




Introduction
Kawasaki disease, first described by Dr. Tomisaku Kawasaki in 1967, is an acute febrile vasculitis of unknown origin that mostly affects children under 5 years of age [1]. The incidence of Kawasaki disease is higher among children of Asian ethnicity as evidenced by epidemiological data from Hawaii [2], and Korea has the second-highest incidence after Japan [3-5]. In a 2015–2017 nationwide survey in Korea, the overall incidence was 196.9 per 100,000 children younger than 5 years, with a mean age at diagnosis of 33.0±24.8 months; 83.5% of patients were under 5 years of age [5].
The systemic inflammation in all medium-sized arteries, multiple organs, and tissues during the acute febrile phase is characteristic of Kawasaki disease [6], which has a predilection for the coronary arteries, leading to coronary artery aneurysm in around 25% of patients without proper treatment [7]. Vasculopathy in Kawasaki disease includes acute self-limiting necrotizing arteries causing saccular aneurysms, subacute/chronic vasculitis, and luminal myofibroblastic proliferation possibly related to progressive arterial stenosis and thrombosis [8]. These cardiac sequalae might cause myocardial infarction or sudden death in adulthood as well as in the acute phase [9]. In developed countries, Kawasaki disease has been emerging as the leading cause of acquired heart disease, surpassing acute rheumatic fever [10].
Several studies of intravenous immunoglobulin (IVIG) in the acute phase have been conducted to reduce the prevalence of coronary artery abnormalities and resulted in a reduction in the incidence of coronary artery aneurysms from 25% to around 4% [11-13]. Nowadays, a single high dose of IVIG and aspirin are the mainstream first-line acute treatment [14,15]. A recent survey in Japan reported the acute cardiovascular complication of 7.9%, coronary dilation of 5.6%, coronary aneurysm of 0.82%, and giant aneurysm of 0.13% [4], and Korean nationwide surveys performed between 2015 and 2017 reported coronary artery dilation in 17.1% and coronary artery aneurysm in 1.7% [5]. Both surveys used dichotomous criteria from by the Japanese Ministry of Health and Welfare for diagnosis of coronary artery abnormalities.
Early diagnosis and proper treatment are imperative to preventing coronary complications, for which the evaluation of coronary artery abnormalities is fundamental. In this article, the diagnosis of coronary artery abnormalities in Kawasaki disease and adaptation of the z score system are reviewed.
Diagnosis of Kawasaki disease
Due to a lack of pathognomonic diagnostic tests, the characteristic clinical manifestations of Kawasaki disease have formed the basis of its diagnosis: fever, bilateral nonexudative conjunctivitis, erythema of the lips and oral mucosa, changes in the extremities, rash, and cervical lymphadenopathy.
The main diagnostic criteria of Kawasaki disease are based on the guidelines of the American Heart Association (AHA) in 2017 and the Japanese diagnostic guideline (6th revised edition) [14,16,17]. These 2 guidelines have similar criteria with few differences. According to the AHA guidelines, the diagnosis of complete Kawasaki disease was based on the presence of fever for more than 5 days and ≥4 of 5 principal clinical features. Meanwhile, in the Japanese guidelines, the count of febrile days is not essential and the redness of the bacille CalmetteGuèrin inoculation can be considered a skin rash, one of its principal clinical features. Additionally, the Japanese guidelines regard fever as among the principal clinical features and define complete Kawasaki disease as the presence of at least 5 of the 6 principal clinical features. Complete Kawasaki disease can also be diagnosed with the presence of 4 principal clinical features after the exclusion of other febrile illnesses, and coronary artery dilation (z score ≥2.5), absolute diameter ≥3 mm (<5 years old), or ≥4 mm (≥5 years old).
However, several patients lack full diagnostic clinical features with persistent unexplained fever and are eventually diagnosed with incomplete Kawasaki disease. The incidence of incomplete Kawasaki disease has increased to 20.6% in Japan and 44.9% in Korea in recent reports [5,17]. Incomplete Kawasaki disease was previously defined as a febrile status with fewer clinical manifestations and coronary artery abnormalities [18]. For patients with few clinical manifestations but in whom Kawasaki disease is suspected, the AHA suggested an algorithm for the diagnosis of incomplete Kawasaki disease in 2004 [19] and revised it in the 2017 guideline [14]. In patients with persistent unexplained fever ≥5 days and 2 or 3 compatible clinical criteria, incomplete Kawasaki disease should be considered. If inflammatory markers are elevated (C-reactive protein ≥3 mg/dL and/or erythrocyte sedimentation rate ≥40 mm/hr) and additional laboratory tests or echocardiographic findings are compatible, incomplete Kawasaki disease can be diagnosed and IVIG treatment should be administered. In this algorithm, the echocardiographic criteria are as follows: positive if any of the following 3 conditions are met: (1) z score ≥2.5 for the left anterior descending coronary artery (LAD) or right coronary artery (RCA); (2) coronary artery aneurysm; (3) ≥3 other suggestive features including decreased left ventricular function, mitral regurgitation, pericardial effusion, or z scores for the LAD or RCA of 2–2.5.
