




Graphical abstract. BP, blood pressure.
Introduction
The prevalence of hypertension remains high, with 54% of adults diagnosed with hypertension worldwide. Of them, an estimated 3%–5% and 10%–14% developed hypertension and elevated blood pressure (BP), respectively, prior to reaching adulthood [1-7]. Pediatric hypertension can develop secondary to an underlying disease or primary hypertension. Although secondary hypertension is more prevalent and often more severe in children than adults, preventable BP elevation and its cumulative effect remain critical across all hypertension types, even in the general population with normal BP [6]. The increasing trend in pediatric hypertension is concerning given that hypertension is among the leading causes of cardiovascular disease (CVD) [8-11]. A recent study evaluating trends in metabolic diseases among individuals under 40 years of age reported that hypertension had the highest age-standardized mortality rate [12]. Also, among young adults aged 20–39 years, those with an elevated BP exhibited a greater risk of premature CVD than their normotensive counterparts: hazard ratio (HR), 1.14 (95% confidence interval [CI], 1.09–1.18) for elevated BP, 1.67 (1.61– 1.72) for stage 1 systolic and diastolic hypertension (SDH), and 3.13 (3.03–3.23) for stage 2 SDH. In particular, early and long-term exposure to an elevated BP is expected to contribute to targeted organ damage and CVD in young adult populations [13]. However, due to the higher prevalence of hypertension with advancing age, most previous studies focused on older adults [14-16].
The increasing burden of hypertension in the young population can cause an increased disease burden now and in the future; however, direct evidence of an elevated BP and hypertension in children and adolescents remains limited. Therefore, understanding the potential impact of an early elevated BP and its associated risk factors is crucial for reducing individual risks and preventing future public health burdens [17-20]. This review aimed to examine the existing body of evidence linking elevated BP in childhood, primarily primary BP elevation or hypertension, with progression to adult hypertension and CVD as well as identify the risk factors contributing to early-life BP elevation.
Definitions of elevated BP in childhood and adolescence
A large body of literature has reported a continuous relationship between BP and cardiovascular (CV) risk in adults [21]. Although hypertension is traditionally defined by arbitrary cutoff values such as ≥140/90 mmHg based on the magnitude of the risk of CVD, evidence of the continuous relationship between BP and CV risk has prompted efforts to address the risk for individuals below this cutoff. For instance, the 2017 American College of Cardiology/American Heart Association guideline lowered the threshold to ≥130/80 mmHg [17].
However, the definition of elevated BP and hypertension in children and adolescents is complex. Children exhibit considerably lower BP than adults [22]. An individual's BP naturally increases with age and height, requiring differentiation from an abnormal elevation [2]. Moreover, evidence of the long-term risk of target organ damage associated with an elevated BP during childhood remains limited. These limitations hinder the determination of arbitrary cutoffs in children, leading to the definition of pediatric hypertension based on the percentiles of age-, sex-, and height-specific BP distributions in healthy children [2,23]. Pediatric hypertension is identified when BP is markedly elevated, for instance, above the 95th percentile, although this may not adequately address the cumulative CV risk in children with an elevated BP below the 95th percentile [24]. Therefore, various criteria and definitions for elevated BP levels and hypertension in children have been employed based on available evidence.
The 2017 American Academy of Pediatrics (AAP) guidelines define normal BP, elevated BP, stage 1 hypertension, and stage 2 hypertension as screening and management criteria for an elevated BP in children and adolescents [2]. Based on BP distributions in healthy normal-weight children, those aged 1–12 years whose BP levels exceeded the age-, sex-, and height-specific 90th percentiles were classified as having an elevated BP. For adolescents aged 13 and older, the cutoffs are 120–129/<80 mmHg for elevated BP and ≥130/80 mmHg for hypertension. The reference values for older adolescents, which align with those for adults, are supported by robust evidence linking BP to CV risk in adults and young adults [2]. The European Society of Hypertension and Hypertension Canada used repeated BP measurements above the 95th percentile [25]. Additionally, the 2019 Japanese Society of Hypertension Guidelines for the Management of Hypertension established 6 reference values based on age and sex [26]. Hypertension is defined at values of ≥120/70 mmHg for preschool children, with the reference values increasing as children grow, and reaching ≥140/70 mmHg for high schoolers, converging with adult hypertension cutoffs.
