




Graphical abstract.
Introduction
Although the mortality of very low birth weight infants (VLBWIs) with birth weights less than 1,500 g has decreased, they remain at an increased risk of mortality, and their mortality rates increase with decreasing gestational age (GA) and birth weight [1-4]. Mortality is lower in very preterm infants at centers with larger delivery units or high-level neonatal intensive care units (NICUs) [5,6]. However,the quantitative and qualitative aspects of medical care can impact patient safety and outcomes [7,8]. The quality of medical care is evaluated based on three indicators: structures, processes, and outcomes [9]. Structures refer to the available facilities, equipment, services, and medical personnel, among other things. In the NICU, structures may include the number of nurses and neonatologists (or pediatricians), the number of infants per area, the number of ventilators, the immediate availability of imaging equipment, and the number of personnel capable of neonatal resuscitation.
In Korea, the proportion of preterm infants born at less than 37 weeks of GA and low birth weight infants (less than 2,500 g) has increased from 2.5% and 3.0% of all births in 1995 to 8.5% and 6.8% in 2020, respectively [10-12]. As the number of high-risk infants has risen in a country with very low fertility rates, the quality of medical care in NICU has become increasingly important [13]. Since 2008, the Regional NICU Support Project has increased NICU beds and improved facilities in Korea [14]. The number of NICU beds and NICU beds per 1,000 births has increased from 1,348 and 2.9 in 2010 to 1,751 and 5.4 in 2018, respectively, despite the recent decreasing trend in the number of births [15-17].
While the number of NICU beds in Korea seems adequate [18], addressing the shortage of NICU personnel, regional imbalances in medical supply, and inefficient medical delivery systems is imperative [13,16]. Enhancing survival and prognosis of VLBWIs requires sufficient certified neonatologists or pediatricians in NICU, as they provide stability during the critical postnatal period, including essential neonatal resuscitation. The NICU should have enough staff to provide round-the-clock care for high-risk infants. This study investigates how NICU medical personnel affect VLBWI mortality rates, aiming to inform future NICU grading and medical policy development.
Methods
1. Study design and data collection
Data were prospectively collected from 69 NICUs registered in the Korean Neonatal Network (KNN). The KNN is a nationwide, multicenter, prospective, web-based cohort registry system for VLBWIs with a birth weight <1,500 g, and it includes >70% of VLBW infants in South Korea. The study focused on VLBWIs born between January 1, 2015, and December 31, 2016. In this study, the exclusion criteria are limited to infants who died due to congenital anomalies, enabling a focused examination of how neonatal intensive care quality and prematurity influence mortality rates. 'NICU capacity' refers to the total number of operational beds within the NICU, reflecting the facility's ability to accommodate neonatal patients.
2. Data categories and classification
We categorized and analyzed data on various aspects, including maternal characteristics (e.g., age, education level, health status, complications during pregnancy), and perinatal characteristics (e.g., GA, birth weight, Apgar score), neonatal mortalities, outcomes at discharge, hospital type, NICU bed count, staffing (number of neonatologists and pediatricians), and available treatments and facilities (e.g., dialysis, therapeutic hypothermia, extracorporeal membrane oxygenation [ECMO]). We categorized cities or provinces into 3 segments based on the mortality rates of VLBWIs identified in our study. This categorization aimed to ensure anonymity and address sensitivity issues. Category A includes regions with the lowest VLBWI mortality rates, category B represents regions with moderate VLBWI mortality rates, and category C comprises regions with the highest VLBWI mortality rates. Nurse staffing was graded based on the NICU bed-to-nurse ratio, with categories ranging from grade 1 (<1.0)to grade 4 (Ōēź2.0). Neonatologists and neonatal fellows were included in the pediatrician count, and NICU beds per pediatrician were classified as 'low' (Ōēż10), 'moderate' (11ŌĆō15), or 'high' (Ōēź16). NICU levels, from I to IV, were differentiated by the complexity of available care, from basic to comprehensive services including all types of surgeries and advanced treatments like ECMO. Level I NICUs provide basic care for healthy newborns and stabilize ill newborns before transfer. Level II NICUs offer specialized care for moderately ill infants. Level III NICUs provide comprehensive care for very ill or premature infants, including advanced respiratory suppor t. Level IV NICUs are regional centers that provide the highest level of care, including complex surgeries and treatments such as ECMO. Categorizing NICUs by their capacity into 'small'(Ōēż19 beds), 'medium'(20ŌĆō39 beds), or 'large'(Ōēź40 beds) provided a framework for analysis.