Meanwhile, in the Japanese guideline [16,17], incomplete Kawasaki disease is defined as the presence of 3 of 6 principal clinical features with coronary artery dilation with the exclusion of other febrile illnesses or in the case of the presence of 3 or 4 principal clinical features without coronary artery dilation but with features from the list of “other significant clinical features,” which includes an elevated hepatic transaminase level early in the course the disease, increased leukocytes in the urine sediment of an infant, thrombocytosis in the convalescent phase, elevated brain natriuretic peptide (BNP) or NT-pro BNP level, mitral valve regurgitation or pericardial effusion on echocardiography, enlargement of the gallbladder (hydrops of gall bladder), or hypoalbuminemia or hyponatremia. Incomplete Kawasaki disease may be considered in the presence of ≤2 principal clinical features after the exclusion of other diagnoses. In both guidelines, coronary artery abnormalities are crucial criteria for the diagnosis of complete or incomplete Kawasaki disease.
Evaluation of coronary artery abnormalities in Kawasaki disease
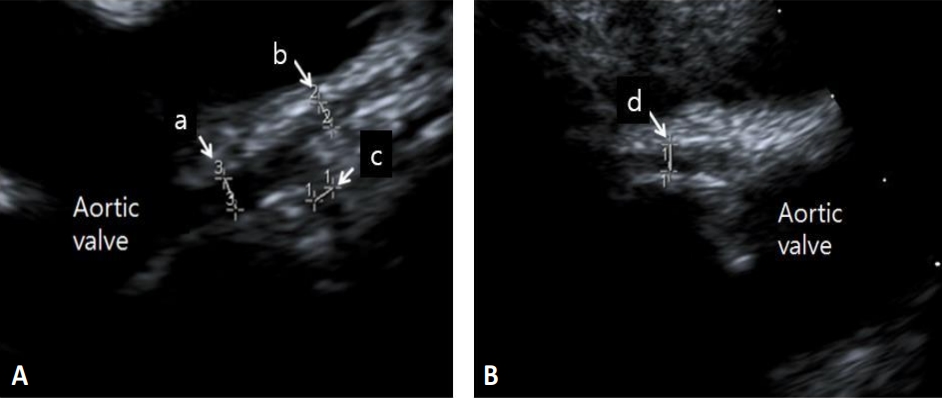
Echocardiography has been the primary imaging modality for assessing coronary artery abnormalities in Kawasaki disease. A standard image should be obtained for coronary artery diameter measurement with the highest-frequency transducer at the minimum gain setting. The 2-dimensional echocardiographic imaging of the left main coronary artery (LMCA), LAD, left circumflex artery (LCX), and RCA on multiple imaging planes and transducer positions are required for optimal visualization (Fig. 1) [20-22]. AHA guideline recommends that the initial echocardiogram be performed as soon as possible to ensure proper diagnosis and treatment [14]. Dominguez et al. [23] reported the importance of the initial echocardiography within the first week of illness. In this study, 81% of coronary artery abnormalities in patients with Kawasaki disease were identified on the initial echocardiography.
In the early period, coronary artery dilation was defined based on the coronary artery size by the Japanese Ministry of Health and Welfare (Research Committee on Kawasaki Disease, Subcommittee on Standardization of Diagnostic Criteria and Reporting of Coronary Artery Lesions in Kawasaki Disease) [24]. Dilated lesions were defined as any coronary artery internal lumen diameter greater than 3 mm for children <5 years of age and 4 mm for those ≥5 years of age. It also included a lesion 1.5 times the diameter of an adjacent normal segment. Additionally, the Japanese Circulation Society classified coronary aneurysms based on absolute diameters as follows: (1) small aneurysm or dilatation: an internal luminal diameter ≤4 mm, or in children ≥5 years of age, lesions with an internal diameter <1.5× that of an adjacent segment; (2) medium aneurysm: the internal luminal diameter >4 mm and <8 mm, or in children ≥5 years of age, lesions with an internal diameter 1.5–4× that of an adjacent segment; (3) giant aneurysm: internal luminal diameter ≥8 mm, or in children ≥5 years of age, lesions with an internal diameter >4× that of an adjacent segment [25]. These arbitrary dichotomous criteria were defined based on clinical experience and have been widely accepted worldwide.
