




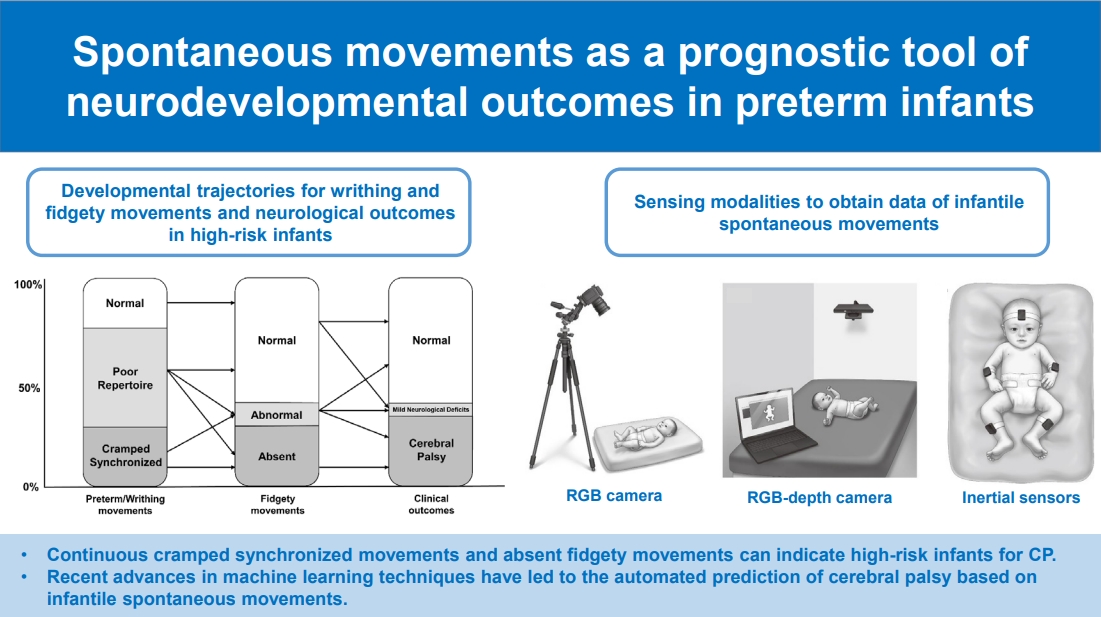
Graphical abstract. CP, cerebral palsy; RGB, red-green-blue.
Introduction
The global incidence of preterm infants is approximately 15 million per year [1]. Preterm birth is a leading cause of neonatal death and closely associated with multiple serious complications such as bronchopulmonary dysplasia, chronic lung disease, retinopathy of prematurity, and intraventricular hemorrhage [2]. Notably, the impact of complications in preterm infants can extend into childhood or adulthood. One such major medical condition, cerebral palsy (CP), is the most common motor disability and presents with permanent abnormal movements, muscle tone, and posture. The overall prevalence of CP ranges from 1.5 to more than 4 per 1,000 live births worldwide [3]. Early intervention should be considered for high-risk infants with CP. The rate of rehabilitation support before 1 year of age in Korea is 34.9%–37.6% [4].
Accurate evaluations should be performed to detect infants at high risk of CP and provide rehabilitation support. Early detection in preterm infants before 6 months of corrected age is emphasized, and several examination tools have been recommended to enable early screening including the Hammersmith Infant Neurological Examination, brain magnetic resonance imaging (MRI), and the General Movements Assessment (GMA) [5]. In particular, the GMA is highly useful for identifying motor dysfunction based on infant’s quality of spontaneous movements (95%–98% predictive of CP) combined with neuroimaging [5]. The GMA is a validated standardized motor assessment used to evaluate video recordings of spontaneous movements of infants <5 months of corrected age [6]. Spontaneous movements can be analyzed to identify abnormal writhing movements or absent or abnormal fidgety movements.
This narrative review aimed to summarize spontaneous movements in healthy infants and their relation to brain development and neural substrates; discuss early markers of spontaneous movements to detect high-risk infants based on the GMA; review recent advances in automatic approaches used to examine infantile spontaneous movements; and suggest the current limitations of assessments based on infantile spontaneous movements and directions for future research.
