 30 years11). In addition, the reduced perinatal mortality rate during the last 20 years (6.0 in 1996, 5.2 in 1999, 4.6 in 2002, 4.2 in 2005, 3.6 in 2006, 3.7 in 2007, 3.6 in 2008, and 3.4 in 2009) influenced the lowered NMR as well12). With decreasing NMR, the proportion of early NMR was 79% in 1993 and 68% in 2009, but the proportion was still over two-thirds the entire NMR, emphasizing the importance of early period neonatal management.
In addition, IMR has shown a decreasing pattern (9.9 in 1993, 7.7 in 1996, 6.2 in 1999, 5.3 in 2002, 4.7 in 2005, 4.1 in 2006, 3.5 in 207, 3.4 in 2008 and 3.2 in 2009). In comparison with Korea, Japan and USA, the IMR of Japan and USA were 4.6 and 9.0 in 1990, 3.1 and 8.0 in 2000, 2.8 and 6.4 in 2005, and 2.8 and 6.3 in 2009, respectively, which means the IMR of Korea is higher than that of Japan but lower than that of USA. Japan has the lowest IMR in the world, which allows us to speculate on the reason why it is lower than Korea. Reasons include operating perinatal health care centers and localization of neonatal care networks which are not yet established in Korea. On the other hand, the IMR of USA is higher than that of Korea, most likely because of different ethnicities in USA, difficulty accessing medical services, increased high risk pregnancy such as teenage or old age pregnancy, multiple gestation, and increased preterm birth8).
When we compare Korean IMR with other OECD nations, the IMR of Korea and the mean of OECD are as follows: 7.7 and 8.1 in 1996, 6.2 and 7.1 in 1999, 5.3 and 6.5 in 2002, 4.1 and 4.9 in 2006 and 3.4 and 4.7 in 2008 showing the encouraging fact that Korea has a lower IMR than OECD countries over the last 20 years. Korea ranked 13th position in 2008 among all the OECD countries8).
The ratio of NMR in IMR was 66.7% in 1993 and dropped to 53.1% in 2009, but NMR still consists of approximately half of IMR, which shows that neonatal mortality has an important place in IMR in Korea, and neonatal period management is much more important.
In changes in the ten major causes of neonatal death from 1996 to 2008 in Korea, respiratory distress of newborns, diseases of the blood and blood-forming organs as well as certain disorfers involving the immune mechanism, symptoms, signs and abnormal clinical and laboratory findings, NEC, other congenital malformation, and others increased in ratio. In contrast, other respiratory conditions originating in the perinatal period, bacterial sepsis of newborns, disorders related to length of gestation and fetal growth, other respiratory conditions originating in the perinatal period, congenital malfotmation of heart, intrauterine hypoxia, birth asphyxia were decreased in trend.
Common causes of infantile death in 2008 had decreased compared with those in 1996 such as other disorders originating in the perinatal period, congenital malformation of the heart, bacterial sepsis of newborns, disorders related to length of gestation and fetal growth, intra-uterine hypoxia, birth asphyxia. However, some other causes are on the increase, such as respiratory distress of newborn, symptoms, other respiratory conditions originating in the perinatal period, other congenital malformation, diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism. Therefore, establishing solutions against these problems is important10).
Conclusions
The authors reviewed improvements in IMR over the last 60 years and NMR during last 20 years in Korea, finding remarkably encouraging advances. Although Korean IMR is higher than that of Japan, it is much lower than that of the USA and other OECD nations. Changes in the neonatal and infantile causes of death related to improved NMR and IMR were also analyzed. Our analysis may further improve the NMR and IMR in the future in Korea.
Changes in the neonatal and infantile causes of death related to improved NMR and IMR were also analyzed. Our analysis may further improve the NMR and IMR in the future in Korea.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