The criteria for pediatric hypertension in Korea were aligned with the AAP guidelines as reflected in the 2017 recommendations of the Korean Society of Hypertension [27]. The BP percentile for individuals is calculated by considering age-, sex-, and height-specific percentiles along with the measured BP for children and adolescents; it is then classified based on this BP percentile [27].
Association between elevated BP in childhood and hypertension in adulthood
Increasing evidence suggests that adult hypertension may originate early in life (Table 1). A meta-analysis of longitudinal studies estimated that a one-standard-deviation increase in childhood BP was associated with a higher likelihood of adult hypertension with an odds ratio (OR) of 1.71 (95% CI, 1.50–1.95) for systolic BP (SBP) and an OR of 1.57 (95% CI, 1.37–1.81) for diastolic BP (DBP) [28]. An elevated BP in childhood defined using BP percentiles had an OR of 2.02 (95% CI, 1.62–2.53), while using static BP cutoff yielded an OR of 3.22 (95% CI, 1.90-5.48) [28]. Another study measured baseline BP values among adolescents aged 16–19 years, categorizing them into optimal, normal, and high-normal BP groups according to European guidelines, and subsequently assessed the development of adult hypertension [29]. As a result, the ORs for adult hypertension were 1.30 (95% CI, 1.22–1.39) for the normal BP group and 1.79 (95% CI, 1.67–1.93) for the high-normal BP group compared to the optimal group [29]. Several studies investigated BP tracking and identified distinct trajectories from childhood to adulthood. One study conducted group-based trajectory modeling using BP measurements at the ages of 7, 11, 18, 26, 32, and 38 years in a birth cohort of 975 individuals [30]. Four distinct trajectory groups were identified: normal (22%), high-normal (43%), prehypertensive (32%), and hypertensive (4%) [30]. Individuals in the hypertensive group exhibited an elevated BP during childhood that persisted into adulthood [30].
BP tracking from childhood to young adulthood demonstrates a relatively clear association. For instance, among adolescents with a mean age of 14.2 years, every 10-mmHg increase in SBP and DBP was associated with a 4% increased risk of developing hypertension in their 20s [31]. In contrast, BP tracking from childhood to midadulthood is limited since it requires an extended follow-up period and large sample size [22]. Despite the scarcity of such studies, one tracked the BP of 211 participants from childhood (3–18 years) to middle age (30–50 years) [32]. BP was measured every 10 years from the age 18 years. The BP levels during the early school years and early puberty were strong predictors of hypertension at 50 years of age [32]. Additionally, the International Childhood Cardiovascular Cohort Consortium study found that the prevalence of hypertension in middle-aged adults was 19% among individuals who maintained a normal BP throughout childhood and adolescence and 80% among those with a persistently elevated BP [33]. Interestingly, participants whose BP was elevated during childhood but normalized during adolescence had a lower prevalence of adult hypertension than those with a persistently elevated BP [33]. Most studies reported that BP tracking from childhood to adulthood shows a moderate correlation with that in adulthood [34,35]. A meta-analysis estimated an overall moderate correlation coefficient; as baseline age decreased or the follow-up period lengthened among studies, this BP-tracking correlation tended to weaken [34]. Taken together, not all individuals with an elevated BP during childhood develop hypertension in adulthood, highlighting the potential benefits of early detection and intervention.
Associations between elevated BP in childhood and CVD in adulthood
Hypertension is a well-known risk factor for CVD. The Northern Manhattan Study estimated that the population attributable risk of hypertension for CVD was 24.3% (95% CI, 13.2–35.4) [36]. Although the prevalence of hypertension and CVD is considerably lower in younger populations than in other age groups, the evidence linking elevated BP to CVD risk in young adults is equally robust. Compared to normotensive young adults aged 20–39 years, the HR for CVD development was 1.14 (95% CI, 1.09–1.18) for those with an elevated BP, 1.67 (95% CI, 1.61–1.72) for those with stage 1 SDH and 3.13 (95% CI, 3.03–3.23) for those with stage 2 SDH [37].
