

Introduction
Dengue is an acute influenza-like disease caused by mosquito-borne arboviruses of the family Flaviviridae, with four different serotypes: DEN-1, DEN-2, DEN-3 and DEN-41, 2). Dengue viruses are maintained in cycles of human-mosquito-human transmission, the major vector is Aedes aegypti, and recently Aedes albopictus is found as a less-efficient but more adaptable vector1). Dengue is found in tropical and sub-tropical regions around the world, predominantly in urban and semi-urban areas. The incidence of dengue has grown dramatically around the world in recent decades. About 2.5 billion people - 40% of the world's population - are now at risk for dengue. The World Health Organization (WHO) currently estimates that there may be 50 million to 100 million dengue infections world wide every year, with 500,000 hospitalizations and 22,000 deaths, mostly in children3). Dengue is now endemic in more than 100 countries in Africa, the Americas, the Eastern Mediterranean, South-east Asia and the Western Pacific region. The South-east Asia and Western Pacific regions are the most seriously affected with lethal complications such as dengue hemorrhagic fever3). In Korea, 22 cases of pediatric dengue fever from 2001 to 2008 were reported according to the data collected by the Korea Centers for Disease Control and Prevention (KCDC)4). All cases were imported dengue fever5).
Many countries where dengue is endemic are popular tourist destinations and the disease is an increasingly important problem encountered by international travelers. The importance of dengue to pediatric infectious diseases practice has been increasing1, 6-8). This study was performed to estimate international travel experiences of Korean children and to report clinical features of dengue fever.
Methods
Data was collected from all patients who visited the pediatric infectious diseases clinic at Samsung Medical Center from January 2008 to December 2008. All new patients were asked through a questionnaire about their illness and history which included travel and environmental exposure history. Four patients who returned from international travel were suspected of dengue fever. Enzyme-liked immunosorbent assay detecting serum IgM and IgG (Dengue Duo IgM and IgG capture ELISA) was performed according to the manufacturer's protocol (Inverness Medical Innovations Australia Pty Ltd, Sinnamon Park, Queensland, Australia) at the Korea Centers for Disease Control and Prevention (KCDC). Medical records and questionnaires were reviewed.
Results
Five hundred and seventeen patients visited the pediatric infectious diseases clinic at Samsung Medical Center from January 2008 to December 2008. Three hundred and thirty nine patients (65.6%, 339/517) responded to the questionnaire. One hundred and one patients (29.8%, 101/339) had experiences of international travel within 2 years and 26 patients (25.7%, 26/101) had visited more than two countries. The popular destinations were the USA (n=32, 31.7%), China (n=23, 22.8%), Japan (n=21, 20.8%), Singapore (n=10, 9.9%), Thailand (n=8, 7.9%), the Philippines (n=7, 6.9%), and Indonesia (n=7, 6.9%) in order (Fig. 1).
There were 7 patients who had a fever and international travel history within 2 weeks at the time of presentation. Four patients were suspected of dengue fever based on their symptoms, laboratory values and travel history to endemic areas.
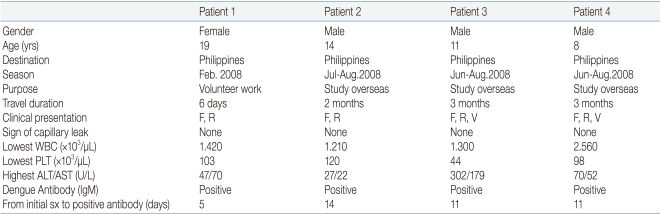
Dengue serological tests were requested and the results were positive in all 4 tested patients. Table 1 shows the clinical and laboratory features of the patients diagnosed with dengue fever. There were one female and three male patients. The range of ages was from 8 to 19 years. All four patients had visited the Philippines. Patient 1 had a past medical history of osteosarcoma which had been completely cured with chemotherapy and a limb salvage operation in 2003. She was presented with a fever and maculopapular skin rash after 3 days of her return. She was initially seen by a hematology-oncology team due to her previous cancer history, fear of cancer recurrence and cytopenia at the time of presentation. However, an infectious diseases team was consulted on this patient and observation with conservative management was recommended since dengue fever was suspected. Patient 2 developed a fever and pin-pointed hemorrhagic rash over his whole body after 5 days of his return. Patient 3 and 4 were brothers who complained of fever, rash and vomiting since the day they returned. The symptoms lasted for one week. Patient 3 and 4 had also visited a hematology-oncology clinic first due to their known history of cytopenia diagnosed at an out-side hospital. They were referred to an infectious diseases clinic for evaluation. All four patients showed mild to moderate leukopenia (median 1,360/mm3) and thrombocytopenia (median 100,500/mm3) and mildly increased serum aminotransferases (median AST/ALT 58.5/61 U/L). However, none of the patients had signs of a capillary leak; elevated hematocrit (20% or more over base line), low albumin, pleural or other effusion. Only one patient was hospitalized (Patient 1) and the other three patients were treated as outpatients. They recovered from the illness with supportive care without significant complications.
