




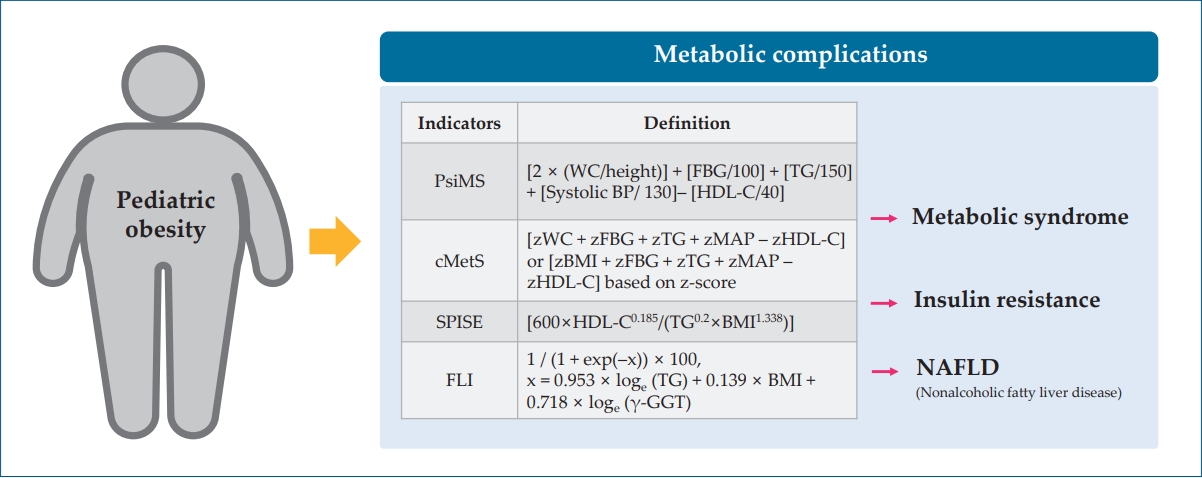
Graphical abstract. PsiMS, pediatric simple metabolic syndrome score; WC, waist circumference; FBG, fasting blood glucose; TG, triglyceride; BP, blood pressure; HDL-C, high-density lipoprotein cholesterol; cMetS, continuous metabolic syndrome; MAP, mean arterial pressure; SPISE, single-point insulin sensitivity estimator; FLI, fatty liver index; BMI, body mass index; γ-GGT, gamma-glutamyl transferase.
Introduction
The incidence of pediatric obesity has increased over the past few decades. From 1975 to 2016, the age-standardized mean body mass index (BMI) of children and adolescents reportedly increased globally per decade by 0.32 kg/m2 for girls and 0.40 kg/m2 for boys [1]. The prevalence of pediatric obesity continues to rise, and this problem has been exacerbated during the coronavirus disease 2019 pandemic. Since the pandemic, the prevalence of overweight and obesity among school-aged children, derived from Korea’s National School Health Examination, increased from 25.8% to 30.8% [2]. This phenomenon has also been observed in the US [3,4] and Europe [5]. Furthermore, an emerging problem in pediatric obesity is the increase in severe obesity, which has become a major public health concern. A recent systematic meta-analysis of 9 million children and adolescents found a 1.7-fold increase in severe pediatric obesity compared to the early 2000s [6].
Obesity can occur even in preschoolers. According to a World Health Organization report, an estimated 39 million children under 5 years of age were overweight and obese in 2020; half of the children were living in Asia [7]. Epidemiological studies revealed that obesity in early life is associated with obesity in adulthood [8]. Childhood obesity not only leads to lifelong obesity but also results in various metabolic complications throughout life. Indeed, early-onset chronic diseases, such as type 2 diabetes mellitus (T2DM) and nonalcoholic fatty liver disease (NAFLD), have been observed in obese children and adolescents [9-11]. Accordingly, the need for an appropriate evaluation of pediatric obesity and the importance of early intervention for its prevention and management have been emphasized [12]. In addition, obesity defined by BMI cannot fully explain health risks; therefore, other concepts were introduced to define obesity.
This review article discusses studies that have evaluated the complications associated with pediatric obesity and introduces the concept of sarcopenic obesity (SO). Finally, it reviews health screening programs for children in Korea.
