


Introduction
Kawasaki disease (KD) is an acute, self-limiting febrile illness of unknown cause that affects the coronary arteries, predominantly occurring in children aged ≤5 years. KD was first described by Kawasaki in 19671) and is now known as the most common cause of acquired heart disease in children in developed countries2). The appropriate initiation of treatment with intravenous immunoglobulin reduces the incidence of coronary artery aneurysms from 25% to 4%3,4,5,6).
A quantitative assessment of the dimensions of the coronary artery using echocardiography is an important practice in the management of patients with KD. The criteria for coronary artery aneurysm, set by the Japanese Ministry of Health and Welfare in 1984, was a maximum internal diameter of ≥3 mm in children aged <5 years and ≥4 mm in children aged ≥5 years, a segment 1.5 times greater than the adjacent segment, and the presence of luminal irregularity7). Until recently, these criteria were widely used as they were easy to memorize and use. However, an underestimation of the incidence of coronary arterial lesions and an inability to reflect children's body growth in the application of these criteria have been pointed out8). A standardized score (z score) for assessing cardiovascular structures has been developed for use in pediatric clinical environments as children undergo rapid changes in their physical development with resultant variations in their body size9). Several coronary artery z score models have been subsequently proposed8,10,11,12,13,14,15); a relatively large number of subjects was included, and nonlinear regression methods were adopted in four of models12,13,14,15). In a recently published practice guideline by the American Heart Association, the classification of coronary arterial lesions is based on the z score of coronary artery diameter2). The previously reported z score model for Korean children has two major limitations: firstly, the number of subjects included in the study for the model was too small and secondly, a linear regression was adopted for model fitting of the body surface area16). The z score model by Kobayashi et al.15), which was derived from the lambda-mu-sigma method in 3,851 Japanese children, holds promise for use in Korean children due to its large sample size and the racial similarity between the Japanese and Korean populations.
In this study, an investigation of the statistical properties of 4 previously developed pediatric coronary artery z score models, including the Japanese model, was performed in relation to 181 healthy Korean children. We expected the results of this investigation to present useful information on the selection of z score models in clinical practice in Korea.
Materials and methods
1. Subjects
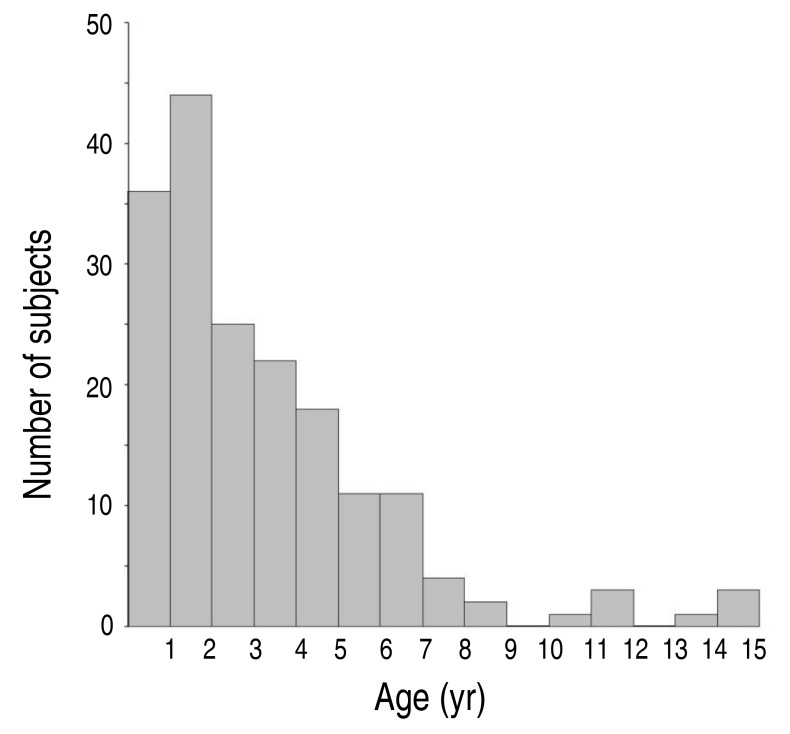
The study subjects were 181 healthy Korean children, whose ages ranged from one month to 15 years (Fig. 1), and who presented at the Asan Medical Center for an evaluation of a cardiac murmur, abnormal findings on chest radiography (e.g., borderline heart size), syncope, or transient chest pain. Echocardiographic studies showed no significant anatomical and functional abnormalities in the subjects. The subjects' demographic characteristics were evaluated through a review of their medical records. A body surface area was estimated using the Haycock formula17).