In this study, we divided NICUs registered in the KNN 2 groups based on their performance. After ranking all NICUs according to their mortality rates, the 1st and 2nd quartiles were designated as high-performance NICUs, while the 3rd and 4th quartiles were designated as low-performance NICUs. This classification formed the basis for our analysis, allowing us to compare medical resources, staffing, and outcomes between these 2 groups of NICUs.
3. Ethical considerations and data access
The data registry was approved by the Institutional Review Board (IRB) of Samsung Medical Center (2013-03-002) and the IRBs of all 69 hospitals participating in the KNN. Written consent was obtained from the parents of infants during enrollment in the KNN. Data availability was subjected to the Act on Bioethics and Safety (Law No. 1518, article 18 [Provision of Personal Information]). Contact for sharing the data or accessing the data can be possible only through the data committee of KNN (http://knn.or.kr) and after permitted by the Centers for Disease Control and Prevention of Korea. This study was approved by the KNN data management committee and the Konyang University Hospital IRB (IRB No. 2018-05-012) and data were accessed July 13, 2018.
4. Data analysis
Demographic characteristics and clinical outcomes were compared using independent sample t tests for continuous variables and chi-square tests for categorical variables. The study assessed morbidity and mortality rates across groups with chi-square tests and further analyzed NICU performance against variables such as medical resources, staffing, and regional differences using the same statistical method. Multivariate logistic regression was conducted to identify significant predictors of NICU outcomes, adjusting for confounders and presenting the results as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). Prior to regression modeling, Spearman correlation analysis determined that GA, birth weight, NICU capacity, and staffing were highly correlated (r>0.6), necessitating the exclusion of certain variables to mitigate multicollinearity. Statistical significance was set at a P value of <0.05 for all tests, and the analyses were performed using STATA 12.1 (StataCorp., College Station, TX, USA).
Results
From January 2015 to December 2016, the KNN registered 4,765 VLBWIs. After removing 20 cases due to congenital malformation fatalities, the study focused on 4,745 infants. Within the NICUs evaluated, 2,717 received care in high-performance units, while 2,028 were in low-performance units. Out of the studied cohort, 4,067 infants (85.7%) were discharged alive, whereas 678 (14.3%) did not survive their NICU admission.
1. Demographic and perinatal characteristics in high vs. low performance NICUs
In our study, the demographic characteristics of VLBWIs treated in NICUs were as follows: the mean GA was 28.4 weeks, the mean birth weight was 1,088 g, and 55.4% were male. Additionally, 23.5% of the infants were small for GA, and 36.1% were part of multiple gestations. VLBWIs were grouped according to the performance quartile of their NICUs. Infants in the high-performance NICUs presented with higher GAs and birth weights in comparison to those in NICUs with lower performance rankings. However, high-quartile NICUs reported a more frequent occurrence of lower initial pH values (<7.25), increased rates of in vitro fertilization conceptions, and more instances of abnormal amniotic fluid conditions, including oligohydramnios or polyhydramnios. Additionally, it was noted that mothers of infants in high-performance NICUs were less frequently administered antenatal steroids. The data did not show a significant difference in the rates of infants small for GA or sex distribution between the NICUs of different performance levels. Multiple gestation rates and the application of cardiac compressions and epinephrine in the delivery room were similar across the groups (Table 1).
