




Introduction
Inflammatory bowel disease (IBD) is a chronic inflammation of the gastrointestinal tract that presents with recurring bouts of inflammation and remission. The 2 most common types of IBD are Crohn disease (CD) and ulcerative colitis (UC) [1,2]. Pediatric IBD, which was previously rare in Koreans, has shown a rapid rise in incidence after the 1990s, with a pronounced increase over the last 5 years. The age of onset of IBD is 15–25 years, and CD is more common in children than in adults [1]. Extraintestinal manifestations are varied from 25% to 40% in both adults and children with IBD, but kidney and lower genitourinary involvement has been reported in 4%–23% of adult patients with IBD and 1%–2% of children with IBD [2]. Urinary calculi, fistulas, and renal tubular damage are known to occur, and although renal parenchymal disease is relatively rare, cases showing glomerulonephritis (GN), minimal-change disease (MCD), secondary (AA-type) amyloidosis, and interstitial nephritis are being commonly reported. Based on references described in the literature, immunoglobulin A (IgA) nephropathy accounts for the largest percentage of disease at 24%, followed by interstitial nephritis (19%), acute tubular injury (8%), proliferative GN (7%), and MCD (5%) [2].
We evaluated the clinical manifestations of renal complications in children and adolescents with IBD in 2 tertiary centers in Korea to enable early detection and prompt treatment of renal complications.
Materials and methods
We retrospectively reviewed the medical records of 456 children and adolescents aged <20 years who had been diagnosed with IBD at the Kyungpook National University Hospital and Samsung Medical Center since 2000. The diagnosis of IBD was based on a combination of clinical evaluations including history, physical and endoscopic examination, histopathological findings, imaging, and serological assays for antineutrophil cytoplasmic autoantibody (ANCA) and anti-Saccharomyces cerevisiae antibody [3-7].
Additionally, we analyzed age, sex, medication use, IBD disease activity, and renal manifestations, such as hematuria, proteinuria, acute kidney injury, chronic kidney disease (<90 mL/min/1.73 m2 over 3 months), and reviewed other renal and urinary tract abnormalities. In particular, patients with proteinuria were screened in the first urine in the morning to exclude orthostatic proteinuria. The results of histopathological examination in patients who underwent renal biopsy were compared with the IBD disease activity. IBD disease activity can be assessed using the Pediatric Crohn Disease Activity Index (PCDAI) and the Pediatric Ulcerative Disease Activity Index (PUCAI) scores. These are noninvasive, valid, highly reliable, and responsive indices to assess disease activity in pediatric patients with CD and UC. PCDAI scores range from 0–100, and this index classifies disease activity as no disease activity (<10), mild disease activity (11–30), and moderate-to-severe disease activity (≥30). PUCAI scores range from 0–85 and this index classifies disease activity as no disease activity (<10), mild disease activity (11–34), moderate disease activity (35–64), and severe disease activity (≥65) [1,8]. The Institutional Review Board at Kyungpook National University Hospital, Daegu, South Korea reviewed and approved this study (approval number: KNUMC_2017-10-007).
Continuous variables were expressed as means±standard deviations (SD). The Student t test and the Mann-Whitney test were used to analyze continuous variables. The chi-square test was used to analyze categorical variables. A P value of <0.05 was considered statistically significant. All statistical analysis was performed using the R software, ver. 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Our study comprised 456 children with IBD including 299 boys (65.6%) and 157 girls (34.4%) with a mean age±SD of 14.1±3.0 years. The mean follow-up period was 4.61±2.93 years. The study included 346 children with CD (75.9%) and 110 with UC (24.1%), and the incidence of CD was greater than UC. Children with IBD were treated with various immunosuppressants including oral prednisolone, 5-aminosalicylic acid (5-ASA, sulfasalazine and mesalazine), azathioprine, infliximab, and adalimumab [3]. The renal function was assessed by measuring the estimated glomerular filtration rate (eGFR) less than 90 mL/min/1.73 m2 for more than 3 months. Of the 456 patients, 11 patients (0.02%) had eGFR <90.
Among the 456 children, 67 (14.7%) showed confirmed renal manifestations, and 59 were identified as children with CD and 8 as children with UC. We observed 26 children (38.8%) with isolated hematuria, 30 (44.8%) with isolated proteinuria, and 11 (16.4%) with hematuria and concomitant proteinuria. During the course of evaluation to detect the cause of hematuria and concomitant proteinuria, we identified 1 child with a urinary stone and 1 with hydronephrosis.