Spontaneous movements as better indicator of brain function
Spontaneous movements are considered a window for the early identification of high-risk infants from the fetal to postterm periods because they can reflect neurological integrity [7]. Unlike reflexes, spontaneous movements are not evoked by external stimuli. Prechtl [8] proposed an approach to the neurological evaluation of newborns by observing spontaneous movements based on Gestalt perception and named it general movements (GMs). Previous studies of fetuses and preterm and term infants demonstrated that GM assessment results are correlated with both brain lesions in terms of neuroimaging techniques such as cranial ultrasound or MRI and neurological outcomes [9,10]. More recently, Peyton et al. [11] showed that the presence of aberrant GMs at 10–15 weeks of corrected age is associated with adverse neurodevelopmental outcomes and specific white matter microstructural abnormalities contributing to cognitive, language, and motor delays.
Reflexes and responses evoked by external stimuli or physical examinations are relatively less sensitive for detecting brain lesions. Sherrington [12] isolated the spinal cord from the dominant brain and analyzed the mechanism of simple reflex behavior. In brainless animals, simple reflexes are provoked as automatic responses. In decerebrated animals, the quantitative relationship between sensory input and reflexive motor output can be analyzed. It is assumed that reflexes are not optimal indicators of brain integrity or damage, whereas spontaneous movements, such as the expression of spontaneous neural activity, are excellent markers of neural dysfunction caused by brain impairment.
General movements and neural substrates
In mammals and humans, there is a transient structure in the developing brain called neural subplate [13]. The complex and variable characteristics of GMs are assumed induced by modulating cortical subplate activity [14]. When the subplate gradually dissolves by up to 3 months of corrected age, the cortical plate dominates [15]. This is the time when fidgety movements first appear. When cortical activity in the primary sensorimotor cortices shifts from the subplate to the cortical plate at 2–5 months of corrected age, fidgety GMs can reveal cortical development [16]. In turn, the absence of fidgety movements highly indicates neural injury.
Normal general movements
In a human fetus, variable specific movement patterns appear at 9–12 weeks’ postmenstrual age and are known to disappear at 1 year of age. These endogenously generated movements continue after birth, even in preterm infants [17]. GMs are endogenously operated on spontaneous movements that may last from a few seconds to several minutes. GMs were first addressed by Prechtl [8] The movements involve a sequential wave of the arm, hand, leg, foot, neck, and trunk with variable speed and intensity and a gradual beginning and end. The elegant rotations of the limbs and complex movements are usually unpredictable and variable [8]. Before term birth, we refer to them as fetal or preterm GMs [18]. From 40 weeks to approximately 46–49 weeks of postmenstrual age, they are called writhing movements [19]. GMs have a similar appearance from early fetal life until the end of 2 months of corrected age, although age-related minor differences exist. Writhing movements are characterized by small to moderate amplitudes at a slow to moderate speed. At 46–49 weeks of postmenstrual age, GMs with a writhing characteristic gradually disappear and fidgety GMs start to appear [6]. Fidgety movements are oscillating movements of small amplitude and moderate speed with variable acceleration of the neck, trunk, and limbs in all directions. Fidgety movements are present until the end of the first 6 months of life, when antigravity movements begin to dominate (Fig. 1).
Abnormal general movements
The quality of GMs can change when the brain is impaired. Previous studies demonstrated that, in newborn infants with brain lesions, spontaneous movements lose variability, fluency, and elegance as opposed to a mere reduction in motility occurring [6]. The observer’s visual Gestalt perception is important for detecting alterations in sequential movements. At each stage, there are several types of abnormal movements with different predictive values and prevalence (Table 1).