However, concern has persisted that the absolute cutoff criteria might underestimate subtle changes to the coronary arteries and result in misclassification of the coronary artery abnormalities in Kawasaki disease, as these criteria could not account for patient size [26-31]. Mean body surface area (BSA)–adjusted dimensions of proximal LAD and RCA in patients with normal coronary arteries by the Japanese Ministry Health and Welfare criteria (JMH criteria) were significantly larger than those of normal subjects during a 1-year follow-up period; among them, 27% had at least one coronary artery with a ≥2 standard deviation (SD) BSA-adjusted coronary dimensions [26]. Similarly, patients without any coronary artery abnormalities by JMH criteria showed increased coronary artery diameters at admission and at 2–3 weeks compared to the normal groups in another study [27]. Particularly, in the initial measurements, JMH criteria underestimated the prevalence of coronary abnormalities compared to that defined by BSA-adjusted z score (11% vs. 23%) [28]. Moreover, Manlhiot et al. [29] reported that the aneurysm classification by JCS criteria could underestimated the coronary artery aneurysm severity of 19%–32% of small aneurysms and 35%–78% of medium aneurysms. They suggested the classification using a z score system, which could discriminate coronary artery aneurysms more efficiently and show better correlations with clinical outcomes.
Recent guidelines have accepted the BSA-adjusted z score system for the diagnosis of coronary abnormalities. The 2004 AHA guideline adapted the z score system as one of the definitions of coronary abnormalities for the diagnosis of incomplete Kawasaki disease as described above [19]. The recently revised 2017 AHA guideline updated the definition of coronary abnormalities and the aneurysm classification by the z score system [14]. They defined small aneurysms as those with a z score of ≥2.5 to <5.0, medium aneurysms as those with a z score of ≥5 to <10 and an absolute dimension <8 mm, and large or giant aneurysms as those with a z score of ≥10 or absolute dimension ≥8 mm (Table 1). The recent Japanese guidelines also adopted the z score system for the classification of coronary artery abnormalities [17]. In this guideline, coronary dilation is defined as a z score of internal coronary artery diameter ≥2.5 SD units or absolute diameter ≥3 mm (<5 years old) or ≥4 mm (≥5 years old) and coronary artery lesions in the acute phase are defined using both z score and absolute values (Table 1).
Development of z score formulas
Several BSA-adjusted z score formulas for coronary arteries have been established using various regression methods (Table 2). The Boston z score system for the LMCA, LAD, and RCA derived from 89 healthy subjects by de Zorzi et al. [26] was initially generated to evaluate its clinical utility in patients with Kawasaki disease. Since then, more subjects were incorporated by report without the publication of its evolving formula, and this updated Boston z score system has been widely used in North America [32-35]. McCrindle et al.36) derived the z score formula for the LMCA, proximal LAD, and proximal RCA derived from 221 healthy children aged 0–18 years using exponential regression method and evaluated the changes in the coronary arteries that occur in Kawasaki disease patients. Olivieri et al. [37] used a logarithmic regression model and suggested z scores for the LMCA, LAD, and RCA from 432 normal echocardiograms of normal subjects aged 0–20 years. Dallaire and Dahdah [38] established z scores for the LMCA, LAD, LCX, and the proximal, mid, and distal RCA using regression with the square root of BSA from data of 1,033 children. Kobayashi et al. [39] used the lambda-mu-sigma method to develop a z score model. They collected 3,851 healthy children ≤18 years of age and established sex-specific z scores for the LMCA, proximal LAD, proximal LCX, and proximal RCA. They also created a Microsoft Excel-based z score calculator (http://raise.umin.jp/zsp/calculator/). Lopez et al. [40] also recently established a z score using the data of 3,566 healthy, diverse, and nonobese children at 19 centers in North America, which was represented by The Pediatric Heart Network Investigators. Using exponential regression, they provided z scores for the LMCA, LAD, and proximal RCA that were well correlated with the Boston z score [33]. The regression equations and a z score calculator are also available on the Pediatric Heart Network website (https://www.pediatricheartnetwork.org/z-scores-calculator/). All of these formulas were normalized to BSA. BSA was calculated using the DuBois formula for Olivieri z scores and Haycock formula for the rest except Boston z score. The data from North American population were used in the Boston, McCrindle, Olivieri, Dallaire, and Lopez z score systems and the Japanese population in the Kobayashi z score system. There are also several other z score formulas published in Asia [27,41].