The observed CVD risk associated with hypertension in adults appears to extend to children and adolescents, although evidence remains limited owing to the challenges posed by extended follow-up (Table 2). A longitudinal study following late adolescents aged 18–20 years found an association between elevated BP and premature CVD before 55 years of age with an HR of 1.09 (95% CI, 1.04–1.15) [8]. Another long-term study spanning up to 50 years confirmed that, among individuals with a persistently elevated BP from adolescence, one in 10 will experience myocardial infarction, heart failure, ischemic stroke, intracerebral hemorrhage, or CV death before retirement [38].
Even in the absence of a major CV event, an elevated BP during childhood has a cumulative detrimental effect on CV health. A meta-analysis of 12 prospective cohort studies exhibited a significant association between an elevated BP in childhood and adolescence and 3 intermediate indicators of CVD in adulthood: high pulse wave velocity, high carotid intima-media thickness (cIMT), and left ventricular hypertrophy (LVH) [11]. A cross-sectional analysis of 130 children with a persistent BP elevation above the 90th percentile reported that 17% of young patients exhibited concentric LVH, a geometric change associated with increased CVD risk in adults [39]. Additionally, a recent United Kingdom birth cohort study reaffirmed that childhood BP was associated with cumulative cardiac damage in adulthood, and BP levels and echocardiography were assessed in 1,856 adolescents aged 17 and 24 years [40]. An elevated BP was defined as an SBP ≥130 mmHg and DBP ≥85 mmHg, while LVH was defined as a left ventricular mass indexed to height2.7 (LVMI2.7) ≥51 g/m2.7 and left ventricular diastolic dysfunction (LVDD) was defined as left ventricular diastolic function E/A <1.5. An elevated BP in adolescence was associated with worsening LVH (OR, 1.61 [95% CI, 1.43–1.80]) and worsening LVDD (OR, 1.35 [95% CI, 1.21–1.50]) in female participants [40]. The cIMT is a well-established predictor of CVD incidence [41]. A persistently elevated BP from childhood through adulthood nearly doubled the risk of high cIMT compared with consistently normal BP levels [42]. A multicenter study of high BP in pediatric patients, the Adult Hypertension Onset in Youth cohort, demonstrated a linear increase in LVMI and higher prevalence of LVH with increasing SBP. The prevalence of LVH was 13% in normotensive children, 21% in those with an SBP in the 80th–90th percentile, and 27% in those with an SBP above the 90th percentile [43].
Studies utilizing the BP trajectory model added to these findings: participants who developed a high BP in adulthood were not only likely to have an elevated BP in childhood, but they also exhibited suboptimal CV indicators [30,44]. Based on BP data of patients aged 7–38 years, 4 distinct trajectories were identified (normal, high-normal, prehypertensive, and hypertensive) that showed progressive worsening of CV risk factors at 38 years of age, with the hypertensive group displaying the poorest outcomes [30]. The observed risk factors include waist/hip ratio, total cholesterol, low high-density lipoprotein cholesterol, glycated hemoglobin, and triglyceride levels [30]. Another trajectory study assessed subclinical CVD risk based on SBP trajectories throughout childhood. Over a follow-up period of up to 23 years, from baseline (age 5–16 years) into young adulthood, low-, moderate-, and high-increasing groups were identified. A progressive worsening of cIMT was observed across these groups, with values of 0.50, 0.52, and 0.55 mm, respectively [44]. Similarly, the mean LVMI values were 65.41, 72.02, and 79.23 g/m2, respectively [44].
Previous studies also suggested that elevated levels in childhood, followed by normalization, were not significantly associated with increased subclinical atherosclerosis or arterial stiffness [42,45]. However, it remains unclear whether this reduction was due to active interventions following the recognition of BP elevation. Although further research is needed to clarify and quantify the causal relationship between childhood BP and adult CV outcomes, these studies indicated the long-term and cumulative effects of persistent BP elevations throughout childhood and adolescence on the development of hypertension and CVD later in life.