This study was approved by the Institutional Review Board of Asan Medical Center (2017-0853), and the requirement for informed patient consent was waived.
2. Echocardiography and coronary measurements
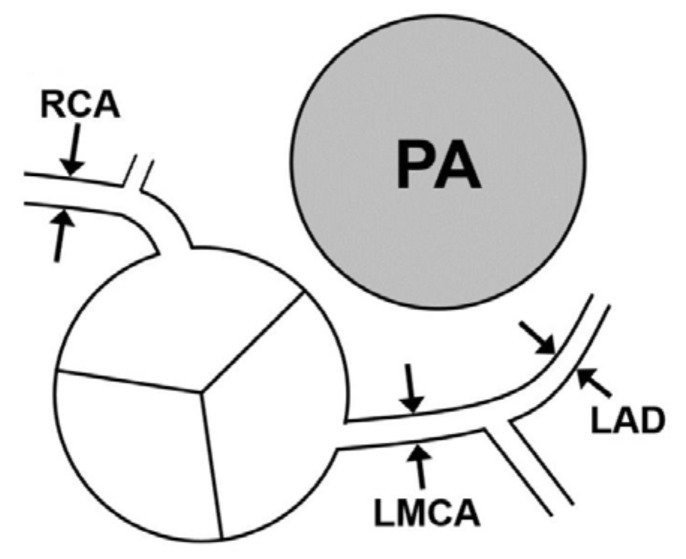
The standard method of measuring the diameter of coronary arteries in a pediatric population was applied according to the recommendation by the American Society of Echocardiography18). The intraluminal diameter of the coronary artery segments was measured from the inner to inner edges. The left main coronary artery (LMCA) was measured midway between the ostium and the bifurcation of the circumflex artery and the left anterior descending coronary artery (LAD) in the parasternal short-axis view. The LAD was measured distally to the bifurcation and before the start of the first marginal branch. A measurement for the right coronary artery (RCA) was obtained in the relatively straight section, just after the initial rightward turn from the anterior-facing sinus of the Valsalva. In a case with a visible origination of the conal branch, the RCA segment distal to the conal branch was measured (Fig. 2). The offline measurement of coronary artery diameters was performed by one author (JJY). The reproducibility of coronary artery diameter measurements has already been reported in another study which was performed by same echocardiographers19) (an intraobserver variability in the measurement of the LMCA, LAD, and RCA as 5.4%, 8.7%, and 5.1%, respectively, and the interobserver variability as 5.8 %, 10.4%, and 7.0%, respectively).
3. Statistical analysis
The diameters of each coronary artery were measured and converted to the z score using the previously reported regression equations or spreadsheet file for calculation12,13,14,15). The results of the z score of coronary artery diameter were analyzed using the Kolmogorov-Smirnov test on a normal distribution and using the 1-sample t test on a convergence of the average value to zero. Statistical analysis was performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Statistical significance was defined as P<0.05.
Results
One hundred eighty-one children were included in the study, 47% of whom were male (Table 1). The age of subjects was median 2.34 years (range, 1 month to 15 years; Fig. 1). The weight of the subjects was median 12.6 kg (range, 2.9–73.9 kg) and the height was median 89.0 cm (range, 48.7–176.6 cm). The body surface area was median 0.559 cm2 (range, 0.201–1.909 cm2). The median diameter of LMCA, LAD, and RCA was 2.13 mm (range, 1.35–4.01 mm), 1.65 mm (range, 1.10–3.26 mm), and 1.60 mm (range, 0.82–3.65 mm), respectively (Table 1).