Clinical application of z score
In addition to the diagnosis of Kawasaki disease, a long-term treatment plan was established based on the z score system. In the 2017 AHA guideline, long-term assessment and counseling and long-term thromboprophylaxis such as lowd-ose aspirin, anticoagulation, and dual antiplatelet therapy is recommended according to the risk classification of coronary artery abnormalities based on the z score system [14]. Patients with coronary artery dilation only (z score 2 to <2.5) are recommended low-dose aspirin for 6–8 weeks (class IIa; level of evidence, C). If luminal dimensions have returned to normal by 4–6 weeks after onset, the patient may be discharged from cardiology care considering a follow-up period of 12 months (class IIa; level of evidence, C). Patients with current or persistent large and giant aneurysms (z ≥10 or absolute dimension ≥8 mm) are recommended combined thromboprophylaxis (low-dose aspirin [class I; level of evidence, C] + warfarin [class IIa; level of evidence, B] or low-molecular-weight heparin [class IIa; level of evidence, C]) with cardiologic assessments including echocardiography and electrocardiography at 1, 2, 3, 6, 9, and 12 months after the episode of acute Kawasaki disease in the first year and every 3–6 months thereafter (class IIa; level of evidence, C) (Table 3).
Meanwhile, Japanese guidelines recommend echocardiography or electrocardiography at 1, 2, 6, 12 months, and 5 years (or yearly) until 5 years of age for patients with no or transient dilation. Patients with remaining giant aneurysms are recommended to undergo these exams every 6–12 months. Lowdose aspirin is recommended for 2–3 months after onset (class I; level of evidence, C) and should be continued for patients with persistent coronary artery aneurysm (class I; level of evidence, C). Antiplatelet drugs such as clopidogrel, ticlopidine, and dipyridamole are used in combination with low-dose aspirin for patients with medium or large coronary artery aneurysms (class IIa; level of evidence, C), and warfarin is used in combination with low-dose aspirin for patients with large coronary artery aneurysm, a history of myocardial infarction, and thrombosis in the coronary artery aneurysm with an international normalized ratio of prothrombin time target range of 2–2.5 (class IIa; level of evidence, C).
Prognosis of coronary artery abnormalities according to z score classification
The initial coronary z score and the difference between the initial and follow-up z scores could be possible predictors of subsequent coronary artery abnormalities [42]. Also, the diagnosis using z score classification was well correlated and predictive of outcomes, especially in patients with giant aneurysms (z score ≥10) [43,44]. In an international study of 34 institutions, patients with a z score <10 did not show luminal narrowing, thrombosis, or major adverse cardiovascular complications. About 99% of patients with small (2.5≤ z score <5), 92% with medium (5≤ z <10), and 57% with large (z ≥10) coronary aneurysms showed normalized luminal diameters at 10-year follow-up [44]. Another 15-year follow-up study showed that the maximum internal diameter of the coronary artery at 2 months after onset had a strong relationship with following changes in the late period [45]. The coronary aneurysm of maximum diameters ≥8 mm at 2 months did not show significant changes after 1 year, while the coronary aneurysm <8 mm significantly decreased in size and the coronary aneurysm <6 mm with a z score <7.5 could be normalized in the late period. Table 4 summarizes the results of recent studies. A nationwide survey of patients with coronary aneurysm diameter >6 mm in Korea showed a persistent coronary aneurysm in 96% of them, while 31% developed coronary stenosis.46) However, the z score system was not applied in this study, and a comparative study using a z score system and including a large number of patients is needed to evaluate the prognostic value of the z score system in the Korean population.
Impact of z scores in managing Kawasaki disease
Although coronary artery aneurysm classification is a better predictor than the absolute diameter criteria, there are some issues with its clinical application. Each z score formula yielded slightly different results, which could influence the diagnosis of coronary artery abnormalities, and the discrepancy of calculated z scores is greater for larger coronary aneurysms [30,31,32,34]. For example, an LAD of 2.5 mm in a 2-year-old boy with a weight of 13 kg and a height of 90 cm could be normal on Olivieri’s formula but small aneurysm on Lopez’s formula, while a z score of an 8-mm LAD in boy with the same BSA could be 8.33–24.62 according to the z score formula (Table 5).
