




Introduction
Korean Neonatal Network update
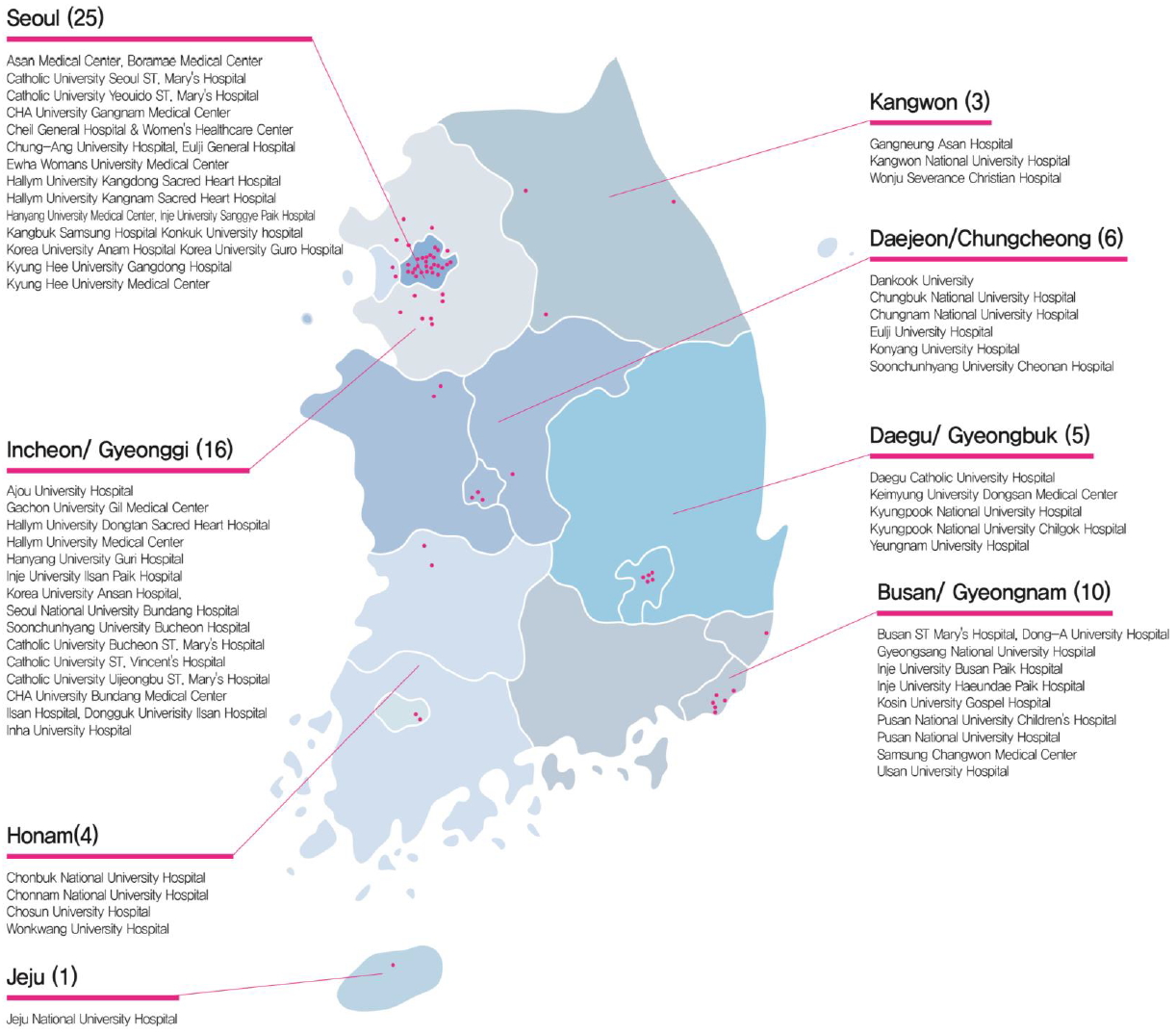 |
Fig. 1.National distribution of 70 neonatal intensive care units participating in the Korean Neonatal Network. Available from: http://www.knn.or.kr/index.jsp.
|
Short-term outcomes of VLBWIs in KNN
Table 1.
Values are presented as percentage (range of probability: 95% confidence interval).
There is a significant difference among groups if the probability ranges do not overlap with each other.
Modified from Lee et al. J Korean Med Sci 2019;34:e40 [10].
![]()
Table 2.
Values are presented as percentage (range of probability: 95% confidence interval).
There is a significant difference among groups if the probability ranges do not overlap with each other.
Modified from Lee et al. J Korean Med Sci 2019;34:e40 [10].
![]()
Long-term outcomes of VLBWIs at the corrected 18–24 months age in KNN
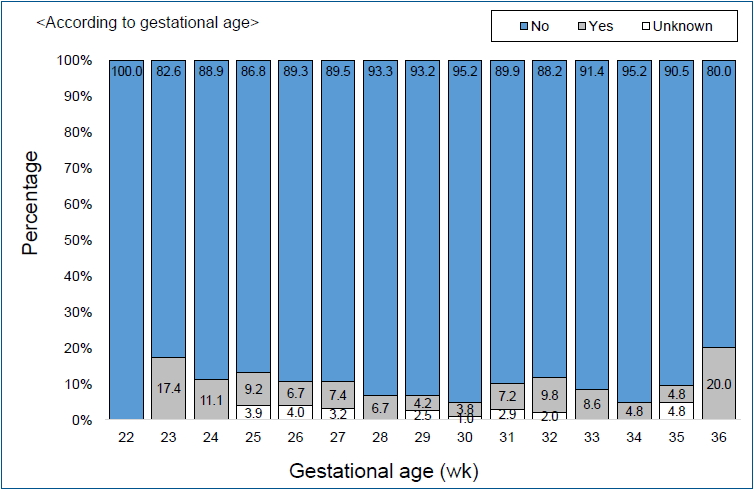 |
Fig. 2.Cerebral palsy cases by gestational age among very low birth weight infants born in 2013. Adapted from the Executive Committee of Korean Neonatal Network. 2013 Korean Neonatal Network Annual Report: Korean Centers for Disease Control and Prevention, 2014 [19].
