


Introduction
Triple A or Allgrove syndrome is characterized by three main conditions: achalasia, alacrima (defective tear formation) and Addison disease1). Achalasia is derived from a Greek word meaning disruption of relaxation2). It is an uncommon idiopathic primary neuromascular disorder involving the smooth muscle layer of the esophagus and the lower esophageal sphincter. This sphincter is the functional barrier between the stomach and esophagus which is impaired in achalasia syndrome. It is characterized by incomplete relaxation of the lower esophageal sphincter and decreased peristalsis of the smooth muscle esophageal3). Achalasia can be the first manifestation of triple-A syndrome. Adrenal insufficiency and alacrima are asymptomatic in some cases; therefore, closer examination should be performed to detect these disorders. Sudden death can occur because of adrenal crisis. Some affected individuals show slowly progressive neurological symptom such as dysautonomia and bulbar involvement4). Allgrove syndrome is very rare and one such case was presented to us as an edentulous child.
Case report
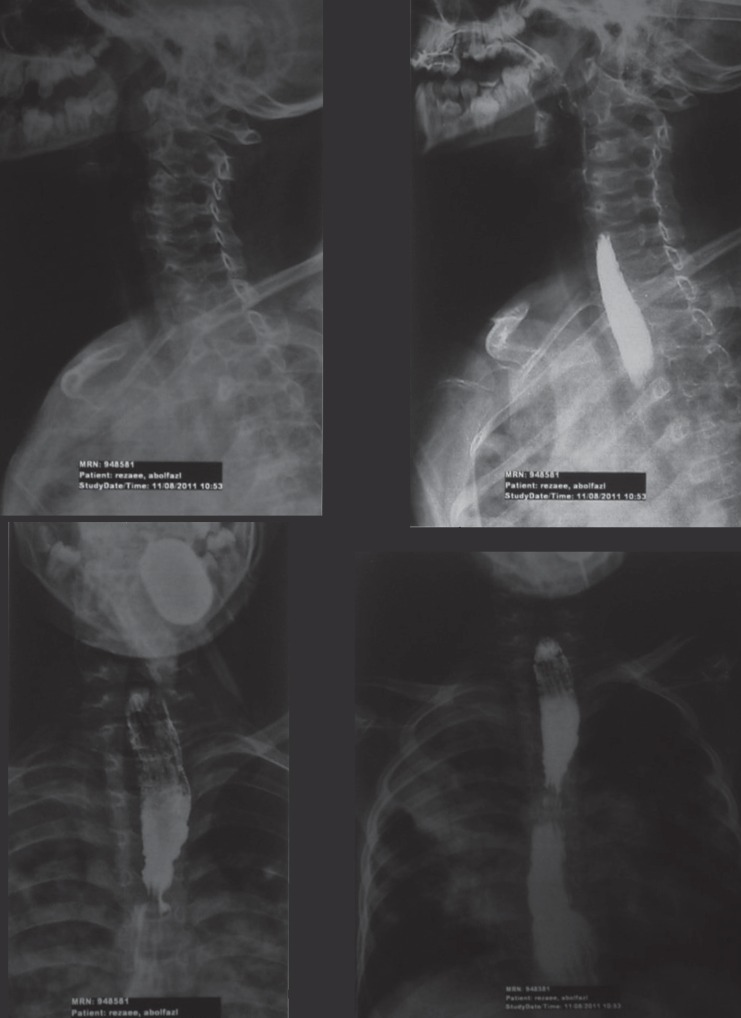
A 15-year-old boy complaining of missing teeth referred to oral medicine department of dental faculty of Hamadan University of Medical Sciences (Fig. 1). He could not eat properly and suffered from his appearance. In the oral examination, many teeth roots with sever caries and second molars could be detected (Fig. 2). He had a very poor hygiene condition and wore a very inappropriate partial denture. In the past he had complained about pain associated with swallowing difficulties, vomiting and weight loss. In his medical history, X-ray examination after barium ingestion by the patient, showed that the contrast passed through different parts of the esophageal. Barium passing through esophageal took place very slowly and with delay (Fig. 3). Sever constriction in the distal esophagus in cardia area with achalasia view was evident. During esophageal dilation, parietal irregularities caused by spasms could be seen locally. Chest X-ray showed the size of a normal heart shadow (Fig. 4). Fairly uniform opacity based on the upper half of the right lung and pre Hillary was evident, causing the disappearance of pericardium and mediastinum. Uniform opacity could be seen in other parts of the right lung and left middle lung. There was no obvious space-occupying lesion in the chest wall. The findings were the most suggestive of bronchopneumonia. On further investigation, it was found that he suffered of adrenal insufficiency (Addison disease) and alacrima. The patient was underwent Heller's myomectomy surgery 3 years ago. Prednisolone, vitamin D and calcium supplements were prescribed for him. At this time, height was 150 cm, weight 41 kg and body mass index was 18.2 kg/m2. The patient was reported to have some symptoms such as fatigue, anxiety, tendency to eating sweet and salty foods, moodiness and poor concentration few years ago. Laboratory tests revealed decrease of cortisole hormone (4.3 mcg/dL; references range, 5–23 mcg/dL) and increase of plasma adrenocorticotropic hormone (ACTH) concentration (77 pg/mL; references range, 10–60 pg/mL). The symptoms being improved, he was treated with hydrocortisone and was currently using maintenance dose. He would visit doctor for hormone values check-up yearly. Growth, development and puberty were normal. There was no pathologic manifest in breathing sound and evidence of osteoporosis was negative.
