

Introduction
Streptococcus pneumoniae is a major pathogen, causing otitis media, sinusitis, pneumonia, bacteremia, and meningitis in children worldwide. It also offers some threat of mortality, mostly in developing countries1,2). The recent spread of antibiotic-resistant S. pneumoniae strains has caused considerable concern3,4). Pneumococcal conjugate vaccines (PCVs), used since 2000, have been shown to reduce the incidence of vaccine-serotype invasive pneumococcal disease (IPD) and nasopharyngeal (NP) colonization of pneumococcus by the vaccine serotypes3,5-11). In spite of the availability of these efficient vaccines, pneumococcal infections remain a global problem due to the emergence of resistance and replacement by nonvaccine-serotype strains12,13).
Pneumococcal infections are traditionally diagnosed using bacterial culture combined with biochemical or immunochemical identification tests. However, conventional culture methods take at least 48 hours to obtain results, and antibiotic treatment prior to obtaining patient specimens or autolysis of pneumococci during transportation of samples may cause false-negative culture results. In addition, the current determination of serotypes by serological methods requires isolation of pneumococci, is time consuming and expensive, and the results are difficult to interpret. Rapid and precise methods of detection and serotyping of S. pneumoniae are needed to improve the diagnosis of IPD, but they are also essential for predicting the consequences of vaccinations on NP carriage. In this study we aimed to compare PCR with traditional culture isolation methods for detecting S. pneumoniae in NP aspirates and to improve the design of previously published protocols for sequential multiplex PCR-based serotyping of pneumococci according to the predicted distribution of pneumococcal serotypes in Korea.
Materials and methods
1. NP secretions
