

Introduction
Somatic growth in children was advanced during last few decades with the change of socioeconomic development. Recently weight gain is more prominent and obesity is emerged as a public health issue1). Adequate organ growth is essential in growth and directly related to body growth2). Organ growth is important and it is directly related to its function. Measurement of weight, height (body length, in children less than 2 year old) and anthropometric indices such as body surface area (BSA), body mass index (BMI), Rohler and Kaup index are used to evaluate the growth status2). We choose renal length as a surrogate of organ growth in growing children. As the kidney is one of the most important organ and measurement of renal length is somewhat easier than other major organs, accurate measurements of the kidneys allows us for the comparison with other major organs3). The renal length in children grows according to body growth and is known to be associated with the height and weight2,3) as well as kidney function.
Urinary tract infection (UTI) is a common disease in children. If UTI was suspected, patients may undergo imaging studies including ultrasonography (US) and dimercaptosuccinic acid (DMSA) scan. Data of the renal length collected from the results of these work were analyzed.
The aim of this study was to evaluate the association of renal length, as a surrogate of organ growth, and somatic parameters and analyze the affecting factors for renal size during growth.
Materials and methods
Sixty-six children who were admitted with the impression of urinary tract infection in the department of pediatrics at Konkuk University Medical Center, from November 2007 to July 2009, were enrolled. Medical records were reviewed retrospectively, when the result of both renal US and DMSA scan were available, data of anthropometric variables including age, sex, heights, weights were obtained and body surface area, height z-score, weight z-score, Rohler index and Kaup index were calculated.
Rohler index = weight (kg)/height (cm)3 × 107
Kaup index = weight (g)/height (cm)2 × 10
Patients with abnormal renal morphology, including renal swelling, vesicoureteral reflux or renal cortical defect were excluded.
Body weight was measured to the nearest 0.1 kg (CAS, Seoul, Korea) and height was measured to the nearest 0.1 cm using a Harpenden stadiometer (Holtain Ltd., Crymych, UK). The comparison of height and weight according to age was revised to z-score using the 2007 Korean standard growth chart for children4). Two methods used for BSA calculation, those equations were as follows5,6):

BSA II (m2) = 0.1 + weight (kg)/30 (if weight is less than 30 kg)
The longest axis from upper pole to lower pole of the kidneys were measured with US in prone position, by one radiologist. Renal length was measured on the planar DMSA image, by assessment of the maximum pixel length and converted to centimeters7). The DMSA scan images were obtained and interpreted by a single nuclear medicine doctor.
Subjects were divided into 2 groups with the result of urine culture and each renal size were compared between groups. As in subgroup analysis, anthropometric characteristics did not show significant difference, correlation and regression analysis was conducted as a whole group.
We examined the difference between the measurement method (DMSA scan and US), with the t-test. Pearson correlation analysis between renal length and anthropometric parameters were conducted. Contributing factors for renal growth were evaluated with regression analysis. SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) were used, P<0.05 was considered statistically significant.
Results
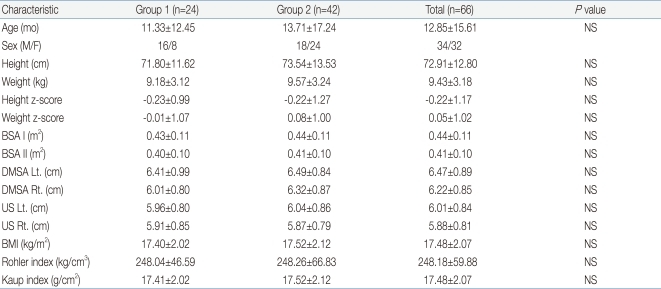
A total of 66 patients who were admitted with the impression of UTI were enrolled in the study. They were divided into two groups. Group 1 was consisted of 24 subjects (mean age, 11.33±12.45 months) with positive urine culture and group 2 was consisted of 42 subjects (mean age, 13.71±17.24 months) with negative urine culture. Anthropometric characteristics including age, sex. height, weight, height z-score, weight z-score, BSA I, BSA II, Rohler index, Kaup index, and each renal length measured by DMSA and US showed no significant difference between two groups (Table 1). According to these results, correlation and regression analysis was conducted as a whole group.
We choose the left DMSA as a representative of the renal length, as in comparison of the each side of renal length by two method, the correlation coefficient between DMSA and US was higher on left (r=0.783) than right (r=0.693) (data were not shown).
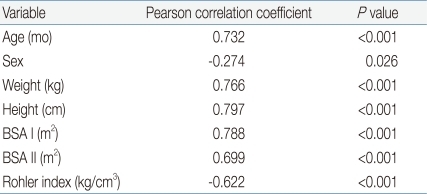
The result of Pearson correlation analysis between somatic variables and left renal length on DMSA scan showed that age, sex, weight, height, BSA I, BSA II and Rohler index were correlated significantly (Table 2).