2. Differential outcomes in NICU performance for morbidity and mortality of VLBWIs
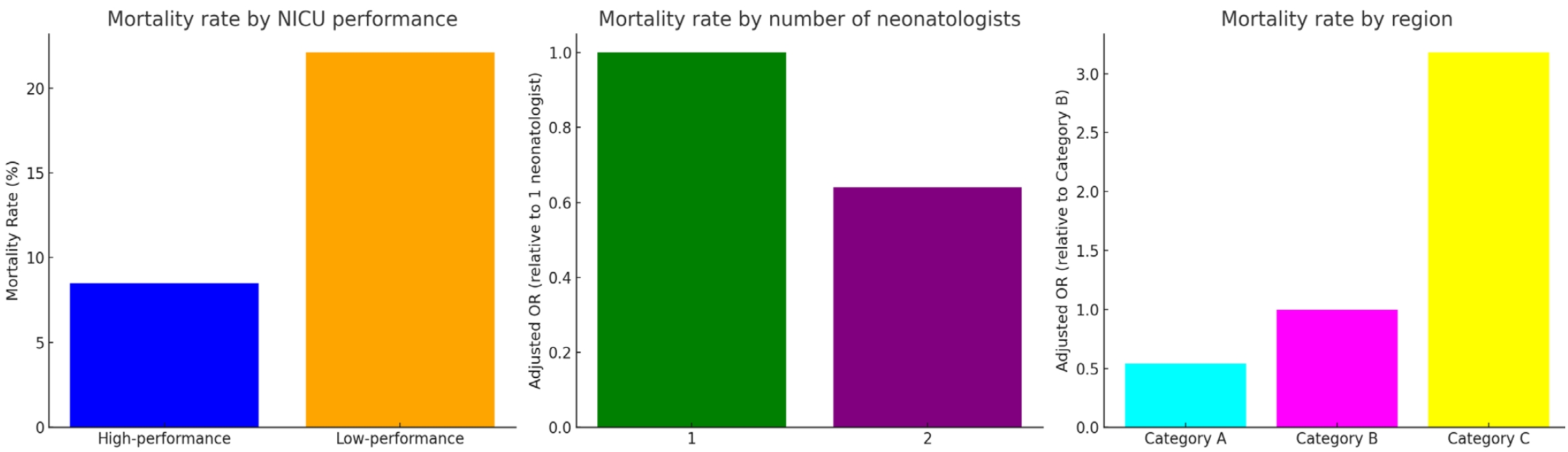
Table 2 delineates the morbidity and mortality rates categorized by NICU performance quartiles. The rates of patent ductus arteriosus treatment, periventricular leukomalacia, bronchopulmonary dysplasia (Ōēźmoderate), and retinopathy of prematurity (Ōēźstage 3 or laser therapy) did not differ significantly between high-performance and low-performance NICUs. Significant differences were noted in the prevalence of sepsis, intraventricular hemorrhage (IVH, Ōēźgrade 3), and necrotizing enterocolitis (NEC, Ōēźstage 2), with low-performance NICUs reporting higher rates of sepsis (23.1%), IVH (11.2%), and NEC (8.3%) compared to 17.7%, 7.3%, and 6.6% respectively in high-performance NICUs. Mortality rates were notably higher in low-performance NICUs at 22.1% compared to 8.5% in high-performance NICUs (P<0.01), with marked disparities across all GA categories. Infants born at Ōēż24 weeks and those within the 25ŌĆō27 weeks category showed significantly higher mortality rates in low-performance units (70.9% and 34.1% respectively) compared to high-performance ones (46.1% and 11.9% respectively).
3. Structural and staffing characteristics of high vs. low performance NICUs
Both high-performance and low-performance NICUs shared similar proportions in tertiary and general hospitals, with each group comprising around 79% of tertiary institutions. High-performance NICUs were more often characterized as 'large' with capacities of 40 or more beds. Additionally, they frequently met a grade 1 nurse staffing level, denoting a favorable nurse-to-bed ratio. With respect to medical professionals, high-performance NICUs employed more neonatologists, especially those with staffing levels of two or more. This was also true for the number of pediatricians, with high-performance units typically having 'low' NICU beds per pediatrician ratios, which suggests a potential for more individualized patient care. Furthermore, high-performance NICUs were correlated with providing higher-level NICU therapy, indicative of more advanced and comprehensive care capabilities. Regionally, high-performance NICUs were more frequently located in areas that recorded lower mortality rates, highlighting a connection between NICU performance and the health outcomes of the surrounding region (Table 3).