Factors associated with elevated BP in childhood and adulthood
Physiologically, BP increases with age and height throughout childhood, with the greatest increase occurring during adolescence [46]. However, this natural increase does not occur uniformly across all children; some may experience a steeper increase, potentially predisposing them to heightened CV risk later in life. Previous studies demonstrated early-life predictors associated with hypertension in adulthood, including perinatal factors such as a low birth weight and maternal history of pregnancy hypertension; genetic factors such as a family history of hypertension; and sociodemographic factors such as male sex and specific ethnic groups (e.g., Black or African American populations) [30].
In addition to these predictors, various modifiable risk factors contribute to the excessive increase in BP from childhood to adulthood. For instance, a high sodium intake has been identified as a significant risk factor [47,48]. A meta-analysis of 18 studies with high-quality sodium intake data found that each gram of sodium intake per day was associated with a 0.8-mmHg increase in SBP and a 0.7-mmHg increase in DBP [47]. Another study using the National Health and Nutrition Examination Survey reported that a sodium intake of >3,450 mg was associated with elevated BP (OR, 1.36 [95% CI, 1.04–1.77]) compared to ≤2,300 mg per 2,000 calories [48]. Notably, a pioneering study in the 1960s compared BP levels by age between 2 indigenous Amazonian tribes [49,50]. The Mundurucus tribe, influenced by Western dietary practices and salt incorporation into its diet, exhibited a pronounced age-related increase in BP as observed in most acculturated societies. In contrast, the Carajás tribe, which remains unacculturated and uses plant ash instead of salt, maintained low BP levels throughout adulthood [49]. These findings underscore the cumulative impact of a high sodium intake on BP elevations despite limitations such as an insufficient control of confounders. They also suggested that the natural distribution of BP in the absence of excessive salt exposure may shift rightward compared with the distribution observed in contemporary societies, while previous studies were largely conducted in acculturated populations. In this context, the 2017 AAP guidelines recommend the Dietary Approaches to Stop Hypertension (DASH) diet as an initial intervention for children with an elevated BP [2]. A randomized controlled trial found that youth aged 11–18 years in the 6-month DASH diet intervention group exhibited a significant reduction in SBP (2.7 mmHg) and improvement in flow mediated dilation (2.5%) compared to the routine care group [51].
The increasing prevalence of insufficient physical activity and sedentary lifestyles has contributed to a higher prevalence of both obesity and early elevated BP in childhood and adolescence [52-55]. A systematic review reported that high-intensity interval training interventions are associated with small but significant reductions in SBP and DBP [56]. Also, school-based interventions were proven effective; compared to the traditional curriculum, high-intensity interval training during the first 20 minutes of school physical education classes held 2 days a week resulted in a significant decrease in SBP and vascular stiffness at the 3-month assessment [57].
Obesity is a strong risk factor for elevated BP in both children and adolescents. A national case-control study found that a one-unit increase in body mass index (BMI) was associated with a 0.56-mmHg increase in SBP and a 0.54-mmHg increase in DBP in obese children [55]. Moreover, an increase in age- and sex-adjusted BMI was associated with elevated SBP and DBP in both obese and nonobese children [55]. A longitudinal UK cohort study that followed 1,856 adolescents for 7 years also reported that an elevated DBP was 1.41 times more likely to worsen LVH, while an elevated SBP was 1.30 times more likely to increase left ventricular filling pressure in overweight and obese participants than in normotensive groups [40]. However, the heightened risk of obesity in childhood seems modifiable: Compared to participants who maintained a normal weight throughout childhood and young adulthood, the relative risk of adult hypertension was 3.79 (95% CI, 2.49–5.64) for overweight participants during both periods [58]. It is noteworthy that individuals who were overweight in childhood but normal weight in young adulthood did not show a significant increase in risk (relative risk, 1.05 [95% CI, 0.33–3.40]) [58].
Additionally, sleep disturbances in childhood, including poor sleep quality, sleep interruptions, and short sleep duration (≤8 hr/night), are also associated with higher BP levels, especially in adolescents [59]. Obstructive sleep apnea is a pathological sleep condition common in children with obesity-related hypertension [60]. Other risk factors, such as a low socioeconomic status (e.g., poverty) and multiple adverse childhood experiences, are outlined in Table 3.
Conclusion
Elevated BP and hypertension in children have received relatively insufficient attention owing to the low prevalence of primary hypertension and CVD and the inherent difficulties conducting long-term studies to assess their impact in pediatric populations. However, emerging evidence suggests that hypertension and CVD develop early in life.
