




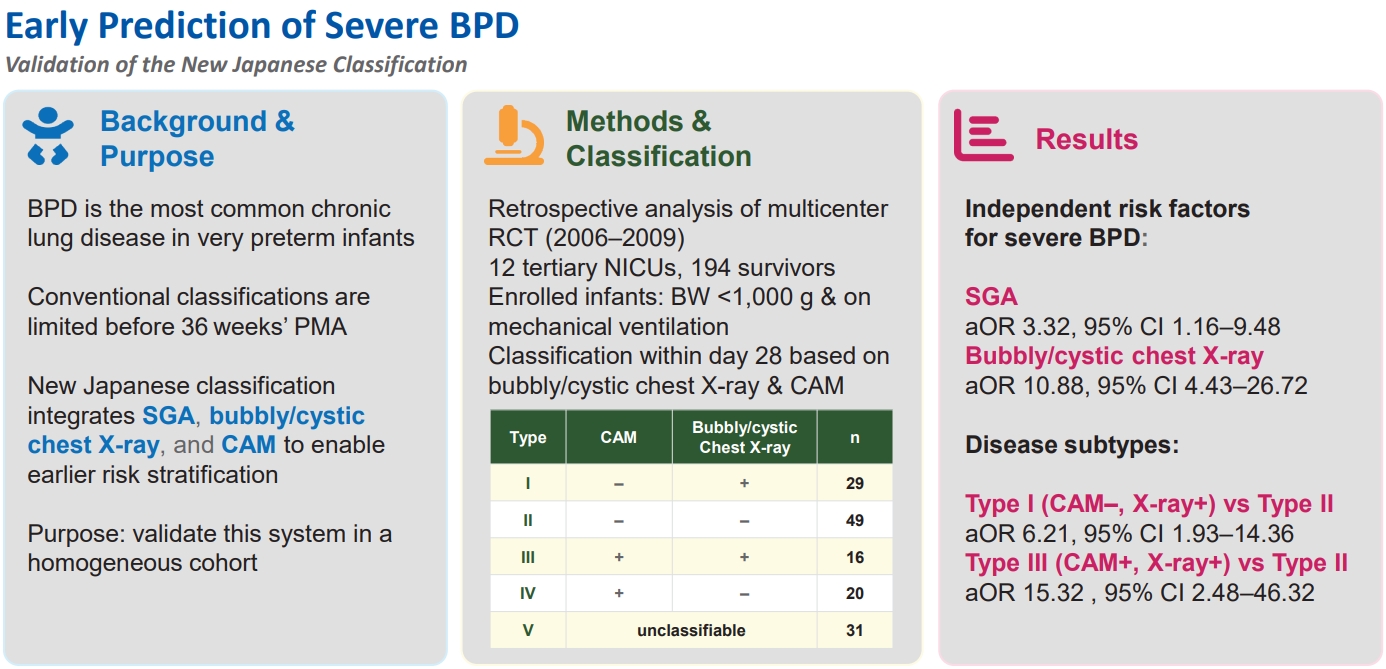
Graphical abstract. BPD, bronchopulmonary dysplasia; PMA, postmenstrual age; SGA, small for gestational age; CAM, chorioamnionitis; RCT, randomized controlled trial; NICU, neonatal intensive care unit; BW, birth weight; aOR, adjusted odds ratio; CI, confidence interval.
Introduction
Bronchopulmonary dysplasia (BPD) is the most prevalent chronic lung disease in very low birth weight (BW) infants; it causes long-term respiratory complications and influences neurodevelopmental outcomes [1-4]. Conventional classifications employed in Western countries remain limited, particularly in predicting and guiding interventions before 36 weeks’ postmenstrual age (PMA); thus, new systems that enable earlier prediction and stratification are warranted [5]. An ideal classification should integrate the pathogenesis, endotypes, and phenotypes of BPD and lead to early prediction and intervention [6].
In Japan, an original BPD classification has been employed since the 1990s, in which disease severity was evaluated based on etiological and phenotypic factors, such as respiratory distress syndrome (RDS), intrauterine infection/inflammation, and chest radiographic findings [7,8]. However, improvements in the survival of very preterm infants, advances in respiratory management, changes in RDS treatment strategies, and the widespread use of antenatal corticosteroids have increased the need to reevaluate the validity of this classification [9]. A recent scoping review identified placental inflammation, small for gestational age (SGA) status, and bubbly/cystic changes on chest radiographs as risk factors for severe BPD [10], which resulted in the revision of the Japanese classification [11]. In the revised system, diagnosis is made at 28 days of age and subtypes are defined according to 3 factors: (1) histologically proven chorioamnionitis (CAM), (2) diffuse bubbly/cystic changes on chest radiographs, and (3) SGA status (Table 1).