4. Influences on mortality outcomes in VLBWIs: overall trends and subgroup focus on <28 weeks GA
The analysis of NICU outcome predictors revealed that neonatologists' presence significantly impacts VLBWI mortality rates, with a lower risk observed in units with two neonatologists compared to those with just one. However, there was no added benefit in having three or more neonatologists. When considering the NICU beds per pediatrician, infants in units with 'moderate'(11ŌĆō15) and 'low'(Ōēż10) ratios experienced a reduced mortality risk relative to those with 'high'(Ōēź16) ratios. In assessing the influence of NICU therapy level, a stepwise increase in mortality risk was seen with decreasing therapy levels. Regional analysis indicated a higher mortality risk in NICUs located in areas with higher overall mortality rates. Furthermore,the study underscores the significance of nursing care quality, as evidenced by the finding that grade 2 nurse staffing is associated with a higher OR of 1.36 for mortality (Table 4).
Subgroup analysis focusing on infants born before 28 weeks of GA not only corroborates the findings from the broader cohort but also provides more granular insight (Table 5). By narrowing the scope to this particularly vulnerable subset, the data underlines the robustness of the associations between NICU staffing, therapy level, and regional disparities with mortality outcomes.
Discussion
The better survival rates in high-performance NICUs are notable, and while initial assumptions may link this to the infants' higher GAs and birth weights, our study's adjustments for these factors reveal a deeper narrative. The data affirm that structural and operational qualities within NICUs are pivotal in patient outcomes, highlighting the essential role of adequate medical staffing and the need for a strategic focus on qualitative improvements in neonatal care. These units show lower instances of severe morbidities and overall mortality, underscoring the critical role that the quality of neonatal care plays in the prognosis of these vulnerable infants. The enhanced outcomes in certain NICUs may also reflect the broader impacts of the nationwide projects, which likely contributed to the upgraded facilities and practices in these units. By emphasizing care quality, Korea can strive to not only meet but exceed international standards in neonatology, ensuring that every infant, regardless of GA or birth weight, has the best possible chance at life [19].
Korea's Regional NICU Support Project (2008) and Integrated Care Center Project for High-Risk Pregnancies and Neonates (2014) have significantly enhanced NICU facilities nationwide [14,20]. Following these improvements, KoreaŌĆÖs infant mortality rate fell from 9.9 (1993) to 2.5 (2020), and VLBWI survival rates rose from 83.0% in the 2000s to 85.7% in the 2010s [21,22]. Despite these gains, KoreaŌĆÖs survival rates still lag behind other developed countries, with recent stagnation in progress [2]. The implications of our study are significant, demonstrating that both the structural dynamics within NICUs and the regional context in which they operate are substantial determinants of mortality among VLBWIs. The staff-to-patient ratio, particularly the number of pediatricians per NICU bed, is strongly associated with survival outcomes, emphasizing the necessity of adequate staffing for providing high-quality, individualized care. Research has established that higher staff-to-patient ratios in NICUs are linked to improved long-term outcomes for preterm infants, including lower risks of severe complications and better developmental progress as they grow [23,24].
Research indicates that hospitals treating many extremely preterm infants and offering advanced NICU care tend to have lower mortality rates [25-27]. The British Association of Perinatal Medicine recommends at least 100 new VLBWI admissions yearly for quality treatment in NICUs [28]. However, the sheer number of admissions alone does not ensure better outcomes. Coordinated obstetric-pediatric care, staff experience, and adherence to clinical guidelines are also crucial. Previous studies suggest that nurse numbers in NICUs correlate with LBWI mortality, impacting care outcomes for moderately preterm infants (30ŌĆō34 weeks of GA) [29,30]. Our study revealed a significant relationship between nurse staffing grades and VLBWI mortality, with higher mortality rates linked to lower staffing grades. We did not evaluate the extent of experience among the medical personnel, which could be a contributing factor to the higher survival rates observed in level IV NICUs. While nurse staffing grading is based on the nurse-to-patient ratio and does not directly measure the staff's experience level, this staffing metric significantly impacts patient care quality and outcomes. The experience level of nursing staff, therefore, remains a potential variable that warrants further investigation, especially given the correlations observed.
