




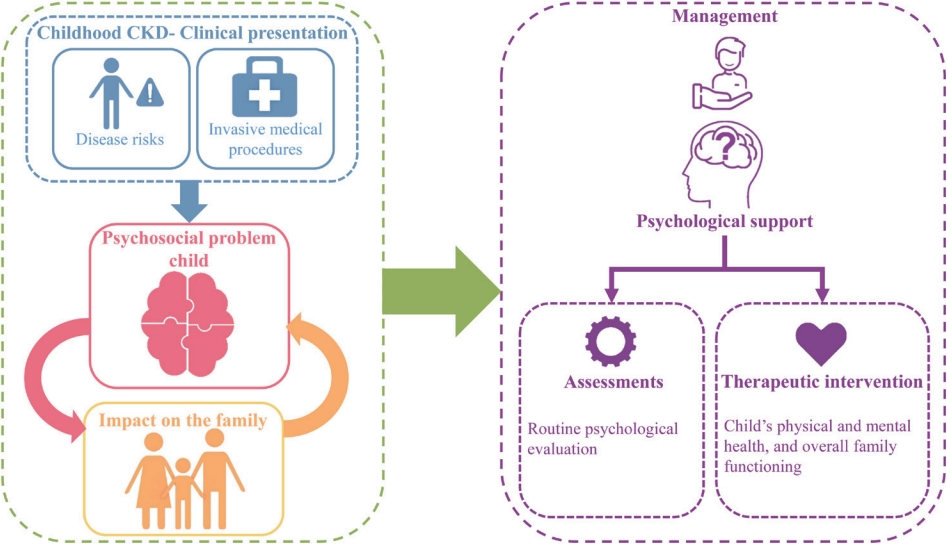
Graphical abstract
Introduction
Chronic illnesses that develop in childhood require longterm treatment affect both the child and the whole family [1,2]. A meta-analytic review reported that children with “physical disorders” (including asthma, cardiac disorders, cancer, diabetes, inflammatory bowel disease, juvenile idiopathic arthritis, neurological disorders, and sensory disorders) had a higher risk of developing internalizing (e.g., anxiety, depression, social withdrawal) and externalizing symptoms (e.g., hyperactivity and aggressive behavior) and overall adjustment problems and lower self-concept or self-esteem than healthy children [3]. A review that integrated 569 studies that administered the Child Behavior Checklist, Youth Self Report, and Teacher Report Form for children and adolescents with chronic physical illnesses found higher elevations in internalizing problems (withdrawn, somatic complaints, anxious/depressed), externalizing problems (delinquent and aggressive), and total behavior problems than their healthy peers [4].
Pediatric chronic kidney disease (CKD) is defined as a reduced glomerular filtration rate (<60 mL/min/1.73 m2) for at least 3 months or the presence of structural or functional kidney damage (even if the value is greater than 60 mL/min/1.73 m2) [5]. The global prevalence of CKD is difficult to assess, as children are frequently diagnosed late, especially in low-resource areas. The prevalence of CKD is 15–74.7 cases per one million children [6]. However, as CKD is often asymptomatic in the earlier stages, it is often underreported or undiagnosed, suggesting an even higher prevalence in children [7].
The etiology of CKD in children varies with age. Congenital anomalies of the kidneys and urinary tract (CAKUT) are observed in younger patients. The common causes of CAKUT causing CKD are renal hypodysplasia, bladder outlet obstruction (posterior urethral valves), and polycystic kidney diseases. In children older than 12 years, primary and secondary glomerular diseases are the leading causes of CKD [6,8]. Regardless of etiology, CKD is associated with progressive loss of kidney function and multiple comorbidities, such as anemia, bone mineral disease, hypertension, cardiovascular disease, and electrolyte/acid-based abnormalities, similar to adult CKD patients. In addition, children experience significant growth failure depending on the age, cause, and onset of CKD [9]. Those with abnormal lower urinary tracts also require multiple surgeries and interventions to empty the bladder, such as clear intermittent catheterization.
If CKD progresses to kidney failure, children require maintenance dialysis until they receive a kidney transplant. Hemodialysis is typically performed thrice weekly at a dialysis facility via a catheter or an arteriovenous fistula. Peritoneal dialysis is performed at home daily using an automated cycler machine or manually by a caregiver. Children undergoing dialysis have multiple dietary restrictions.
Given the extent of the comorbidities of pediatric CKD and the challenges of lifelong treatment, the following unique psychological and social problems may occur.
Psychological and social problems in children and families with CKD
With modern medical advances, such as dialysis and kidney transplantation, the survival of children and young people with CKD has noticeably increased [10,11]. While long-term survival improves among children with CKD, their overall quality of life remains hampered and often continues in adulthood [12-14]. The prolonged need to take medications, frequent contact with medical professionals, and interruptions in schooling and everyday activities may be mechanisms through which the illness increases affected children’s psychological problems [15]. Caregivers often experience emotional, marital, social, and financial burdens, which may leave families feeling unable to deliver the complex care that children with CKD require [16,17]. Moreover, studies of siblings with other chronic conditions revealed that siblings also experience various feelings and reactions, such as sadness, anxiety, stress, or guilt over their good health [18,19]. Some of the problems commonly associated with CKD are summarized in Table 1 [20-34].