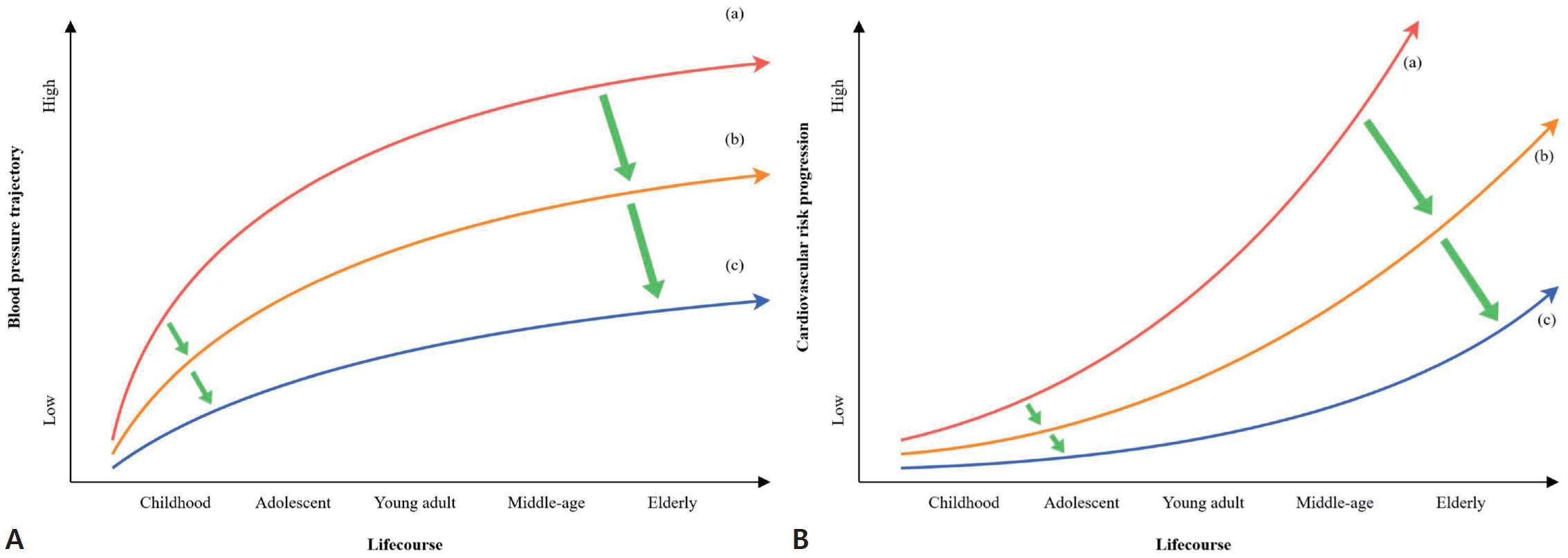
Although BP naturally increases with age during childhood and adolescence, the rate and pattern of this increase vary, with some individuals maintaining an optimal BP and others experiencing a steeper rise. The effect of an elevated BP during childhood may not be immediately apparent. However, without timely and appropriate intervention, elevated BP trajectories can persist into adulthood, substantially increasing one's CV risk (Fig. 1). Numerous studies, both direct and indirect, have demonstrated that a high BP during childhood significantly increases the risk of hypertension in adulthood. Prolonged exposure to a high BP during childhood leads to cumulative subclinical changes that potentially result in irreversible cardiac structural alterations or major premature CV events. While future efforts to establish evidence that guides consensus—such as the necessity of regular BP screening and determining optimal timing and target BP for pharmacological treatment in children—remain under debate, the benefits of maintaining optimal BP throughout childhood and addressing elevated BP through lifestyle modifications are already evident. Promoting healthy behaviors in children and adolescents, such as maintaining a healthy body weight, reducing sodium intake, engaging in regular physical activity, abstaining from smoking, and ensuring adequate sleep, is crucial for managing BP from an early age and fostering lifelong habits that support CV health. These efforts are essential for reducing individual risk and efficiently mitigating the future burden on public healthcare systems given the substantial burden of hypertension and CVD.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