A study of the United States population found that regions with a low number of neonatologists (4.3/10,000 births) had lower newborn mortality rates than regions with significantly lower numbers of neonatologists (2.7/10,000 births), especially for newborns with birthweights of 500ŌĆō999 g. However, no further reduction in neonatal mortality was found as the number of neonatologists increased [31]. Our study extends these findings by indicating that while having 2 neonatologists instead of one is associated with a decrease in VLBWI mortality, increasing the number to three or more does not further reduce mortality rates. This underscores the importance of both neonatologists and pediatricians per NICU bed in determining outcomes, rather than focusing on one type of physician alone. In 1985, the American Academy of Pediatrics proposed that the appropriate standard for the number of patients per neonatologist in the NICU should be six, considering the severity, length of hospital stay, and working patterns of neonatologists in NICUs [32,33]. Based on the data published by Thompson et al. [34], which compared population data by country and neonatologist staffing, the number of NICU beds per neonatologist was 8.4 in the United States, 6.9 in Australia, and 8.1 in Canada, all of which were under 10. In Korea, only 50.7% of VLBWIs were admitted to NICUs with a low staffing ratio (Ōēż10 beds per pediatrician), while 17.8% were admitted to units with a high staffing ratio (Ōēź16 beds). Although the cause for this recent change is unknown, the medical staffing conditions of NICUs may have worsened due to the shortage of pediatric medical residents.
Our analysis underscores significant regional differences in mortality rates among VLBWIs, indicating that location plays a crucial role in these disparities. Although our study did not officially categorize NICUs into metropolitan and nonmetropolitan areas, the data suggest pronounced variations in mortality depending on the region. This disparity likely stems from differences in healthcare infrastructure, available resources, and the concentration of tertiary hospitals, which are more prevalent in certain areas. Despite ongoing government efforts to reduce these disparities, our findings emphasize the need for continued research into regional healthcare variations. Addressing these inequalities is essential for policy interventions aimed at ensuring equitable healthcare access across all regions,thus providing every infant the best possible chance of survival [35,36].
This study has various limitations that need to be addressed. First, presenting NICU capacity and bed-to-doctor ratios as interval, not continuous variables, might have influenced the analysis due to interval distribution. Second, although the data for VLBWIs born in 69 centers were analyzed, the information about each center was not available, making it challenging to determine the actual number of analyzed centers after the exclusion. Third, our study did not compare the varying degrees of experience among medical staff, including nurses, neonatologists, and pediatricians, due to the lack of standardized data on their qualifications and experience within the registry, despite this being a critical factor that can significantly impact neonatal outcomes. Fourth, our analysis was limited to a 2-year dataset from a national registry, which is insufficient for drawing robust conclusions. This study was planned in late 2017 and approved in 2018, and the KNN only allows for the distribution of registry data after the year-end verification has been completed. Therefore, further studies, including follow-up data on long-term development and growth outcomes according to medical resources, are necessary.
In conclusion, this study underscores the critical role of NICU staffing and facility characteristics in influencing mortality among VLBWIs. We observed that NICUs with higher staffing levels and those located in regions with more robust healthcare infrastructures demonstrated superior survival rates. These findings highlight the necessity of enhancing NICU staffing and improving the distribution of healthcare resources to ensure equitable care across different regions. Addressing these disparities is crucial for optimizing outcomes in this vulnerable population. Future policies should focus on ensuring the availability of skilled neonatologists and pediatricians across all NICUs to maintain high-quality care standards consistently.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