However, to what extent the new Japanese classification corresponds to conventional international systems and whether it is useful for the early prediction of severe disease in real-world clinical data remain unclear. In particular, factors such as SGA status, radiographic findings, and placental pathology can be assessed from the perinatal period, indicating their potential utility for early intervention and outcome prediction. Previous retrospective studies using large national databases in Japan have indicated the usefulness of these factors [12], however, no study has validated the classification in a homogeneous cohort enrolled in a randomized controlled trial (RCT). Therefore, the present study aimed to elucidate the association between the revised Japanese classification and the development of severe BPD through a secondary analysis of cases included in an RCT of inhaled corticosteroids [13].
Methods
This study is a retrospective secondary analysis of cases included in a multicenter, double-blind, randomized, placebo-controlled trial of inhaled corticosteroids conducted in 12 tertiary neonatal intensive care unit (NICUs) in Japan between June 2006 and December 2009 [13]. The study was registered at Saitama Medical Center (registration No. 2025‑052) and approved by the Research Ethics Committee of Saitama Medical Center, Saitama Medical University (IRB No. 2025‑052). The original trial included very-low-birthweight infants (<1,000 g) requiring mechanical ventilation. Randomization was performed using an Internet-based allocation system with minimization, stratified by gestational age (GA), RDS presence or absence, and study site. Of the 211 infants enrolled in the original RCT, 194 survivors were included in the final analysis.
The primary outcome was severe BPD, defined as the requirement for oxygen supplementation with an effective FiO2 >0.30 or ventilator dependence at 36 weeks’ PMA, in accordance with the U.S. National Institute of Child Health and Human Development (NICHD) criteria [14] used in the original RCT. The requirement for written informed consent was waived by the institutional review board because the study involved anonymized secondary data from a completed RCT.
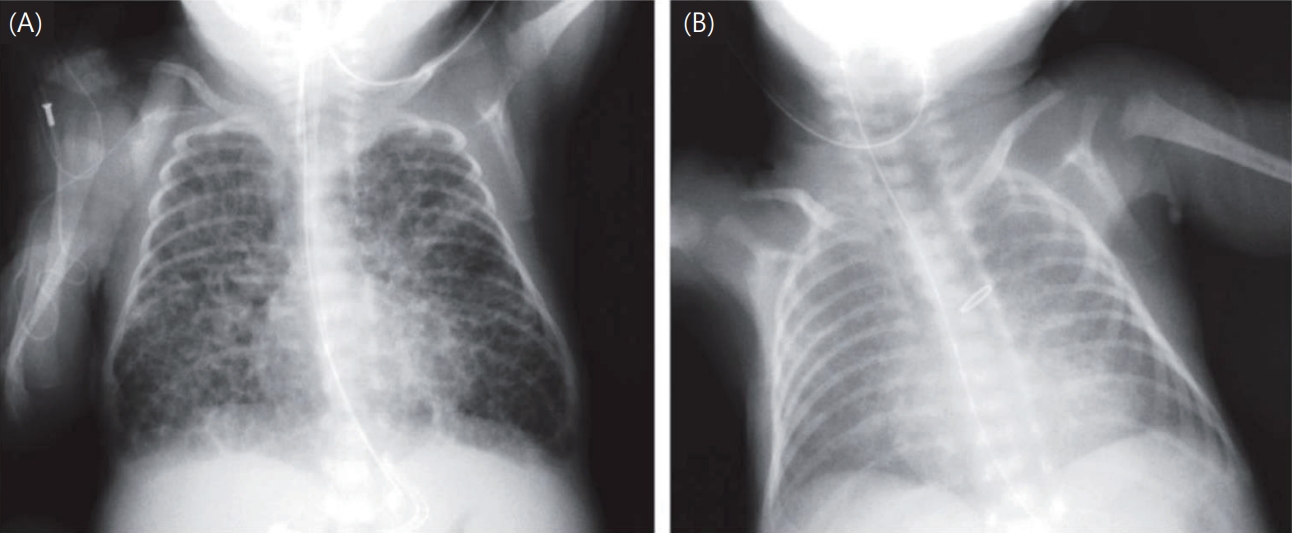
Exposure factors were determined according to the revised Japanese BPD classification. SGA was defined as a BW below the 10th percentile for gestational age according to the Japanese neonatal anthropometric reference curves [15]. These population‑specific values were used because harmonized international birth‑weight z scores were unavailable in the original RCT dataset. Chest radiographs at 28 days were evaluated, and infants judged as having bubbly/cystic changes in the original RCT by participating centers were classified as positive in the present analysis. Representative examples of bubbly/cystic and non‑bubbly chest radiographs are shown in Fig. 1 [16]. In the original RCT, detailed documentation about who interpreted the radiographs and under what conditions were lacking, so the number and specialties of readers and whether the readings were blinded are unknown. Because the images were not available for review, interobserver reproducibility could not be assessed. This limitation reflects real‑world practice in Japan, where neonatologists rather than radiologists typically interpret NICU chest radiographs, and standardized blinded procedures are not routinely used [9]. CAM was defined as acute inflammatory cell infiltration in the amnion, subchorion, or chorion on placental histopathology. RDS was defined as respiratory distress from