Nonetheless, given the condition’s effects on this vulnerable patient population’s physical and emotional well-being, steps must be taken to provide intensive and ongoing psychological support for children with CKD and their families.
Conceptual framework
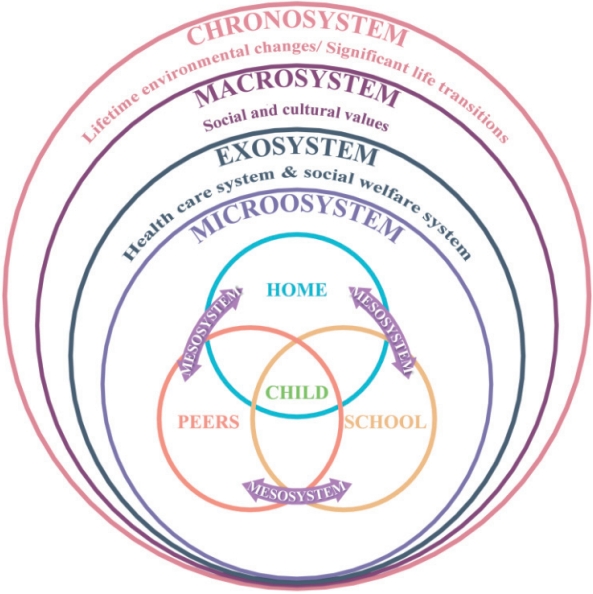
It is essential to understand and examine the various factors that influence the lives of children with chronic illnesses. Theoretical approaches aid in the identification and understanding of the associated psychological risks and guide clinicians in decision-making and planning psychosocial interventions [35]. Bronfenbrenner’s ecological model has been central in guiding the understanding of risk and resilience as development unfolds and supports a contextualized view of child development and treatment (Fig. 1) [36]. It also provides insight into working with children who have a chronic medical illness and their families and the influence of multiple systems, such as the extended family, school, neighborhood health care system, and community, on the child’s interactions and development. This model ensures that a clinician examines the subsystems of the child’s world that play prominent roles in their adjustment and outcomes [37].
Need for psychosocial evaluation
Routine psychological evaluations should be integrated to ensure better understanding of the illness and the child’s overall quality of life. It helps establish a therapeutic alliance with the child and family and provides an opportunity for the parent or family to reflect upon and work through their difficulties [38]. Psychosocial issues reported by the child and parents, or elicited by the clinician, help determine the key areas to be addressed, and the information obtained must be shared across professionals involved in caring for the child and family [38,39]. During an evaluation, if problems such as anxiety, withdrawn behavior, low self-esteem, school refusal, attention deficit, poor scholastic performance, or poor treatment adherence are perceived or reported, the primary physician can refer the child to a mental health professional or a medical social worker for further evaluation. Thus, it ensures early identification and intervention, which lead to better outcomes. Clinicians must also pay attention to the well-being of the siblings, as they are likely to be at risk of adjustment problems. In addition, acknowledging the burden and providing emotional support to the parents or caregivers will help reduce stress.
Psychosocial management
Interventions with children are based on various frameworks, such as cognitive-behavioral, art, storytelling, workbooks, games, music, and play, which decrease distress, anxiety, and pain and enhance adjustment [52-56]. Furthermore, a child’s age, developmental level, and cognitive ability should be considered in planning interventions to allow their families to understand and prepare. VanLeeuwen and Mathews highlighted the need for psychological preparation, mental health consultation, therapeutic intervention, and continuous counseling to prevent unnecessary psychological stress in a pediatric dialysis program [57]. Warady and Chadha [58] reported that therapeutic camps organized for children with kidney failure were successful, indicating reduced depression, improved self-esteem and selfconfidence, and overall promotion of emotional maturity. Meade et al. explored the development and implementation of a self-management program designed to address noncompliance in adolescents with kidney failure on renal replacement therapy [59]. They found that the program effectively created a supportive environment for patients and their parents and addressed healthrelated concerns. Hashim et al. [60] described a dialectical behavior therapy adaptation to improve adherence in adolescent patients with kidney failure. Families also require intervention to help them cope with the stress while providing care. Some aspects of psychological management are shown in Table 3.
Conclusion
Despite medical advances, CKD can take a toll on a child’s social and emotional functioning. Primary care physicians must become proficient at recognizing psychosocial issues, assume a more supportive role, and collaborate with families to address these issues. Awareness and understanding of the child’s condition will improve medication adherence. In addition, screening and monitoring psychological status and referrals for mental health services will enable comprehensive treatment. The best care for children with CKD in addition to medication should involve identifying and managing psychosocial factors, which will facilitate a successful transition to adult life.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


