

Introduction
Children have a natural tendency to explore objects with their mouths, which can result in foreign body ingestion. Many cases of ingestion of foreign bodies are noted in children between 6 months and 3 years of age1). Most of the foreign objects that are passed down to the stomach or to more distal sites are spontaneously excreted in feces without treatment. However, foreign bodies sometimes cause obstruction or perforation of the gastrointestinal tract, necessitating surgical intervention2). Here, we report the first Korean case of duodenal perforation resulting from an ingested lollipop stick.
Case report
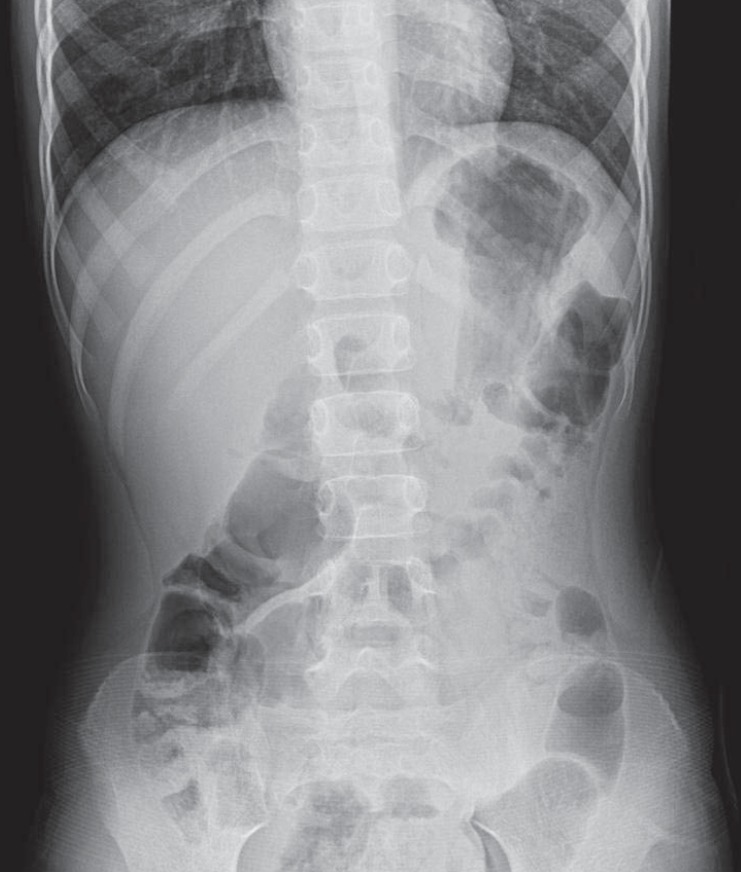
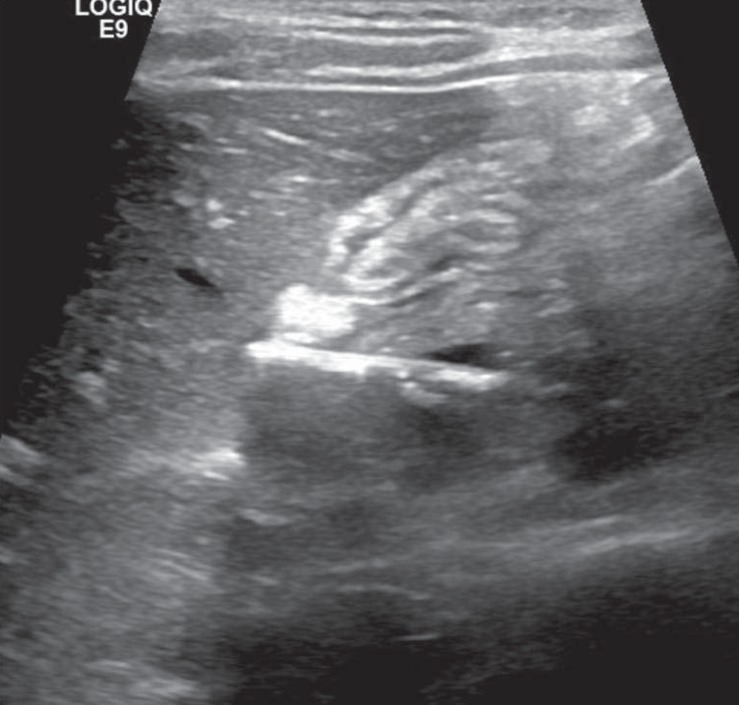
A six-year-old girl with no previous history of medical problems or surgery was admitted to the emergency department of our hospital with a two-day history of diffuse abdominal pain, nausea and vomiting. Physical examination of the febrile patient (38.8℃) was unremarkable except for moderate right-upper quadrant abdominal tenderness. Laboratory findings revealed moderately increased white blood cell count (20,710/µL; reference range, 4,000 to 11,000/µL) and C-reactive protein level (6.95 mg/dL; reference range, 0 to 0.3 mg/dL). Hemoglobin, platelet count, total bilirubin, aminotransferases, amylase, lipase, creatinine, and urinalysis were within reference ranges. Chest and plain abdominal X-ray examinations were unremarkable (Fig. 1). Abdominal ultrasonography showed a tubular echogenic structure in the second portion of the duodenum with the possibility of duodenal penetration and adjacent omental fatty infiltration associated with right-side peritonitis (Fig. 2). The computed tomography scan also identified a linear foreign body of about 10 cm with internal air contents in the duodenum (Fig. 3). The patient denied foreign body ingestion.