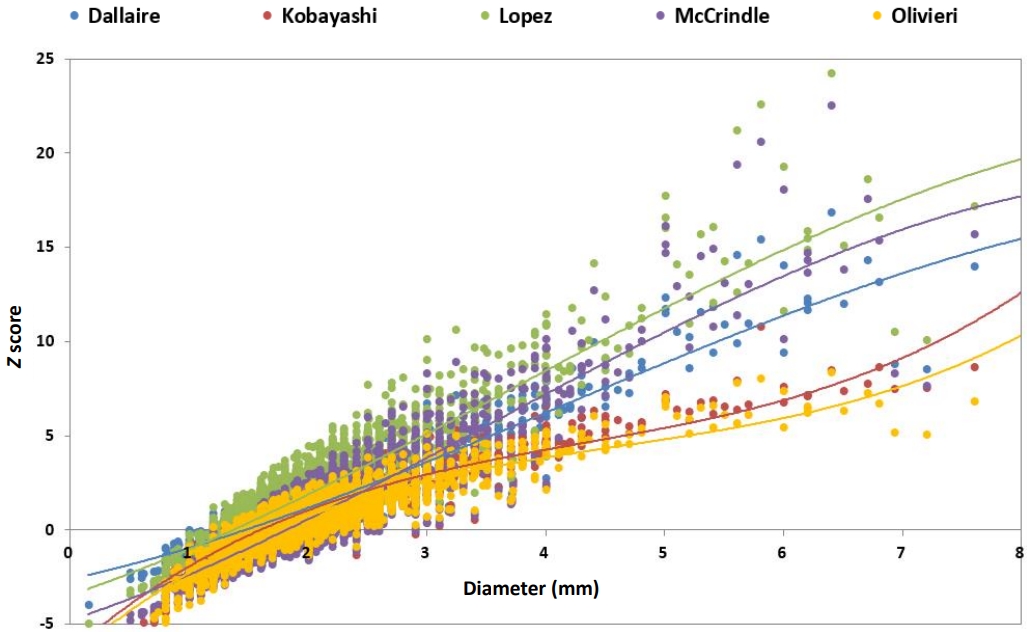
Compared to the range of lower z scores (1.5–3), the range of large z scores (7–14) showed the noticeable discrepancy among the Boston, Olivieri, and Dallaire z score systems [32]. A comparative study using the data of 181 healthy Korean children showed the statistical feasibility of normal distribution among the McCrindle, Oliveri, Dallaire, and Kobayashi z score systems [47]. However, Kim et al. [31] reported a large nationwide retrospective cross-sectional analysis of 6,889 Korean children with Kawasaki disease in which the choice of guidelines or z score systems could result in different rates of coronary artery abnormalities, and the calculated z scores showed the discrepancies among the z score systems. The z score formula of LAD by Lopez produced the highest z scores, while that by Olivieri produced the lowest z scores among McCrindle, Olivieri, Dallaire, Kobayashi, and Lopez’s z scores, and the discrepancy was maximized in the extreme dimension (Fig. 2). In the analysis of the 4 z score systems from North America (The Boston, Dallaire, Olivieri, and Lopez z score systems), the acute coronary abnormalities were 24%–55%, especially in the LAD [34].
Additionally, the choice of z score system influenced the classification of coronary artery aneurysms related to the long-term treatment plan [31,34]. Patients with giant aneurysms by Dallaire z scores were diagnosed as having medium aneurysms in 58% of cases and giant aneurysms in 42% of cases by the Kobayashi z score in the report by Kim et al. [31]. Similarly, up to 22% of Kawasaki patients could have a changed long-term anticoagulation treatment plan due to the differences among the Boston, Dallaire, Olivieri, and Lopez z score systems in the report by Lorenzoni et al. [34]. They reported that the Dallaire z score system diagnosed the most aneurysms in the LMCA, the Lopez z score system in the LAD, and the Boston system in the RCA.
This discrepancy may be due to various reasons. These BSA-adjusted z score systems used different BSA equations and were derived from different normal population sizes, sexes, and races. The regression methods also differed according to the z score system. In the report by Kim et al. [31], among the 4 z score systems using the Haycock equation in the BSA calculation, 3 z score systems from North America yielded higher z scores in every coronary artery than the Kobayashi z score system, which implies a possible ethnic effect of the z score formula.
Because the z score system is strongly related to risk stratification and the long-term treatment plan, the z score formula should be selected carefully and consistently. Until now, there has been no coronary artery z score formula derived from data from a large Korean population. Further research is needed to determine the ideal coronary z score system for this ethnic group and evaluate its prognostic value.
Conclusion
The diagnosis of coronary artery abnormalities is imperative in Kawasaki disease. The coronary z score system has been widely adapted in the guidelines and clinical field to evaluate coronary abnormalities and classify risk stratification according to coronary aneurysms. The classification of coronary artery aneurysms using the z score system is well correlated with clinical outcomes. The choice of z score formula yields different results, possibly related to the diagnosis of coronary artery abnormalities, and the discrepancy of calculated z scores is greater for the larger coronary aneurysms. A careful choice of z score formula and its consistent use is needed to enable its clinical applications.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