Metabolic complications associated with pediatric obesity
1. Pediatric obesity associated with metabolic complications
Pediatric obesity is associated with a high risk for a wide range of metabolic, mental, respiratory, joint, and reproductive problems [13]. Metabolic complications related to pediatric obesity have been reported by several studies.
A few studies using cohort data have reported that obesity in children and adolescents is associated with metabolic complications, and early research focused primarily on the disease risk in adulthood. Metabolic complications are known risk factors for later cardiovascular disease (CVD), and several cohort studies have shown that childhood obesity is associated with CVD-related mortality [14,15]. Due to the long observation period required, few longitudinal studies have directly assessed the association between childhood obesity and CVD in adulthood [16]. However, evidence has accumulated that the progression of atherosclerosis, a major cause of CVD, begins early in life [17] and that childhood obesity and related metabolic complications can accelerate atherosclerosis [18,19]. The International Childhood Cardiovascular Cohort Consortium, which analyzed four cohorts (Bogalusa Heart Study, Muscatine Study, Childhood Determinants of Adult Health, and Young Finns Study), found that overweight or obese children who remained obese into adulthood were at an increased risk of type 2 diabetes mellitus (relative risk [RR], 5.4; 95% confidence interval [CI], 3.4–8.5), hypertension (RR, 2.7; 95% CI, 2.2–3.3), hypo-high-density lipoprotein (HDL) cholesterolemia (RR, 1.8; 95% CI, 1.4–2.3), high triglyceride (TG) levels (RR, 3.0; 95% CI, 2.4–3.8), and carotid atherosclerosis (RR, 1.7; 95% CI, 1.4–2.2) [20].
We reasonably expect that metabolic complications such as insulin resistance (IR), hypertension, and dyslipidemia will increase further with childhood obesity rates and that early and long-term exposure to these metabolic disorders will contribute to early CVD in an increasingly young adult population [21]. Recently, as metabolic diseases observed in adulthood have been increasingly recognized in adolescence, the focus of disease susceptibility assessments has shifted from adulthood to childhood and adolescence. Population-based cross-sectional studies of adolescents found that overweight and obese status are more likely to involve high blood pressure, high fasting glucose levels, and abnormal lipid profiles, even at a young age [22-24]. Although international consensus is lacking on the screening and monitoring of pediatric NAFLD, it is a major chronic liver-related disease that occurs frequently in children and is considered a metabolic complication associated with obesity. Obesity plays a crucial role in NAFLD progression by increasing oxidative stress and mitochondrial dysfunction [25]. A systematic review reported that the prevalence of NAFLD in overweight and obese children was 34.2% (95% CI, 27.8%–41.2%), and the risk of NAFLD was 13.4 times (95% CI, 9.1–18.0) higher in overweight and obese than in normal-weight children [26].
From a longitudinal perspective, a study of data from the Ewha Birth and Growth Study identified the trajectory of childhood BMI from 3 to 12 years and found those with a high BMI at an early age were more likely to have a high BMI throughout childhood [27]. Childhood obesity caused by genetic, lifestyle, and environmental factors can occur even in the early stages of life and seriously affect the occurrence and progression of metabolic diseases. Disease susceptibility can be observed during childhood and adolescence; therefore, early assessments and interventions are encouraged.
2. Metabolic complications assessment index
Unlike adults, for whom the diagnostic criteria for diseases are well defined, the consensus is inconsistent on the definition of metabolic diseases in children because of the relatively low prevalence in children. Nevertheless, many studies have suggested various indicators to evaluate an individual’s susceptibility to metabolic diseases, and only a few are introduced here (Table 1) [28-32].
In 2017, Vukovic et al. [28] developed the pediatric simple metabolic syndrome score (PsiMS), a modified metabolic syndrome (MetS) scoring system based on the simple metabolic syndrome score originally developed for adults. This index can be easily calculated, and its usefulness was confirmed in a study of Korean adolescents (area under the curve [AUC], 0.958) [33]. The continuous metabolic syndrome score (cMetS)is a reliable indicator for predicting the risk of MetS in children and adolescents. It is a more comprehensive and robust measure than dichotomous measures of MetS, thus allowing for better evaluations in pediatric epidemiological studies [29,34]. A systematic review noted that cMetS is useful for predicting the risk of MetS with high accuracy [35].