birth combined with characteristic chest radiographic findings, with surfactant replacement therapy administered as needed. PDA was diagnosed via echocardiography. Data on maternal steroid use and other clinical background variables were extracted from the original RCT database. Potential confounders included BW, GA, sex, 5-minute Apgar score, maternal steroid use, RDS, and PDA. Continuous variables were expressed as mean±standard deviation or median (interquartile range) and compared using the t test or Mann-Whitney U test, depending on normality. Categorical variables were compared using the chi-square test or Fisher exact test. For the primary outcome of severe BPD, univariate and multivariate logistic regression analyses were conducted to calculate odds ratios (ORs) with 95% confidence intervals (CIs). Initially, univariate analyses were conducted to evaluate the association between each candidate variable and severe BPD. Variables with a value of P<0.10 in the univariate analysis or considered clinically relevant (including antenatal corticosteroid exposure) were entered into the multivariate model, alongside classification-related factors (SGA, bubbly/cystic chest x-ray findings, and CAM). A subgroup analysis was also conducted for infants born at <27 weeks’ GA to evaluate the association between BPD subtypes and severe BPD. A 2-sided value of P<0.05 was considered statistically significant. In addition, the predictive performance of the final multivariable logistic regression model was evaluated. Discrimination was assessed using the area under the receiver operating characteristic (ROC) curve, and calibration was examined using the Hosmer-Lemeshow goodness-of-fit test. All statistical analyses were conducted using IBM SPSS Statistics ver. 29.0 (IBM Co., USA).
Results
1. Patient characteristics
Among the 194 infants analyzed, the BPD subtypes at day 28 were as follows: I (CAM [-], bubbly/cystic chest x-ray [+]; n=29, 14.9%), II (CAM [-], bubbly/cystic chest x-ray [-]; n=49, 25.2%), III (CAM [+], bubbly/cystic chest x-ray [+]; n=16, 8.2%), IV (CAM [+], bubbly/cystic chest x-ray [-]; n=20, 10.3%), type V (unclassifiable; n=31, 15.9%), and non-BPD (n=49, 25.2%). Significant differences were observed among the groups in terms of BW (P=0.01), gestational age (P<0.01), and Apgar score at 5 minutes (P=0.023). PDA frequency also significantly differed across the groups (P<0.01). Contrarily, no significant differences were observed in maternal antenatal steroid use, cesarean delivery, or sex distribution. RDS was common overall but exhibited significant variation among the subtypes (P<0.01) (Table 2).
2. SGA, chest x-ray, and placental pathology
A total of 80 infants (41.2%) developed severe BPD at 36 weeks’ PMA. 25 infants were SGA, which was significantly associated with severe BPD (OR, 3.58; 95% CI, 1.46–8.76; P<0.01). Furthermore, 45 infants had bubbly/cystic findings on chest x-ray, which exhibited the strongest association (OR, 13.8; 95% CI, 5.73–33.40; P<0.01). Placental pathology was present in 86 infants and was associated with severe BPD (OR, 1.92; 95% CI, 1.07–3.43; P=0.045) (Table 3).
3. Multivariable analysis
After adjustment for potential confounding factors (GA, birth weight, sex, 5-minute Apgar score, maternal steroid use, RDS, PDA), SGA status (adjusted OR [aOR], 3.32; 95% CI, 1.16–9.48; P=0.032) and bubbly/cystic findings on chest x-ray (aOR, 10.88; 95% CI, 4.43–26.72; P<0.01) remained as independent risk factors for severe BPD. Contrarily, placental pathology did not show significant association (aOR, 1.45; 95% CI, 0.72–2.94; P=0.30) (Table 4).