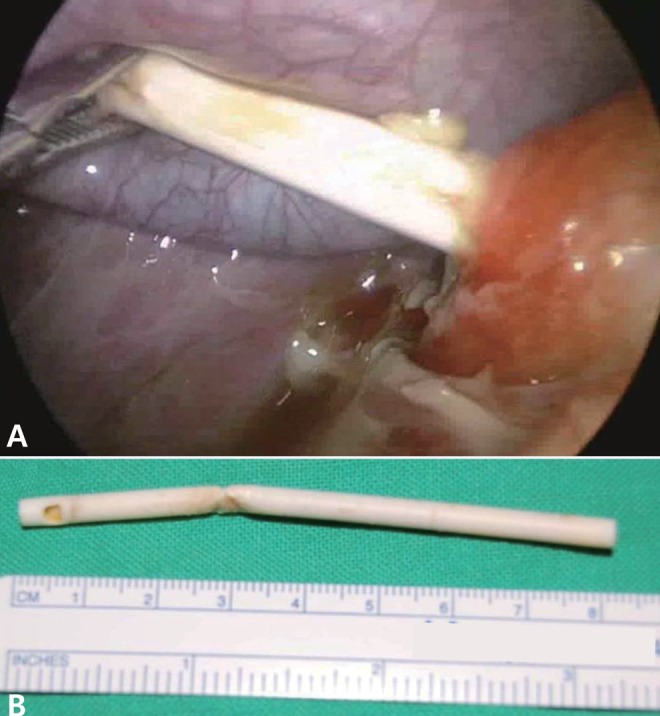
Considering the patient's stable general condition, we chose to perform a laparoscopic examination to assess the status of the perforation site and surrounding tissues. Using an umbilical 5-mm port, two 3-mm ports at the upper midline, and a fourth 5-mm port in the subxiphoid area, we found a lollipop stick perforating the second portion of the duodenum and evidence of peritonitis. The stick was easily discernible and extracted from the duodenal lumen through the perforation (Fig. 4). The biliary tree was undamaged. The perforation was closed in a single layer using 4/0 absorbable monofilament (Monosyn) and later reinforced with an omental patch. The peritoneal cavity was lavaged with saline. We performed intraoperative upper gastrointestinal endoscopy with a pneumatic test and found no evidence of leakage. We inserted a closed drain in the right upper quadrant of the subdiaphragmatic area.
The postoperative course was uncomplicated. The patient resumed oral intake on the seventh postoperative day and was discharged from the hospital ten days after surgery.
Discussion
Foreign object ingestion is a common clinical problem in young children. Commonly ingested objects are coins, toy parts, jewelry, button-type batteries, needles and pins, as well as fish and chicken bones3). The majority of ingested foreign bodies pass uneventfully through the gastrointestinal tract4). However, in some patients, the ingested foreign body causes impaction, perforation, or obstruction. Perforation occurs in less than 1% of ingestion of a foreign body3). Perforation of the gastrointestinal tract may be associated with a considerably high mortality and morbidity. Gastrointestinal tract perforation may cause peritonitis, abscess formation, inflammatory mass formation, obstruction, fistulae, and hemorrhage5). Most deaths in patients with foreign body perforation of the gastrointestinal tract are due to fulminant sepsis6). Therefore, efforts should be made to remove the ingested foreign bodies if they cannot pass through the gastrointestinal tract spontaneously.
The most common sites of intestinal perforation by a foreign body are the ileocecal and rectosigmoid regions7). Duodenal perforation because of ingested foreign objects is relatively uncommon8). Clinical presentations vary, depending on the site of perforation and the extent and duration of peritonitis4). As most young pediatric patients usually do not remember the foreign body ingestion, the final diagnosis is frequently delayed. Non-radio-opaque foreign bodies are especially difficult to detect on plain radiographs of the abdomen. Computed tomography scans and ultrasonography may help clinicians in this challenging situation; however, in most patients, the diagnosis is not confirmed until surgical intervention.
In this case, the lollipop stick was entrapped in the duodenal sweep and resulted in perforation of the duodenum. The retroperitoneal, relatively immobile, and rigid nature of the duodenum as well as its deep transverse rugae and sharp angulations make it a common site for the entrapment of long and sharp-ended objects9). Objects longer than 6 to 10 cm have difficulty in passing the duodenal sweep10). Therefore, in cases of unsuccessful endoscopic removal of gastric foreign bodies that are longer than 6.0 cm, surgical removal should be considered. Compared with traditional surgical treatments, laparoscopic removal of a foreign object is less invasive and is associated with minimal postoperative pain, a faster return to normal activities, and better cosmetic outcome6).
This is the first Korean case report of duodenal perforation resulting from an ingested lollipop stick. Lollipops are popular among the pediatric population, and they are accessible to children because most parents are not aware of their potential risks. Pediatric clinicians should be aware of the risk associated with lollipop stick ingestion. Our report also suggests the feasibility and safety of laparoscopic diagnosis and treatment for pediatric patients with peritonitis induced by the ingestion of foreign bodies.

 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