The single-point insulin sensitivity estimator (SPISE) is an index that was developed to simplify the estimation of insulin sensitivity in adults and obese adolescents [30]. TG/HDL-cholesterol(HDL-C)was introduced approximately 20 years ago as an index for evaluating IR; however, it showed high variability among populations, suggesting the need for a cutoff point [36]. To improve its performance, Paulmichl et al. [30] developed the SPISE as a promising tool for estimating IR based on TG, HDL-C, and BMI. In adolescents aged 16–17 years, SPISE showed significantly better AUC values than the homeostatic model assessment for IR (HOMA-IR) and TG/HDL-C in discriminating MetS [37]. Finally, the fatty liver index (FLI) and hepatic steatosis index are primarily used as noninvasive/nonimaging indicators to define pediatric and adult NAFLD [31,32]. In the United States, an FLI for a multiethnic population was developed [38]. Although these indicators are used in epidemiological studies, evidence assessing the usefulness of the FLI and hepatic steatosis index in pediatric populations is lacking, and further evidence is required.
3. Studies using metabolic complication assessment indicators
These indicators have been used in several studies to evaluate the metabolic complications of pediatric obesity. In a study of adolescents (10–18 years) using the Korea National Health and Nutrition Examination Survey (KNHANES) data, mean PsiMS was significantly higher in MetS than in non-MetS participants (3.2 vs. 1.9 in boys, 3.1 vs. 1.8 in girls; all P<0.001) [33]. In a cross-sectional cohort study of 2,107 overweight or obese children and adolescents (aged 5–18.4 years), participants in the lowest versus highest quartile of SPISE values were three times more likely to develop dysglycemia during follow-up [39]. Similar findings were observed in a study of 10–17-year-olds in which the SPISE index was significantly lower in MetS than in non-MetS participants (5.5 vs. 9.4 in boys and 4.4 vs. 8.6 in girls; all P<0.001) [40]. Additionally, in the International Childhood Cardiovascular Cohort Consortium (average follow-up, 22.3 years), cMetS in childhood was associated with a 2.1-fold higher risk of MetS in adulthood [41]. The cMetS remained stable throughout childhood [42]. NAFLD is often asymptomatic and can lead to irreversible complications, highlighting the importance of early diagnosis to prevent progression. The global prevalence of NAFLD is 4.2%–9.6% and can reach 38% in pediatric obese populations [43]. In a study of overweight and obese children aged 5–15 years, those with an ultrasound-diagnosed fatty liver had significantly higher FLI values than those without a fatty liver (odds ratio, 3.5; 95% CI, 1.1–11.3) [39]. These indicators provide valuable insight into the metabolic complications associated with childhood obesity and aid in the early identification and intervention to prevent long-term health consequences.
Changes in evaluation perspective for pediatric obesity
1. BMI as proxy for body composition
Obesity refers to the excessive accumulation of fat caused by an imbalance between energy intake and expenditure. Body weight comprises two components: body fat mass (FM) and fat-free body mass (FFM). BMI, a simplified measure commonly used to define obesity, was determined based on height and weight. However, although BMI can reflect high FM levels, it also includes individuals with naturally high FFM, limiting its ability to assess obesity accurately [44]. Furthermore, although obesity may be visually classified based on BMI, metabolic health levels can vary. Evaluating metabolic health using BMI alone may have limitations in distinguishing functional differences [45]. In children and adolescents, a BMI increase may not simply indicate an increase in FM, as body composition changes can occur depending on growth rate and pubertal development level [45].
An example that effectively demonstrates the impact of body composition on health is the “obesity paradox,” which reveals the incorrect results that can be derived when evaluating the relationship between high BMI and low mortality rates in the elderly population-based solely on BMI. Body composition offers a better explanation for this phenomenon [46]. In studies conducted on children and adolescents, the term “normal-weight obesity” define cases in which excessive body fat and low muscle mass coexist, resulting in a normal BMI. Despite having a normal BMI, these children may experience unfavorable metabolic health [47]. In fact, they exhibit lower cardiorespiratory and muscular fitness than children with normal body fat levels. They also display physical fitness deficits similar to those of overweight children, which can be partly attributed to low physical activity levels [48]. Muscle plays a vital role in glucose and lipid metabolism and can be assessed using FFM, lean body mass (LBM), and skeletal muscle mass (SMM) [49]. However, considering muscle mass alone does not sufficiently reflect muscle quality and performance, grip strength has been used as a muscle strength indicator [50,51]. Grip strength correlates with muscle mass and body FM and has been found to be associated with metabolic risk [52] not only in adults but also in studies involving children and adolescents [53]. With the accumulation of research findings suggesting differences in health impacts based on metabolic health or body composition rather than just visual obesity, new paradigms are being proposed for evaluating obesity.