Discussion
For the present, there is no report of dengue occurring in Korea5, 9). Six cases of imported dengue were first reported in 20015). As increasing numbers of international travelers visit dengue endemic areas, the incidence of imported dengue has increased. Choi et al9) reported the characteristics of 17 adult cases with dengue fever by collecting domestic literature from Korean bibliographic databases. Park et al10) reported the case of a 15 year-old male with dengue fever complicated by rhabdomyolysis. This is the first report that prospectively estimated international travel experiences and dengue fever in Korean children who visited a pediatric infectious diseases clinic at a university hospital.
Dengue fever is a reportable infectious disease (group 4) in Korea. The KCDC reported 169 cases of dengue from 2003 to 20075). The destinations of imported dengue patients were mostly Asian countries except in one case where the patient was infected in Brazil. The most common destination where Korean travelers were infected with dengue was the Philippines (36.7%, 62/169). Among 169 cases, 13 cases (7.7%, 13/169) occurred under 20 years of age. Of note, we diagnosed 4 pediatric dengue cases in 2008 in our clinic.
The data from the Korea national statistical office showed that 13.33 million people accounting for 22.3 percent of the total population traveled abroad and 11.3 percent of all primary school students had international travel experiences in 200711). In this study, about one third of children who visited the pediatric infectious diseases clinic (29.8%) had international travel experience during the 12 months of the survey period from January 2008 to December 2008. Although the patients who visited our clinic may not represent all Korean children in a general population considering the socioeconomic differences among cities and provinces, this study still shows that Korean children are at risk of acquiring dengue fever from travel abroad and Korean pediatricians should be more prepared for such patients. Although small in numbers, this study is the first report to describe the clinical features of dengue fever in Korean children.
Dengue may present symptoms 3-14 days (usually 4-7 days) after exposure to the virus and the infection may range from subclinical to fever, retro-orbital headache, arthralgia and sometimes a quite florid maculo-papular rash usually within 3-5 days following the onset of the fever3). Patients with dengue fever sometimes may have hemorrhagic manifestations. Laboratory findings commonly include thrombocytopenia, leukopenia with lymphopenia, mild to moderate elevations of hepatic aminotransferases and lactate dehydrogenase, and hyponatremia2). The capillary leak results in dengue hemorrhagic fever and in its severe or fatal form dengue shock syndrome, which are complications defined by the WHO6, 12, 13). Although infection with one serotype confers life-long protection against that serotype, reinfection with another serotype of dengue virus may predispose a person to the development of dengue hemorrhagic fever or dengue shock syndrome which have more serious outcomes2). Therefore those who have suffered from dengue fever previously should be more careful when traveling to endemic areas.
The spread of dengue is attributed to expanding geographic distribution of the four dengue viruses and their mosquito vectors, A. aegypti and A. albopictus14, 15). Of note, although Korea is not a dengue endemic country, the A. albopictus ("Asian tiger mosquito") mosquitoes have been discovered throughout Korea5, 9). These mosquitoes are well adapted to life in urban settings2). Global air travel has allowed introduction and cocirculation of different serotypes of the virus in new regions. Consequently, dengue has developed into a disease of pandemic proportions16). Although A. albopictus is native to tropical and subtropical regions, they are successfully adapting to cooler regions and have been expanding globally at an alarming rate6, 17-19). Having vectors capable of transmitting dengue in Korea has a very important implication on the nation's dengue surveillance since there is the possibility for a domestic dengue case by the Aedes albopictus mosquito in the future5, 18).
Many countries where dengue is endemic are popular tourist destinations and the disease is an increasingly serious problem encountered by international travelers. Many Korean children visit dengue endemic areas, may return home with dengue fever and there are no vaccines or drugs against dengue yet.
Dengue fever is not a familiar disease to Korean pediatricians which makes its diagnosis harder. Fever in the returned traveler can be a manifestation of a minor, self-limited process or can develop into a progressive and life-threatening illness. The clinician's lack of familiarity with the types of infections that the patient may have encountered while traveling is often an obstacle for the assessment of these patients. A systematic approach to the evaluation of febrile patients should include basic information about the geographic distribution of infectious diseases in the locations where the person has lived and traveled20, 21).
In conclusion, dengue fever should be suspected in Korean children who have a travel history to endemic areas and febrile illness.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