4. Association between BPD subtype and severe BPD at 36 weeks’ PMA
Logistic regression analysis was conducted using severe BPD at 36 weeks' PMA as the outcome and subtype II (CAM [-], bubbly/cystic chest x-ray [-]) as the reference. In the univariate analysis, subtype I (CAM [-], bubbly/cystic chest x-ray [+]) (OR, 5.41; 95% CI, 1.93–15.16; P<0.01) and subtype III (CAM [+], bubbly/cystic chest x-ray [+]) (OR, 12.06; 95% CI, 2.46–59.20; P<0.01) exhibited significant association with an increased risk, with subtype III showing the strongest association. Contrarily, subtype IV (CAM [+], bubbly/cystic chest x-ray [-]) (OR, 1.15; 95% CI, 0.40–3.34; P=0.80) and subtype V (unclassifiable) (OR, 2.39; 95% CI, 0.95–5.98; P=0.06) did not show significant association.
After adjustment for gestational age, BW, sex, Apgar score, antenatal steroid use, RDS, and PDA, subtype I (CAM [-], bubbly/cystic chest x-ray [+]) (aOR, 6.21; 95% CI, 1.93–14.36; P<0.01) and subtype III (CAM [+], bubbly/cystic chest x-ray [+]) (aOR, 15.32; 95% CI, 2.48–46.32; P<0.01) remained as independent risk factors for severe BPD. The final multivariable logistic regression model demonstrated good discriminatory performance, with an area under the ROC curve of 0.73, and acceptable calibration (Hosmer-Lemeshow P=0.16) (Table 5).
5. Subgroup analysis (<27 weeks’ GA)
In the subgroup of infants born at <27 weeks GA, logistic regression with subtype II (CAM [-], bubbly/cystic chest x-ray [-]) as the reference showed that subtype III (CAM [+], bubbly/cystic chest x-ray [+]) was associated with the highest risk of severe BPD at 36 weeks' PMA (unadjusted OR, 21.54; 95% CI, 2.52–184.01; P<0.01; aOR, 20.8; 95% CI, 1.80–165.3; P=0.018). Subtype I (CAM [-], bubbly/cystic chest x-ray [+]) was also significantly associated with severe BPD (unadjusted OR, 3.01; 95% CI, 1.03–9.24; P=0.042; aOR, 4.88; 95% CI, 1.23–19.3; P=0.026) (Table 6).
Discussion
This study is the first to apply the new Japanese BPD classification in a retrospective secondary analysis of a cohort from an RCT on inhaled steroids, evaluating its association with severe BPD development at 36 weeks’ PMA. The main findings were as follows: SGA status and bubbly/cystic findings on chest x-ray were independently associated with severe BPD, placental pathology exhibited significance in the univariate but not in the multivariate analysis, and subtypes III (CAM [+], bubbly/cystic chest x-ray [+]) and I (CAM [-], bubbly/cystic chest x-ray [+]) were particularly strongly associated with severe BPD in infants born at <27 weeks’ GA. These results suggest that the new classification enables early risk stratification for BPD progression using information available shortly after birth.
The importance of SGA status demonstrated in this study is consistent with those in previous reports. Fetal growth restriction impairs secondary septation and pulmonary angiogenesis, thereby contributing to BPD severity via reduced alveolarization and increased pulmonary vascular resistance [17,18]. The persistence of SGA status as a risk factor even following adjustment for confounders indicates the importance of optimizing maternal–fetal nutrition to prevent severe BPD development.
Bubbly/cystic changes on chest x-ray were identified as the strongest predictor. Chest radiography, which is generally performed in the NICU, provides a surrogate marker of structural injury without additional burden [19]. These radiographic findings reflect parenchymal heterogeneity, hyperinflation, airway obstruction, and microalveolar rupture, all of which have been demonstrated to prolong oxygen and ventilator dependence [16,20]. The identification of this factor as an independent risk indicates the clinical rationale for early intervention strategies based on imaging, such as optimization of lung volume settings, secretion management, and lung-protective ventilation.