When using body composition indicators, it is imperative to consider their correlation with body size. Because a decrease in FFM can increase the proportion of fat, interpreting the meaning of body composition indicators alone can be challenging when making comparisons. Indeed, some studies have reported differences in the results depending on the evaluation criteria [44]. Some studies have presented muscle mass as a ratio of weight to height squared or calculated the ratio of muscle mass to FM to supplement the interpretation of research findings, thereby addressing these challenges.
2. Studies evaluating relationship between body composition indices and metabolic complications
Studies have reported associations between obesity and major metabolic complications such as impaired glucose metabolism, MetS, and NAFLD. Various body composition indicators are associated with these complications. Muscle is considered an essential tissue in human endocrine function and metabolism, and its involvement in glucose and lipid metabolism has been explained by various biological mechanisms [49]. In a recent systematic literature review of 15 research papers, differences in FFM or LBM were evaluated between children and adolescents with IR/glucose tolerance (GT)/MetS and those without these conditions. Children and adolescents with IR/GT/MetS exhibited lower FFM or LBM in terms of percentages. This suggests a higher proportion of adiposity in relation to body weight, indicating the influence of adiposity on IR [44]. Another systematic literature review evaluated the correlation between FM percentage and glucose metabolism in children and adolescents [54]. FM percentage showed a correlation of 0.48 with fasting plasma insulin and a correlation of 0.44 with HOMA-IR based on data from 11 studies.
NAFLD is recognized as a major chronic disease in the pediatric population and is understood as a condition that is not simply limited to liver abnormalities but also involves various metabolic risks [55]. In a study evaluating the association between muscle mass and NAFLD risk in overweight children and adolescents, a lower muscle mass was associated with a higher risk of NAFLD, while an inverse relationship was noted between muscle mass and nonalcoholic steatohepatitis as evaluated through biopsy [56]. Furthermore, in a study that assessed the grip strength to body weight ratio and considered muscle strength, differences were observed based on the presence of MetS, with a lower grip strength/body weight ratio observed in adolescents with MetS [50]. Studies focusing on obese children have also used muscle-to-fat ratio (MFR) to predict the risk of metabolic disorders [57].
Abdominal fat accumulation during childhood and adolescence may be directly associated with unfavorable cardiovascular and metabolic health profiles irrespective of overall body fat levels [58]. The prospective study conducted by Park et al. [59] evaluated the association between SO at ages 7–9 years and cMetS at ages 13–15 years. Children with SO had higher cMetS during adolescence than those without SO; this trend was consistent in the evaluation of other MetS indicators. Furthermore, being overweight during childhood and adolescence had a positive interaction effect on adolescent metabolic health. As evidence suggests the limitations of BMI in explaining health effects, there is growing recognition of the need to evaluate body composition and alternative indicators to assess health outcomes.
3. Definition and prevalence of SO
A high BMI is associated with various metabolic health outcomes. However, individuals with the same body weight do not always experience the same health effects. Additionally, the impact of muscle mass on IR and lipid metabolism may vary depending on the FM index [49]. SO, which refers to the coexistence of muscle loss and obesity, has been linked to various metabolic disorders [60]. MFR calculations are commonly used to define SO using appendicular skeletal muscle mass or SMM [51,61]. The handgrip strength-to-BMI ratio is another indicator used to evaluate SO [51]. However, a consistent definition of SO in children and adolescents is lacking, leading to the use of various criteria in different studies to estimate its prevalence. The reported prevalence is 5.7%–32.1% in the general population and 20.2%–84.4% in overweight and obese populations (Table 2) [51,56,59,61-67].