1. The descriptive statistical properties of z score value
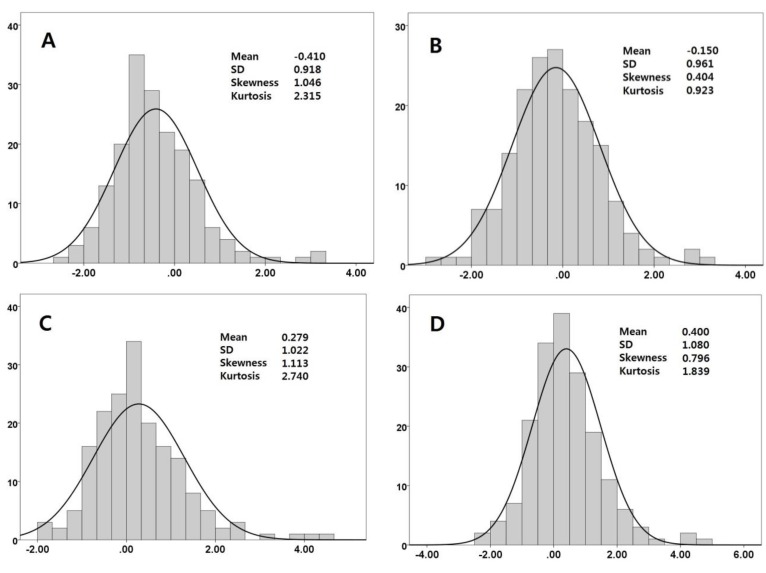
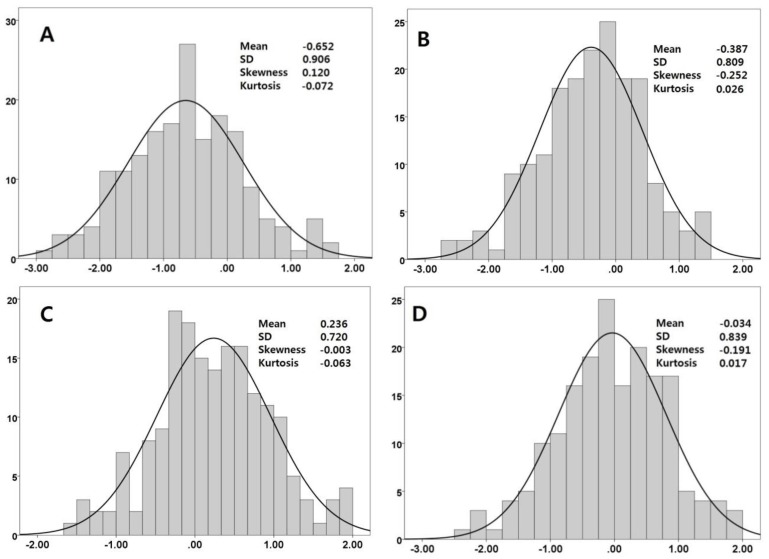
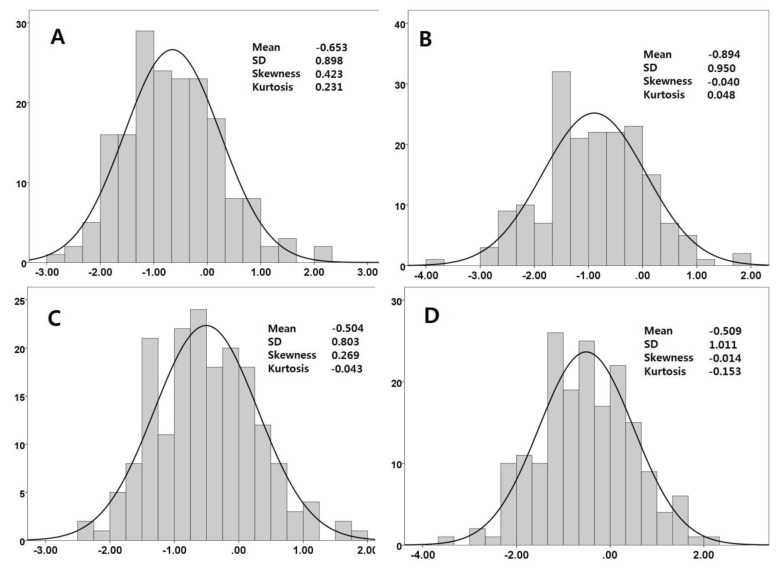
By definition, the z score values must be normally distributed and the mean value should converge to zero, the standard deviation to 1, the skewness to zero, and the kurtosis to zero. The descriptive statistical characteristics of the z score value is presented in Table 2 and plotted as a histogram in Fig. 3, 4, 5. The mean value of the z score of the RCA was less than zero in all 4 models. The values of skewness and kurtosis of the LMCA were above zero in all models. The P value on the Kolmogorov-Smirnov test for the z score value was ≥0.050 in three coronary arteries in all four models, which suggests the statistical feasibility of normal distribution. One sample t test showed that the mean z score value was significantly different from zero (Table 3); the only exception was a z score of the LAD in the Japanese model (P=0.582).
