




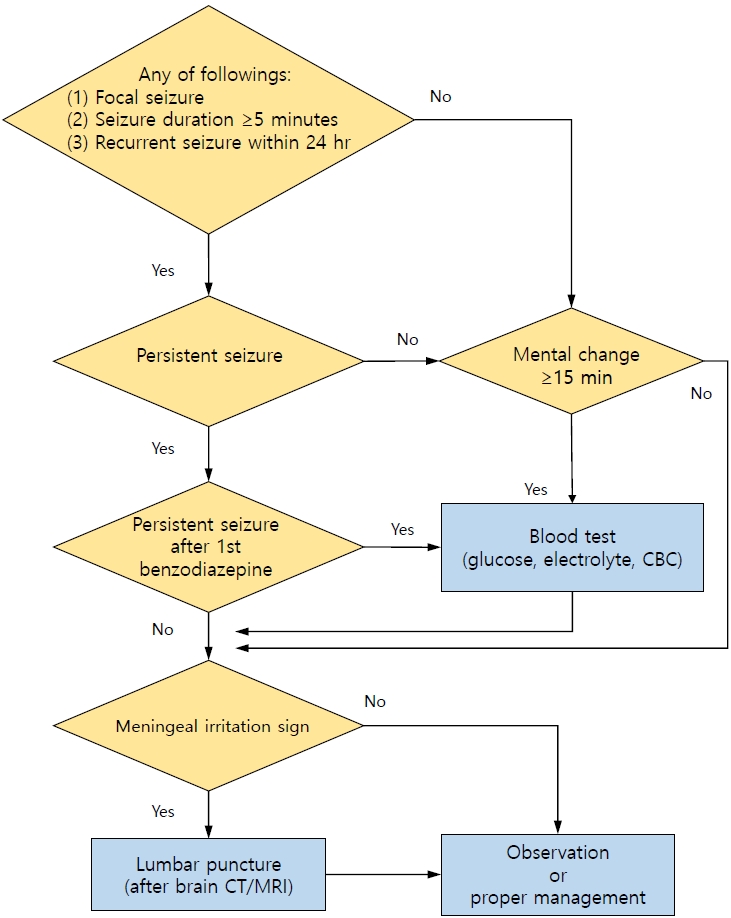
Graphical abstract.Flow chart for examining a child with a febrile seizure who visits the emergency room. This flow chart is based on the guidelines of the American Academy of Pediatrics[1] and Japanese Society of Child Neurology.[6] CBC, complete blood count; CT, computed tomography; MRI, magnetic resonance imaging.
Febrile seizures, which occur in children aged 6–60 months without a central nervous system (CNS) infection, are accompanied by fever (≥38 °C/100.4 °F) [1]. Febrile seizures are the most common type of pediatric seizures. Byeon et al. [2] recently reported a 6.9% prevalence and 6.5% incidence of febrile seizures among Korean children under 5 years of age. This incidence is higher than that in Europe and the United States (2%–5%) but slightly lower than that in Japan (7%–10%) [3]. An episode is classified as a complex febrile seizure if any of the following conditions are met: (1) focal seizure, (2) prolonged duration (≥15 minutes), or (3) recurrent seizure within 24 hours [1]. Otherwise, cases are classified as simple febrile seizure (SFS) [1].
The routine use of lumbar puncture (LP) in cases of SFS has markedly decreased over the past decade [4]. This change accelerated after SFS guidelines was proposed by the American Academy of Pediatrics (AAP) in 2011, and has been consistently supported by other guidelines [1,4-7]. The biggest difference from the previous AAP guidelines is that LP is no longer recommended in cases of infants aged 6–12 months [1,4]. In the absence of signs of a CNS infection, LP is an option for infants of this age with SFS whose vaccination history of Haemophilus influenza type b (Hib) or pneumococcus is uncertain or lacking [1]. This is related to the fact that the prevalence of bacterial meningitis has significantly decreased since the introduction of Hib and conjugated pneumococcal vaccines in Korea and elsewhere [8]. However, if a CNS infection is suspected in children with SFS (meningeal irritation sign, loss of consciousness for more than 30 minutes, or swelling of the anterior fontanel), the use of LP is still recommended [1,6]. LP is also an option in children treated with antibiotics prior to the development of febrile seizures [1]. A recent study of data from children’s hospitals in the United States from 2005–2019 showed that this change was not associated with a delayed diagnosis of bacterial meningitis [4]. These data support the fact that most patients with SFS can be safely cared for without LP [1,4-7].
In children with febrile seizures, blood tests (glucose, electrolyte, and complete blood count) should be considered only in the following conditions: (1) persistent seizure after the first benzodiazepine dose, (2) prolonged loss of consciousness, (3) poor general condition, or (4) signs of dehydration [6,9].
Many studies have reported that electroencephalography (EEG) is not helpful for predicting the development of epilepsy in children with febrile seizures [6]. Thus, EEG is not recommended in children with SFS without a history or signs of neurological disease [1]. When conducting EEG, it is necessary to consider the timing of the recording. Some studies have reported that slowing dominates immediately after a febrile seizure, while epileptiform discharge appears after 7–14 days [10]. Therefore, some researchers recommend performing EEG at 48 hours to 2 weeks after febrile seizures occur [7,10].
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