4. Need for new definition of obesity, including body composition
Computed tomography and magnetic resonance imaging are accurate methods for measuring body composition. However, owing to their high cost and limited accessibility, bioelectrical impedance analysis and dual-energy x-ray absorptiometry are becoming more commonly used to assess body composition. In addition, grip strength has been suggested as a low-cost and easily measurable indicator of body composition. McCarthy et al. [62] proposed using MFR as an indicator of metabolic health in children and suggested cutoff points to define SO. Subsequently, regarding the diagnostic criteria for pediatric/adolescent SO, Kim et al. [61] applied the method proposed by McCarthy et al. [62] to domestic research and utilized KNHANES data to make suggestions. However, specific criteria based on sex and age are necessary during the growth period, and consideration should be given to the onset of puberty owing to differences in adipocyte composition [68]. Therefore, standardized measurement methods are required to define SO, and the development of national-level criteria is required.
National Health Screening Program for children in Korea
Health screening programs are important for the early detection of diseases or conditions and the prevention of chronic diseases. In Korea, the National Health Screening Program (NHSP) for adults was initiated in 1980, and the target population and diseases are expanding as health demands change in society [69]. The NHSP for children was started in 2007 to monitor the growth and development of infants and children under 6 years of age and is conducted eight times from 14 days after birth. This program consists of physicians administering physical examinations, anthropometric measurements, health education, oral examinations, and developmental evaluation [70]. However, there are limitations in assessing physical and cognitive development, excluding laboratory tests that can assess metabolic health.
Through the National School Health Examination, students in certain grades (1st and 4th grades of elementary school, 1st grade of middle and high school) receive health examinations at schools or hospitals under Ministry of Education supervision. However, screening blood tests for obesity complications are only performed on overweight students except for 1st graders in elementary schools. Despite the high risk of obesity-related complications, opportunities for intervention and treatment may be lost. Moreover, out-of-school youths were excluded [71]. Therefore, establishing a system that connects doctors and schools and provides timely feedback is an urgent health issue for early intervention in obesity.
The NHSP includes BMI measurements for all children and adolescents who undergo routine checkups. BMI is generally used as a screening and diagnostic tool for detecting obesity because it is easy to use and inexpensive. Meanwhile, body fat percentage may be very different even if the BMI is the same, and the amount of FM can increase the risk of MetS independent of BMI. Therefore, to detect obesity complications early, national examinations of children and adolescents should include body composition and laboratory tests to evaluate metabolic health rather than measuring body height and weight.
The critical periods in pediatric obesity are reportedly gestation, early infancy, the adiposity rebound period, and adolescence. Adiposity rebound refers to an increase in BMI following the minimum BMI in early childhood in the preschool period [72]. The earlier the timing of adiposity rebound, the higher the probability of obesity and metabolic complications [73]. Disease susceptibility can be observed at an early age, and lipid abnormalities such as high TG and low HDL-C levels have been reported in obese children under 10 years of age [74,75]. Furthermore, the American Academy of Pediatrics guidelines recommend that pediatricians evaluate hypertension by measuring the blood pressure of overweight children during adolescence at every visit starting at 3 years of age [76]. Recent studies demonstrated that lifestyle changes are effective even in preschoolers aged 2–5 years [77,78].
Healthcare providers and physicians who conduct the NHSP should encourage children to engage in healthy behaviors and lifestyle treatments. Moreover, based on BMI classification, laboratory evaluations can be performed in clinically indicated children. Laboratory tests for metabolic complications should begin before 10 years of age [76]. For obese children 2–9 years of age, screening for dyslipidemia may be included. Children 10 years and older with overweight status should be evaluated for glucose metabolism and liver function for the detection of IR or NAFLD. Early detection and treatment in these populations can reduce future complications of obesity and motivate treatment engagement.
Conclusion
Pediatric obesity is a major public health issue because early-onset obesity and its complications can increase one’s risk of metabolic disorders and CVD in later life. Various indicators have been proposed to screen for obesity-related metabolic complications, and evaluating these indicators is possible even at a young age. This finding suggests a new paradigm for assessing obesity rather than BMI to evaluate health appropriately. Expanding health screening and laboratory tests can promote the early detection and intervention of obesity-related metabolic complications, ultimately reducing long-term complications.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


