


Introduction
The Epstein-Barr virus (EBV), which belongs to the γ-herpesviridae family, causes a persistent and lifelong latent infection in patients worldwide. Infectious mononucleosis, the well-known related clinical syndrome, is triggered by the EBV1). Its main presenting symptoms are fatigue, malaise, sore throat, and generalized lymphadenopathy2). Hepatic involvement may occur as symptoms of EBV infection, including hepatomegaly, jaundice, and abnormal liver function test3). Although gastric involvement is extremely rare, gastritis, lymphoma, and gastric cancer can develop. Concomitant acute gastritis rarely occurs, and only a few cases have been reported in adults and adolescents. There have been no case reports to date in children. We report a case of EBV gastritis documented in a 4-year-old girl who presented with fever, cervical lymphadenopathy, and abdominal pain.
Case report
A 4-year-old girl was hospitalized via the Emergency Department with a 6-day history of fever, headache, and a 3-day history of upper and periumbilical abdominal pain. There was no vomiting and diarrhea, but the abdominal pain was aggravated with the complaint of anorexia. She had a history of febrile convulsion and tic disorder. No notes about supplementary food or special doses of medicines were found.
Physical examination showed a temperature of 38.5℃, blood pressure of 114/63 mmHg, heart rate of 96 beats/min, and respiratory rate of 24 breaths/min. Pharyngeal injection and cervical lymphadenopathy were observed. The abdomen was flat and soft. Upper quadrant and periumbilical tenderness were noted with normal bowel sounds. The liver edge was palpable 5 cm below the right low costal margin. The spleen was enlarged. There was no skin rash.
The cell blood count examination revealed the following; white blood cell count 11,120/µL (segment, 6.0%; lymphocyte, 40.0%; atypical lymphocyte, 37.0%), hemoglobin level 11.4 g/dL, hematocrit 33.1%, and platelet count 254,000/µL. Results of liver function tests were abnormal, including aspartate transaminase (105 IU/L), alanine transaminase (166 IU/L), alkaline phosphatase (363 IU/L), γ-glutamyl transpeptidase (229 IU/L), and albumin (3.4 g/dL). Other results were as follows: serum lactate dehydrogenase 799 IU/L and total bilirubin 0.6 mg/dL. Serologic tests were negative for hepatitis B viral surface antigen as well as antibodies against hepatitis A virus, hepatitis C virus, and cytomegalovirus. Blood culture failed to grow any bacteria. Monospot testing for heterophil antibody was negative. Serum IgM antibody for EBV capsid antigen and IgG antibody for EBV nuclear antigen were negative. Polymerase chain reaction performed with peripheral whole blood was positive for EBV DNA with a viral load of 8,180 copies/mL.
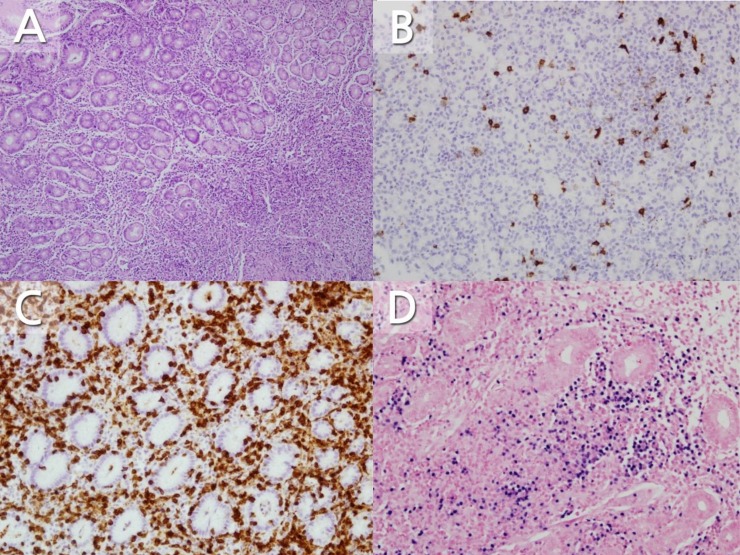
Abdominal ultrasonography showed hepatosplenomegaly, multiple enlarged lymph nodes along the greater curvature of the stomach, and enlarged periportal and ileocolic lymph nodes. Diffuse thickening of the gastric wall and prominent enhancement of the mucosal layer and multiple enlarged lymph nodes along to the greater curvature of stomach were detected on a computed tomography scan, suggesting lymphoproliferative disease and infectious disease (Fig. 1). Due to li2016-12-16mitations of the radiographic findings for differentiating the lymphoproliferative disease and infectious disease, esophagogastroduodenoscopy (EGD) with biopsy was performed, which revealed edematous mucosa in the antrum and body of the stomach. The esophageal and duodenal mucosa findings were nonspecific. Since endoscopic findings were not suggested for gastric lymphoproliferative disease, we easily thought the possibility of EBV gastritis. Histological findings of hematoxylin and eosin staining revealed expansion of the lamina propria and a proliferation of atypical lymph nodes in the mucosa (Fig. 2A). No eosinophils were noted on biopsies. Immunohistochemical staining showed the expression of each T-cell marker (CD3 and CD45RO) and B-cell marker (CD20 and CD79a) (Fig. 2B, C). An EBV-encoded small RNA in situ hybridization test showed positive lymphocytes in the lamina propria (Fig. 2D). A campylobacter-like organism test was negative for Helicobacter pylori. The abdominal pain and sore throat alongside with cervical lymphadenopathy improved with histamine 2 (H2) receptor antagonist and supportive care. The patient was discharged on the 10th day of hospitalization. Two months after discharge, the edematous gastric antral and body mucosa were normal on a follow-up EGD. The biopsy showed no atypical lymph node proliferation of the gastric mucosa and an in situ hybridization test was negative.