2. The proportion of z scores with extreme value
The percentage of subjects with a z score of the LMCA ≥2.0 in the Dallaire and Japanese models appears higher (4.9% and 7.1%, respectively) than 2.3% which is the proportion of the z score ≥2.0 in standard normal distribution (Table 4). Moreover, the percentage of the z score of the LMCA ≥2.5 also appears higher (3.3% and 3.8%, respectively) than 0.6% which is the proportion of the z score ≥2.5 in standard normal distribution in those 2 models. The extremely high z score of the LMCA seems to be more frequent in the Dallaire and Japanese models than in the other 2 models.
Discussion
In this study, the descriptive statistical analyses of coronary artery diameter z scores in 181 normal children were performed using four frequently used z score models (Table 5)12,13,14,15). As all models are designed to represent a normal population, we expected that the calculated z scores for healthy children would also follow a normal distribution. The Kolmogorov-Smirnov test showed P≥0.050 in three coronary arteries in all 4 models, implying the statistical feasibility of normal distribution. Therefore, it was consequently estimated that the four z score models would be distributed normally, which justifies the application of these models to Korean pediatric populations.
We additionally expected that the mean value of the z score should converge to zero since the subjects were normal healthy children. However, the mean z score value of the 3 coronary arteries was significantly different from zero in each of the four models, except for one of the LADs in the Japanese model. The limited number of subjects in this study could be one of causes. Another explanation for this difference could be the subtle differences in the measuring points. In this study, the mean z score of the RCA was consistently less than zero in all models, which implies that the measured RCA diameters were smaller than the reference values of the z score models. It is reported in the z score model reference papers that the RCA measurements were obtained 2–5 mm distal to its origin in the parasternal short-axis view13,14,15). In this study, the RCA segment distal to the conal branch was measured in a case with a visible origination of the conal branch to avoid an exaggerated measurement on the branching point. In addition, the measurement point was more distal to 5 mm from the origin of the RCA in some of such cases. As a result, the RCA diameters in this study would have been smaller accordingly. We think that more precise instructions are needed for an accurate and reproducible measurement of the RCA proximal diameter on the issue of the conal branch.
Among the four z score models, the Dallaire and Japanese models were more favorably recommended for use in recent American Heart Association guidelines because they included a relatively larger number of subjects and provide normative data on the left circumflex branch2). Incidentally, the percentage of subjects with an extreme z score of the LMCA appears to be higher in the Dallaire and Japanese models in this study than the expected level under normal distribution. This higher percentage could be due to anatomic variation in several cases, which can be seen in the histograms for the LMCA (Fig. 3). The positive skewness and kurtosis in the distribution of the LMCA z score would not impact on the higher percentage of subjects with extreme z scores of the LMCA. It is well known that anatomic variations are frequent in the LMCA2). Additionally, caution in the interpretation of the LMCA z score was also recommended in recent guideline2). For the other branches of coronary arteries, all four z score models could reasonably be used for the evaluation of vascular dilatation.
The relatively small number of subjects is a limitation of this study.
In conclusion, all 4 models showed statistical feasibility of normal distribution. More precise instructions are needed for RCA measurement. A higher percentage of extreme z scores of the LMCA is compatible with a commonsense understanding of anatomic variations of the LMCA.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