1. Writhing movements
Poor repertoire GMs are monotonic sequences of repertoires. The movements of different body parts showed repetitive patterns with less variability in speed and intensity, similar to normal writhing movements. Although the emergence of a poor repertoire does not necessarily indicate a poor prognosis, serial observations are necessary since they can be followed by normal, abnormal, or absent fidgety movements (Fig. 2) [6]. Cramped synchronized GMs are abnormal and have high predictive value for the outcome. These abnormal GMs appear rigid and lack normal smooth, variable, and fluent characteristics, while all limb and trunk muscles contract and relax almost simultaneously [6]. If this abnormal pattern is observed consistently or dominantly, it is highly predictive of CP [6,20-22]. Chaotic GMs can be observed during the preterm and term periods and even after 40 weeks of postmenstrual age but are rather rare. Movements with large amplitudes and fast speeds involve all limbs and occur in a chaotic order without fluency or smoothness. They consistently appear abrupt [23,24]. Chaotic GMs can often become cramped, synchronized GMs within a few weeks [18].
2. Fidgety movements
The absence of fidgety movements is highly predictive of later neurological impairments, particularly for CP [25]. If fidgety movements are never observed between 9 and 20 weeks of corrected age, this is referred to as “absence of fidgety movements.” Abnormal fidgety movements are rare and have low predictive value. While these movements resemble normal fidgety movements, their amplitudes, speeds, and jerkiness are either moderately or significantly exaggerated.
Prognostic value of general movements
It is widely accepted that the GMA is a highly recommended method of predicting neurological outcomes of young infants along with neonatal MRI and the Hammersmith Infant Neurological Examination [5]. The GMA was previously compared with other neurological examinations or neuroimaging tools [22,26]. Cioni et al. [27] reported that the GMA showed superior sensitivity and specificity to traditional neurological examinations of the Amiel-Tison and Touwen criteria for neurological outcomes until 2 years of age. In this study, the results of the GMA were also highly correlated with neurological outcomes in infants. Another previous study indicated that continuous observations of cramped synchronized GMs showed greater sensitivity and specificity for predicting CP than Dubowitz and Touwen neurological examinations [22]. Additionally, a recent systematic review reported that the sensitivity of neonatal MRI and GMA was 86% and 98%, respectively, and their combination with history taking about risk factors is strongly recommended in high-risk newborns for the early detection of CP [28,29].
The role of the GMA can be extended to predict both motor developmental outcomes and cognitive or behavioral outcomes. A previous study showed that abnormal GMs were correlated with the development of attention-deficit-hyperactivity disorder as well as aggressive behavior [30]. In a prospective study of 31 infants without CP, the presence of abnormal GMs was related to the presence of attention-deficit-hyperactivity disorder [31]. Moreover, infants with autism spectrum disorder more often showed poor repertoire GMs as well as abnormal or absent fidgety GMs than a control group [32]. Likewise, in a review by Einspieler et al. [33], GMA results were highly associated with the later diagnosis of autism spectrum disorder or Rett syndrome. The quality of writhing and fidgety GMs in 17 children who were diagnosed with typical or atypical Rett syndrome showed abnormal GMs during their first few months of life [33].
Since GMs start at an early fetal age, it is essential to administer the GMA to high-risk infants before discharge from neonatal intensive care unit and throughout their development. The prognostic value of the GMA increases with serial observations [21,34]. It is usually recommended to conduct the GMA using several recordings of GMs from the preterm period to 8 weeks of corrected age, and at least one recording during the fidgety periods (9–16 weeks) [35].
Reliability of the general movements observation
The assessment is based on the overall visual Gestalt perception, and standardized training with the observer’s detailed skills is extremely important. GM observation is conducted by individuals who have received certification through 4- to 5-day training courses provided by the GMs Trust (http://www.general-movementstrust.info). It has been reported that approximately 9,000 videos assessed by 800 observers yielded a correct diagnosis rate of 83% after the completion of the training course [36]. Interscorer agreement reliability has a kappa value range of 0.81–0.92 [36-38].
Automated approaches based on infantile spontaneous movements
Recent rapid advances in the fields of computer vision and pattern recognition based on machine learning techniques have led to the publication of numerous articles on automated approaches to GMA. Machine learning is a cutting-edge, datadriven approach that encompasses the intrinsic properties of the constituents of data. It has a core strength of predicting the expert level or, at least, providing supportive information to health professionals [39]. Previous evidence of risk factors or characteristics of spontaneous movements for CP in preterm infants implies that machine learning has great potential for the early detection of high-risk infants with CP [40].