Discussion
We experienced a rare case of EBV gastritis that developed in a healthy child as a manifestation of infectious mononucleosis secondary to EBV infection. The diagnosis was established by proving EBV in gastric biopsies with in situ hybridization, and the patient recovered spontaneously due to the infection's self-limiting nature.
As noted previously, EBV gastritis is rarely reported. We found only 6 case reports of EBV gastritis in the literature (Table 1)1,4,5,6,7,8). Here we presented a case of EBV gastritis in a previously well 4-year-old girl. To our knowledge, this is the first case report of EBV gastritis in a young child.
EBV infection-related diseases include infectious mononucleosis, multiple organ disease, complications caused by acute infection, lymphoproliferative disease, and certain types of cancer9). Infectious mononucleosis is an acute disease caused by EBV infection. Its features are atypical lymphocytosis on peripheral blood, fever, and generalized lymphadenopathy10). As mentioned above, our patient had typical clinical symptoms and signs of infectious mononucleosis but other previous reports were not. There were no typical symptoms and signs of infectious mononucleosis in previous reports but their patients all had atypical lymphocytosis on peripheral blood. Related gastrointestinal cancers include gastric non-Hodgkin's lymphoma, gastric T-cell lymphoma, gastric adenocarcinoma, and esophageal cancer11,12,13). Neurologic or blood disorders rarely occur14,15).
Making the clinical diagnosis of EBV infection is usually simple. It can be done by serological tests for EBV and extracting heterophil antibody. Serum specific antibodies for EBV are viral capsid antigen IgM/IgG, EBV early antigen IgG/IgM, and Epstein-Barr nuclear antigen IgG. Polymerase chain reaction for EBV DNA is also available. Our patient had fever, sore throat, and cervical lymphadenopathy. Although the specific serum antibodies were all negative, the diagnosis of infectious mononucleosis was confirmed by the presence of EBV load in assays of DNA extracted from the peripheral blood.
EBV infection is simply diagnosed with serological testing. However, EBV gastritis can occur without positive serological evidence. As such, it is possible to overlook EBV even in patients with gastrointestinal symptoms. Our case along with the previous cases shows that EBV gastritis selectively invades the stomach without involving lesions of the esophagus and duodenum1,6).
EBV gastritis might be confused with various types of lymphoma radiographically, histologically, and endoscopically. Kitayama et al.6) presented that it could be mis-diagnosed as diffuse B-cell lymphoma at the first assessment. Moreover, EBV gastritis can involve acute or chronic in nature, and it is difficult to distinguish it from other types of gastritis such as Helicobacter gastritis and lymphocytic gastritis2,8). Various reports of endoscopic findings stated that EBV gastritis was accompanied by a range of conditions from mucosal hypertrophy with partial edema to ulcerative lesions with irregular margins1).
Since endoscopic appearances of EBV gastritis were various as shown in other cases, performing biopsies with in situ hybridization could be helpful for confirming the diagnosis. In our case, EGD was performed to evaluate the diffuse thickening of the gastric wall visible on imaging studies. EBV gastritis was diagnosed by biopsies with in situ hybridization based on our suspicion judging by the patient's clinical manifestation. And our patient was recovered with using H2 receptor antagonist and supportive care, which was consistent with previous reports1,5,6,7,8).
In summary, we reported a rare case of EBV gastritis in a 4-year-girl presenting with upper and periumbilical abdominal pain as well as fever, sore throat, and cervical lymphadenopathy. This is the first case of EBV gastritis in an early childhood. EBV-associated gastric involvement was carefully investigated in the case of upper digestive symptoms in the clinical situation of highly suspicious EBV infection.
Serological testing for EBV infection and biopsies with in situ hybridization by EGD are useful tools to clarify EBV-associated gastric involvement.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