|
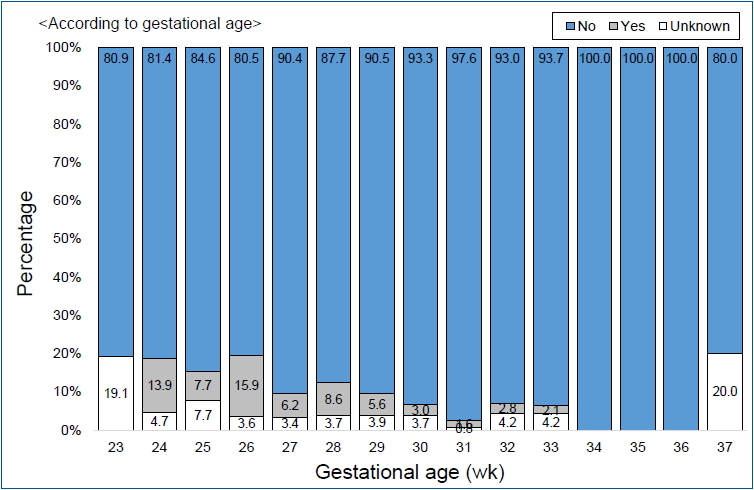 |
Fig. 3.Cerebral palsy cases by gestational age among very low birth weight infants born in 2014. Adapted from the Executive Committee of Korean Neonatal Network. 2014 Korean Neonatal Network Annual Report: Korean Centers for Disease Control and Prevention, 2015 [20].
|
Table 3.
| Variable | 2013 (n=1,000) | 2014 (n=1,660) |
|---|---|---|
| Gestational age (wk) | 291/7±26/7 | 292/7±26/7 |
| Birth weight (g) | 1,093±268 | 1,125±261 |
| Male | 504 (50.4) | 833 (50.2) |
| Post-discharge mortality | 15 (1.5) | 20 (1.2) |
|  Respiratory | 5 (45.5) | 6 (35.3) |
|  Underlying disease | 11 (73.3) | 17 (85.0) |
| Growth at visit | ||
|  Weight | n=800 | n=1,091 |
|   <50th | 465 (46.5) | 721 (66.1) |
|   50th–90th | 243 (30.4) | 337 (30.9) |
|  Height | n=753 | n=993 |
|   <50th | 482 (64.0) | 622 (62.6) |
|   50th–90th | 219 (29.1) | 325 (32.7) |
|  Head circumference | n=632 | n=811 |
|   <50th | 404 (64.0) | 516 (63.6) |
|   50th–90th | 176 (27.8) | 267 (32.9) |
| Rehospitalizationsa) | n=846 | n=1,182 |
|  Respiratory | 262 (44.9) | 349 (47.5) |
|  Surgery | 135 (23.2) | 168 (22.8) |
|  Infection | 106 (18.2) | 106 (14.4) |
| Medical treatmenta) | n=846 | n=1,182 |
|  Oxygen | 142 (16.8) | 166 (14.0) |
|  Ventilator | 53 (6.3) | 60 (5.1) |
|  Nasogastric tube feeding | 76 (9.0) | 100 (8.5) |
| Cerebral palsy | n=846 | n=1,182 |
|  Diplegia | 28 (3.3) | 46 (3.9) |
|  Hemiplegia | 4 (0.5) | 7 (0.6) |
|  Quadriplegia | 24 (2.8) | 20 (1.7) |
|  Unknown | 21 (2.5) | 47 (4.0) |
| Rehabilitative support | ||
|  No | 512 (60.5) | 748 (63.2) |
|  Yes | 318 (37.6) | 412 (34.9) |
| Language support | ||
|  No | 779 (92.1) | 1081 (91.5) |
|  Yes | 43 (5.1) | 68 (5.7) |
| Eye and hearing | n=846 | n=1,182 |
| Blindness | n=846 | n=1,134 |
|  One-eye | 4 (0.5) | 3 (0.3) |
|  Both eyes | 2 (0.2) | 3 (0.3) |
| Ophthalmologic disordersa) | 120 (14.2) | 179 (15.1) |
|  Retinopathy of prematurity | 56 (41.2) | 51 (26.6) |
|  Glaucoma | 0 | 3 (1.6) |
|  Cataract | 2 (1.5) | 1 (0.5) |
|  Strabismus | 29 (21.3) | 40 (20.8) |
|  Refraction abnormality | 15 (11.0) | 11 (5.7) |
|  Wearing glasses | 23 (2.7) | 19 (1.6) |
| Hearing impairmenta) | 24 (3.2) | 22 (1.9) |
|  Unilateral | 10 (1.3) | 12 (1.0) |
|  Bilateral | 14 (1.9) | 10 (0.8) |
|  Hearing aid | 6 (0.7) | 3 (0.3) |
|  Need for cochlear impairment | 1 (0.1) | 4 (0.3) |
Modified from Youn et al. J Korean Med Sci 2018;33:e309 [21].
![]()
Table 4.
Values are presented as number (%).
VLBWI, very low birth weight infant; BSID, Bayley Scales of Infant Development; MDI, Mental Developmental Index; PDI, Psychomotor Developmental Index.
Modified from Youn et al. J Korean Med Sci 2018;33:e309 [21].
![]()
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