With respect to placental pathology, the previously mentioned scoping review [10] and large-scale studies in Japan [12] have identified placental inflammation as a strong risk factor for BPD development. However, the binary assessment of placental findings (present vs. absent) in this study may have weakened associations by neglecting critical details, such as site, severity, and timing (acute vs. chronic). Previous literature has suggested that intervillositis and funisitis severity is correlated with BPD [21,22]. Therefore, the lack of significance in the multivariate model in this study is likely attributable to methodological limitations in placental pathology evaluation.
In the subtype analysis, both in the overall cohort and in the subgroup of infants born at <27 weeks’ gestation, type III (CAM [+], bubbly/cystic chest x-ray [+]) and type I (CAM [-], bubbly/cystic chest x-ray [+]) were associated with a considerably increased risk of severe BPD. The fact that classification at day 28 reflected disease severity at 36 weeks' PMA supports the intended concept of the new classification as an “early diagnostic” tool. In particular, type III (CAM [+], bubbly/cystic chest x-ray [+]) frequently overlapped with cases of respiratory management difficulty, indicating that this group is a priority target for early intervention.
Recent updates in the conceptual framework of BPD have highlighted limitations of the NICHD 2001 definition, which does not fully reflect contemporary respiratory support practices, long-term developmental outcomes, or distinctions between mild and no BPD. Newer classification systems such as the treatment-based severity criteria aim to incorporate evolving modalities including high-flow nasal cannula and modern noninvasive ventilation [23]. However, the original RCT from which our dataset was derived collected clinical information strictly according to the NICHD 2001 definition, and key parameters required for applying newer criteria (e.g., detailed flow settings and noninvasive ventilatory modes) were not available. Therefore, although the importance of updated definitions is well recognized, the present analysis necessarily employed the NICHD 2001 framework. Future validation using contemporary diagnostic criteria will be essential to determine the broader applicability of this classification.
The strengths of this study include the use of a homogeneous cohort derived from an RCT and the consistent demonstration of associations between SGA status, chest x-ray findings, and subtypes I (CAM [-], bubbly/cystic chest x-ray [+]) and III (CAM [+], bubbly/cystic chest x-ray [+]) with severe BPD, even following adjustment for confounders.
The clinical implications of this classification warrant careful consideration. Infants who are both SGA and exhibit bubbly/cystic radiographic changes within the first 28 days represent a particularly vulnerable group. For these infants, several targeted strategies may be beneficial. Enhanced nutritional management, including early optimization of caloric intake, protein supplementation, and close monitoring of postnatal growth—may help mitigate the growth-related component of their risk [24,25]. In addition, bubbly/cystic patterns may indicate early structural lung injury, and the presence or absence of CAM further suggests whether antenatal inflammation contributed to the disease process. Recognizing these radiographic-pathologic profiles may prompt clinicians to strengthen respiratory surveillance and adjust noninvasive ventilatory support more proactively when signs of worsening lung disease emerge. Integrating this combined information into routine clinical assessment may therefore facilitate earlier identification of high-risk infants and allow timely tailoring of supportive strategies to prevent progression toward severe BPD.
Several limitations should be acknowledged. First, because infants who died were excluded, the association between radiographic severity and adverse outcomes may have been underestimated; this potential selection bias should be considered. Second, as a retrospective secondary analysis, the study was susceptible to missing data and residual confounding; the limited sample size also restricted subgroup analyses, and binary coding of placental pathology may have introduced misclassification. Moreover, outcomes were confined to severe BPD at 36 weeks’ PMA, and differences in ventilator management and oxygen targets across centers could not be fully controlled. Third, the relatively small number of infants classified as SGA limited our ability to perform more granular analyses, such as separating subtypes by SGA status or directly comparing SGA‑related subtypes (e.g., I_s vs. III_s). Additionally, because SGA was defined using Japanese population‑based growth references, the classification may differ from one derived from international standards; anthropometric distributions vary across populations, so generalizability to non‑Japanese cohorts should be interpreted with caution and will require external validation. Finally, the original RCT dataset did not capture details of chest radiograph interpretation (e.g., number and specialties of readers, blinding or duplicate readings), precluding assessment of interobserver agreement and potentially limiting the generalizability of the radiographic findings.
Conclusion
This secondary analysis of an RCT cohort demonstrated the potential utility of the new Japanese BPD classification for severe BPD prediction. Notably, SGA status and bubbly/cystic radiographic findings were independently associated with disease severity and may facilitate effective risk stratification from early postnatal stages. In this study, placental pathology did not reach significance, which is likely attributable to limitations in assessment methods. Future work should incorporate detailed scoring and integrative analyses with other factors.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