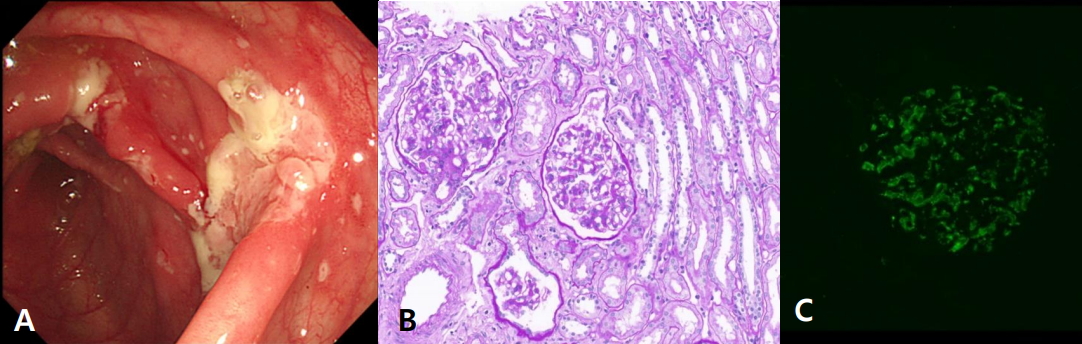
A renal biopsy was performed in 7 children with CD. Of them, 5 children showed both microscopic hematuria and proteinuria. Persistent microscopic hematuria and recurrent gross hematuria was observed in 2 children. Complement 3/4 level, spot urine calcium/creatinine level, ANCA, antinuclear antibody (ANA), and anti-ds DNA were examined in 7 patients who underwent renal biopsy. All of the patients were negative except 1 patient. This patient tested positive for ANCA, ANA, and anti-dsDNA, and IgA nephropathy (Haas classification I) was identified on renal biopsy. Histopathological examination revealed 5 children with IgA nephropathy (71.4%) and in 1 child with Henoch-Schönlein purpura (HSP) nephritis (14.2%), whereas 1 child (14.2%) showed no histopathological abnormalities (Table 1). Based on the Haas classification of IgA nephropathy, 2 children were diagnosed with Haas subclass I, 2 with Haas subclass III, and 1 with Haas subclass IV (Fig. 1). Additionally, 1 child with HSP nephritis was diagnosed with class II disease based on the histological classification proposed by the International Study of Kidney Disease in Children. Angiotensin receptor blockers and/or angiotensin converting enzyme inhibitors were administered to 5 children with IgA nephropathy and 1 with HSP nephritis, and oral prednisolone was administered to 2 of 6 children.
Disease activity was evaluated in 102 children, of which 81 showed CD and 21 showed UC. Of note, 35 of these 102 children (30 with CD, 5 with UC) presented with renal manifestations. Disease activity was assessed based on the PCDAI for CD and the PUCAI for UC. The mean PCDAI score was 8.5 with renal manifestations and 2.2 without renal manifestations, and the mean PUCAI score was 21 with renal manifestations and 6.3 without renal manifestations. No significant correlation was observed between the IBD disease activity and the presence of renal manifestations in 102 children in whom we were able to assess disease activity. Disease activity was mild, and the disease was well controlled in all children (Table 2).
Discussion
IBD is a chronic relapsing disorder of unknown etiology that includes 2 distinct disorders—CD and UC. Approximately 2 decades ago, IBD was considered a rare disease among Korean adults. However, the incidence of IBD has shown a rapid rise after the 1990s. Recently, the incidence of pediatric IBD has shown a steep rise in Korea since 2000 [1]. Pediatric IBD usually demonstrates a more severe presentation of IBD than that in adults with widespread infiltration and more common colonic lesions.
Extraintestinal manifestations vary from 25%–40% in both adults and children with IBD [7,9,10]. In pediatric IBD patients, 6% show at least one extraintestinal manifestation before a confirmed diagnosis of IBD is established, and an extraintestinal manifestation is known to develop in 29% children within 15 years of diagnosis [11]. The eyes (uveitis, episcleritis, retinitis), the skin (erythema nodosum, pyoderma gangrenosum), joints (arthritis, sacroiliitis, ankylosing spondylitis), hepatobiliary tract (sclerosing cholangitis, autoimmune chronic hepatitis), and respiratory tract (chronic bronchitis, bronchiectasis, bronchiolitis obliterans with organizing pneumonia) are most commonly involved in children with extraintestinal manifestations [12-15].