Mandibular alveolar ridge resorption was developed partly in his age. Due to the gastric reflux, repeated vomiting, chemical erosion, tendency to eating sweet foods and poor oral hygiene, the teeth have decayed rapidly. Also, due to inadequate root length remaining after the removal of decay, all of them were extracted. Root canal treatment of mandibular right second molar was performed. Implant treatment was delayed because of the lower age of the patient and economic problem. Maxillary and mandibular temporary complete dentures were provided for the patient in prosthetic dental department of university (Fig. 5).
Discussion
Triple-A syndrome, also known as Allgrove syndrome, is a rare autosomal recessive disorder. This multisystemic disease appears during early childhood and is characterized by prominent features of esophageal achalasia, alacrima, and atypical primary adrenal insufficiency. Alacrima is generally asymptomatic but it can be displayed by history taking. The patients can benefit from use of artificial tears. Also, ophthalmologic symptoms, if present, can be well tolerated. While ACTH insensitivity could barely have manifestation such as asthenia, it might be wrongly diagnosed as muscle fatigue. The hormone values must be checked-up yearly because acute adrenal crisis could lead to sudden death4).
The etiology of achalasia esophageal motility is unclear. It is characterized by degeneration of enteric nervous system that innervates the esophageal muscles and lower esophageal sphincter. Studies have found no gender distribution5).
This syndrome was introduced by Dr. Jeremy Allgrove and colleagues for the first time in 19786). Since then, almost 200 patients with this disorder have been reported around the world4). Wallace and Hunter7) presented an 8-year-old girl with AAA syndrome. She had dark pigmentation on her hands skin. Papageorgiou et al.8) reported the genetic basis of triple-A syndrome in a Greek family. All family members (parents and her sibling) had mutation in AAA gene and the parents were affected. Nakamura et al.9) focused on the neurological disorder in a 60-year-old Japanese man with Allgrove syndrome, and his parents and siblings were unaffected. Gebril10) reported an Egyptian family with two affected siblings. Unlike our case, they had neurological symptoms. They were diagnosed in childhood as well as our patients. While these patients usually consult with physicians because of vomiting, dysphagia and weight which loss, our case suffered from similar symptoms 3). Yassaee et al.11) investigated 5 unrelated families clinically diagnosed with Allgrove syndrome for AAA gene mutation. Accordingly, while some cases do not have adrenal insufficiency, our case was affected11). Vitamin D and calcium supplements are prescribed for the prevention of osteoporosis.
Genetic examination indicated mutations in both alleles of AAA gene coding for a special 546-amino-acid protein denominated ALADIN. Although scientists have discovered that the mutations are related to chromosome 12q13, they have not identified the role of ALADIN protein, yet4). Genetic test of our patient did not indicate mutation in the AAA gene. Therefore, the genetic cause of the syndrome is unknown in this child patient.
To date, 90 families with affected members have been reported worldwide8). In our report, although the parents were nonconsanguineous and healthy, the patient's sister was affected. She was 19 years old and had the same symptoms of her brother. Her first complaint was eating problem. Achalasia was proved after examination. Then her adrenal insufficiency and alacrima were discovered. She had lost all of her tooth, too. Our case was diagnosed in childhood and did not have dark pigmentation lesions on skin and neurologic disorders. The parents of our case were healthy and he did not have mutation in genetic test.
Autonomic dysfunction and peripheral neurologic manifestation is detected in some adult cases that may progress slowly during the time4). Since achalasia is a rare condition in children, affected child with adrenal insufficiency should undergo more medical examinations. In conclusion, we report an edentulous boy with achalasia, adrenal insufficiency, and alacrima, which are main conditions of triple-A syndrome.




 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