Data acquisition from infantile spontaneous movements is practical using diverse types of sensing modalities. There are 2 categories of sensing modalities for acquiring data on infantile spontaneous movements: indirect (video cameras, 3-dimensional motion capture, and Microsoft Kinect) and direct (inertial sensors, magnet tracking system) [40]. Fig. 3 illustrates several representative sensing modalities used to record infantile spontaneous movements in previous studies [40,41]. The determination of sensing modalities is among the key steps for developing prediction models using infantile spontaneous movements because it can affect the essential properties of movements in each body region, quality, dimension, measurement error, and data acquisition ease.
The model performance for classifying infants at high risk of CP based on machine learning in previous studies seems to be satisfactory with an overall accuracy exceeding 80%–90% [42]. The majority of the developed prediction models utilized 2-dimensional video images, and some studies adopted 3-dimensional video images or data from inertial sensors. Table 2 sum marizes previous studies that developed machine learningbased prediction models or explored features to discriminate infants at low versus high risk of CP or neurologic impairment using 2-dimensional images of infantile spontaneous movements [43-47]. Although machine learning-based prediction models using infantile spontaneous movements showed promising results in previous studies, their clinical utility has not yet been demonstrated in clinical practice [42]. Most previous studies evaluated the model performance using only internal validation without reporting external validation results [42]. Thus, it is strongly recommended that future studies evaluate the performance of prediction models through external validation to confirm their clinical utility in the medical field [48].
Moreover, the discovery of biomarkers based on infantile spontaneous movements using machine learning enables us to understand the underpinnings of neurodevelopment and provides opportunities for health professionals to obtain novel insights. The exploration of novel features in developing machine learning-based prediction models can enhance model usability and help clinicians interpret and recognize them more confidently. Shin et al. [47] indicated that early neurological development in preterm infants is closely associated with movement complexity in terms of sample entropy at the upper and lower limbs, which is considered an important marker for a high risk of CP. This finding is consistent with the results of a previous study in which a lack of complexity might result from injury or dysfunction of the subplate or cortical plate and/or its connective fibers [49].
Challenging issues of clinical evaluations as prognostic tool
According to the guidelines, GMA is among the recommended evaluation tools for the early detection and intervention of preterm infants [5]. However, it is not universally utilized worldwide because of limited access to clinical expertise in GMA [50]. GMA is either a qualitative or semiquantitative evaluation method that is highly dependent on the skills and experience of the assessor. The assessment must be performed by certified individuals who have completed high-quality training courses [42]. Although GMA training courses are held several times a year, their regional distribution remains limited. Considering the privacy issues of educational content containing images of preterm infants, extending training courses by providing online courses for remote learners might be difficult despite the growing global acceptance of online courses. Automated approaches for GMA or prognostication using infantile spontaneous movements based on machine learning can be a good alternative to broaden its applicability [42]. These approaches may be less dependent on the skills or experiences of assessors and provide objective evaluations with quantitative results to support clinicians during the decision-making process for early intervention in clinical practice.
Conclusion
Spontaneous movements in preterm, term, and postterm infants reflect neuronal integrity and can be utilized to identify infants at high risk of developing CP. GMs are spontaneous movements involving the entire body, including the upper and lower extremities, neck, and trunk, before the emergence of voluntary or antigravity movements. In the GMA, abnormal writhing movements, which are categorized as poor repertoire, cramped synchronized, chaotic movements, and absent or abnormal fidgety movements, are highly predictive of CP or other neurological impairments. In particular, continuous cramped synchronized movements and the absence of fidgety movements indicate greater sensitivity and specificity for CP. Recent advances in machine learning techniques have led to the automated prediction of CP or neurological impairments based on infantile spontaneous movements. This may help overcome the limited utilization of the GMA owing to its qualitative or semiquantitative nature and high dependency on the skills and experience of the assessors.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