Among the IBD patients, renal manifestations account for 4%– 23% in adults [2], but only in 1% to 2% of children with IBD had renal manifestations such as proteinuria, hematuria, renal failure and uremia [9,12,14]. It was reported that renal manifestations have a 3-fold increased risk in males and a 10-fold increased risk in CD compared with UC [9,13]. Renal complications in IBD include nephrolithiasis, GN, interstitial nephritis, AA-type amyloidosis, and enterovesical fistula, among other such conditions [10,16]. In children, GN, renal artery stenosis, amyloidosis, renal failure, ureteral compression, and perinephric abscesses have been reported [7,14].
To date, the most common histopathological finding in the kidneys in these patients is interstitial nephritis secondary to the use of 5-ASA. 5-ASA and its derivatives (sulfasalazine and mesalazine) are widely used as first-line drugs of induction and maintenance in patients with IBD [8,17,18]. However, lately, following the popularity of new biological agents such as infliximab and adalimumab, the use of 5-ASA and its derivatives in patients with IBD and the consequent prevalence of renal complications caused by these drugs have been decreasing. In our study, no child was diagnosed with interstitial nephritis caused by 5-ASA.
A study evaluating the properties of renal stones observed in patients with CD demonstrated that the stones were predominantly composed of calcium oxalate and phosphate. The incidence of renal stones in patients undergoing an ileostomy is significantly high. The probability of renal stone formation was observed to be 8 fold higher in children with a urinary pH ≤6.0 than in those with a urinary pH ≥6.5 [19]. In our study, we incidentally identified 1 child with a urinary stone in the course of assessing the causes of hematuria and concomitant proteinuria.
Ambruzs et al. [2] reported the histopathological spectrum of renal biopsies in patients with IBD. Most patients with IBD with renal complications showed involvement of glomerular and tubulointerstitial components. IgA nephropathy was the most common diagnosis (24%), followed by interstitial nephritis (19%), arterionephrosclerosis (12%), acute tubular injury (8%), proliferative GN (7%), and MCD (5%). In addition, there have been several case reports suggesting the pathogenetic association between IgA nephropathy and CD in children [20,21]. Takemura et al. [20] reported 10-year-old boy patient who had proteinuria with macroscopic hematuria and from the renal biopsy he was proven IgA nephropathy. At the age of 13 years, the patient developed CD and IgA nephropathy recurred, simutaneously. McCallum et al. [21] reported 11-year-old girl who presented with recurrent gross hematuria, she was proven IgA nephropathy from renal biopsy and later, she developed CD.
Shaer et al. [16] suggested that immune complex deposition may play an important role in the pathogenesis of GN associated with IBD. They concluded that all renal manifestations occurred in the setting of active bowel disease and that the improvement in GN was paralleled by the institution of treatment and subsequent improvement in the gastrointestinal disorder, confirming that GN is indeed an extra-intestinal manifestation of IBD. Forshaw et al. [22] also suggested that GN appeared to show a direct correlation with intestinal disease activity and improvement of renal function after remission of bowel inflammation has been conclusively demonstrated. The prevalence of IgA nephropathy was significantly higher in those with IBD than in those without IBD [10]. However, interestingly, because our study showed no correlation between renal manifestations and IBD disease activity, we conclude that this result suggests the role of other contributory pathogenetic mechanisms in addition to IBD disease activity. Therefore, it is necessary to confirm renal manifestations by performing regular urinalysis even in patients with IBD without disease activity.
This study was limited in that periodic urinalysis was not performed in all children with IBD. It was unclear when the renal manifestations occurred, and we cannot exclude the possibility of pre-existing renal manifestations that might have progressed and been noticed only during the study period. Thus, it is possible that the relevant tests were not performed despite an indication for a biopsy, and thus the observed biopsy result may not be representative of the whole.
However, this study is the first to report the prevalence and clinical manifestations of kidney-related symptoms in children with IBD using a large-scale Korean pediatric IBD series, and further larger prospective observational studies are needed in the future. Children with IBD are more likely to show renal symptoms than healthy children and adolescents. Therefore, regular urinary screening and evaluation of renal function are necessary for early detection and prompt treatment of renal complications.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