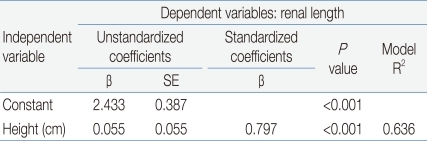
We tried to figure out the independent variables which influence on the renal length by using the stepwise multiple regression analysis. Regression analysis was conducted separately with BSA I or BSA II. The significant contributing factor for renal growth was height (R2=0.636, P<0.001) (Table 3). Other factors (age, sex, weight, BSA I, BSA II, Rohler index, Kaup index) were not remained.
Discussion
Knowledge of renal length can be critical to the management children with chronic pyelonephritis, obstructive renal disease, and chronic glomerulonephritis with early onset in their life8,9).
Somatic growth in children was advanced during last few decades with the change of socioeconomic development. Recently weight gain is more prominent than height and obesity is emerged as a public health issue. Adequate organ growth in children is important and it is directly related to its function7).
DMSA scan, US, intravenouspyelogram (IVP), computerized tomography (CT), and magnetic resonance imaging (MRI) are used to measure the size of the kidneys. For children, relatively noninvasive and cost effective technique such as US and DMSA are commonly used. The accuracy of these imaging methods depends on either the position of the probe or the experience of physician.
There was the difference that could be up to about 1 cm between intraobserver and interobserver of measuring kidney size with US10-13). In this study, one radiologist or one nuclear medicine doctor did all the measurement for decreasing inter-observer variability. Kim and Park8) reported close relationship between the renal length and height using US in normal children. The DMSA scan has been known to be the most sensitive test for the diagnosis of renal cortical defect14,15), which has been used for the diagnosis of acute pyelonephritis during the acute stage of a UTI. This can also be used to measure renal length and diagnose a renal scar three to six months after treatment.
Recently, adult renal length and the capacity measurement using MRI was reported9). They assessed the validity of the ellipsoid formula for evaluating kidney volume and determined the normal range of renal length and volume of a patient with unknown history of kidney disease. For patients, who were unaware of a history of kidney disease, the measurement of their renal length and volume using MRI was larger than that obtained by US, a commonly used reference9).
The use of renal length as a reference for the diagnosis of congenital renal disease such as renal agenesis or congenital ureteric stenosis of the newborn was reported16). The longest straight axis between the upper pole and lower pole of the kidney was measured longitudinally; the horizontal line was measured between the inner and outer projecting parts to meet the longitudinal line using US among the newborn16). Both measurement and assessment of the width of the renal parenchyma are considered to be very important.
Measuring renal length with IVP has not been used nowadays because it has the risk of radiation exposure during comparing the longest axis of the upper pole and the lower pole to the length between the L1-L4 vertebra17). According to the data about kidney sizes obtained from 19 adults comparing ultrasonogram with CT, the length of kidney on US was similar to that of CT18). The kidney width showed no significant difference between two methods.
Rossleigh et al.7) reported on the sensitivity and specificity of DMSA scans and US for the diagnosis of a renal scar in pigs with reflux nephropathy, and comparing the size of the kidneys. The DMSA scan showed a higher sensitivity and specificity than US when assessing the renal scar. Furthermore, in comparison of the renal length measured by DMSA scan and US to length measurement at pathologic examination, it was noted that the renal length by DMSA scan was, on average, 6% longer than anatomic length; the renal length by US was 22% smaller than anatomic length. Ultrasound measurement on this study underestimated renal length significantly when compared with pathology. Ultrasound was technically difficult in these animals and its images taken at full inspiration could not obtained7). They reported that the DMSA scan is preferred method for the detection of renal cortical scarring and accurate renal length measurement tool compared to US7). It was widely believed that DMSA scan is an objective measuring tool and it has high reproducibility19).
Considering both the weight and height simultaneously is important in assessment of growth in children. The weight for adults is 20-fold increased compared to the newborn period; however, the BSA increases about 8-fold5,6). The somatic variables including age, height, weight, BSA, Rohler index showed a significant correlation with renal length. The result of this study showed that the renal length was significantly related to height.
This study has the limitation because of the narrow age range and small sample size of the subjects, not the representative of all children. In addition, the data was obtained by DMSA and US from the patients under the impression of UTI. It should be followed that further studies including all age group of normal children with advanced technique such as MRI, and also measuring volume is needed.
This study showed that the renal length as a surrogate of organ growth, is significantly correlated with age, weight, height, BSA, Rohler index, in growing children. We concluded that height seems to be the most important contributing factor for the renal growth. Further studies to evaluate adequate organ growth during childhood should be followed.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