A total of 842 NP secretions were collected from children (younger than 5 years of age) hospitalized with lower respiratory infections at Severance Children's Hospital in Seoul, Korea, from March 2009 to June 2010. The NP aspirates obtained by suction were divided into two samples: one was used for bacterial culture and the other for multiplex PCR-based serotyping. Informed consent was obtained from the parents or guardians of the patients prior to the collection of samples. The study was approved by the institutional review board of Severance Hospital.
2. Bacterial culture
A portion of each of the NP specimens was cultured on blood agar plates for 48 hours at 37℃ in an atmosphere enriched with 5% CO2. Isolates were identifiedas S. pneumoniaee by typical colony morphology, alpha-hemolysis, negative catalase reaction, Gram-positive staining, optochin disk sensitivity, and bile solubility.
3. Multiplex PCR-based serotyping
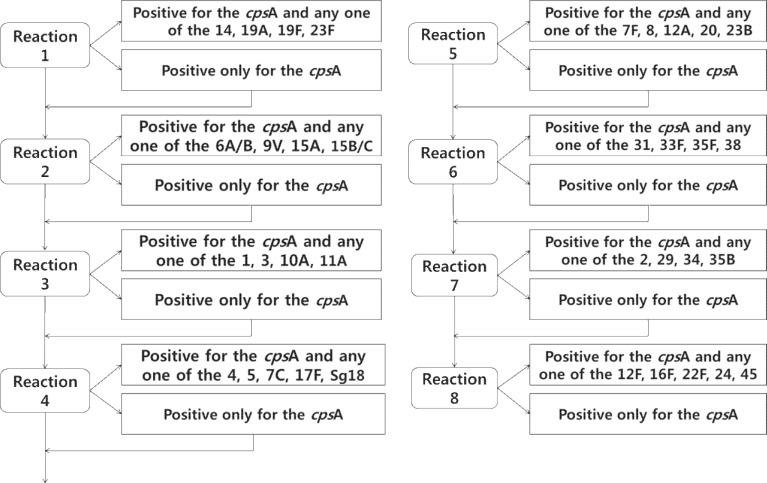
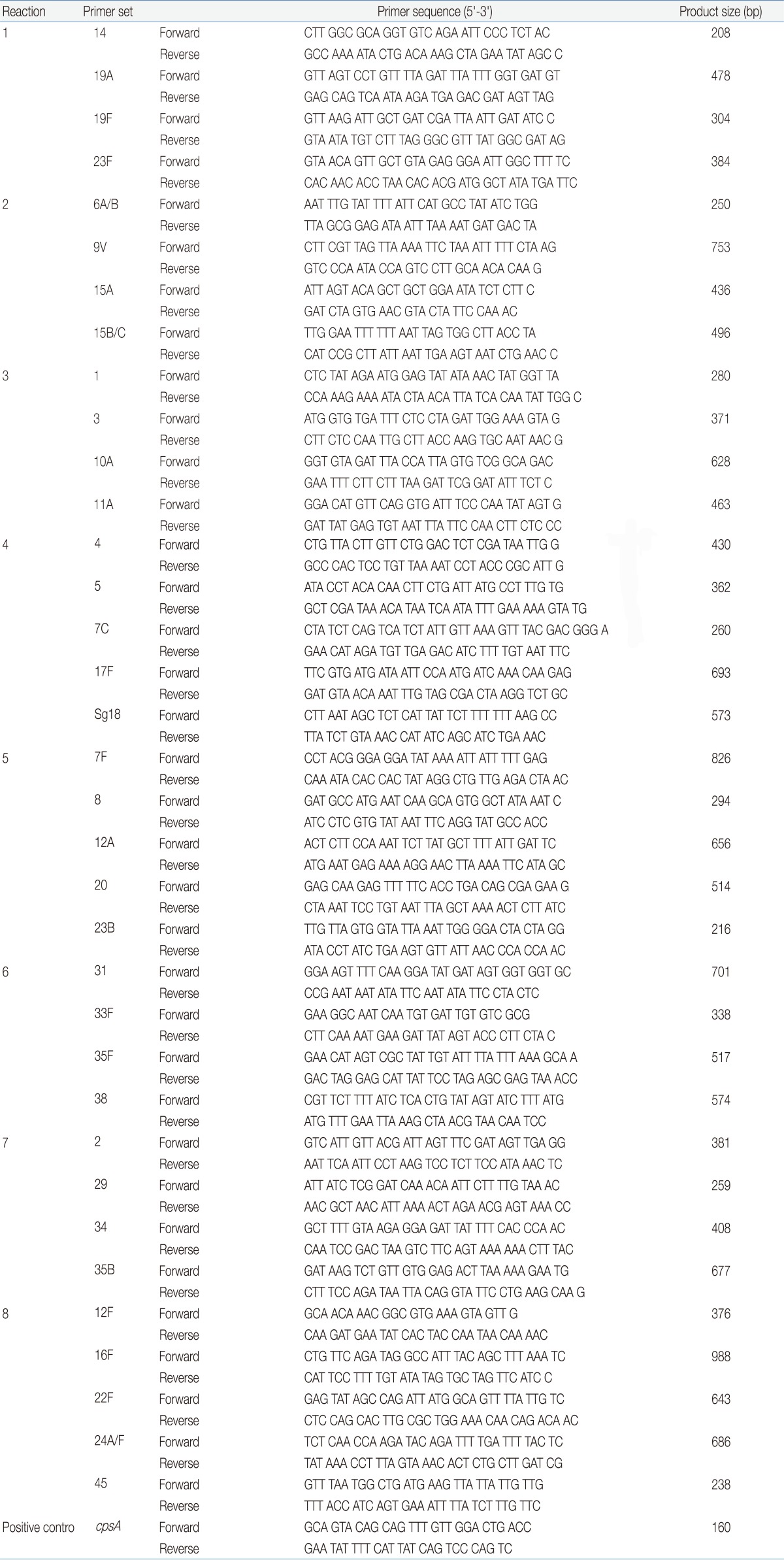
Nucleic acid from each NP specimen was extracted using a QIAamp Genomic DNA kit (Qiagen, Valencia, CA, USA) according to the manufacturer's protocol. The extracted DNA suspension was kept frozen at -70℃ until further use. Thirty-five serotype-specific primer pairs were designed as described in published reports (Table 1)14-16). A primer pair targeting cpsA found in all 90 known pneumococcal serotypes was used as the positive control. The primers were grouped into eight sets for sequential testing (Fig. 1) based on the ranking of serotypes that are frequently detected in South Korea17-19). PCR for 35 serotypes were performedon all samples to check the status of co-colonization. PCR mixtures consisted of 12.5 µL 2× multiplex PCR Pre-Mix, 3.5 µL purified DNA, primers at concentration of 1 µm, and cpsA-f and cpsA-r primers at a concentration of 0.5 µm in a 25 µL reaction volume. Amplification conditions for all reactions were as follows: initial denaturation at 94℃ for 4 minutes; 30 cycles at 94℃ for 45 seconds, 54℃ for 45 seconds and 65℃ for 2 minutes 30 seconds; and a final extension cycle of 72℃ for 5 minutes. The PCR products were analyzed by gel electrophoresis on a 1.4% agarose gel at 120 volts for 45 minutes, stained with ethidium bromide, and visualized with ultraviolet transillumination.
Results
1. Comparison of PCR and bacterial culture results for identification of S. pneumoniaee
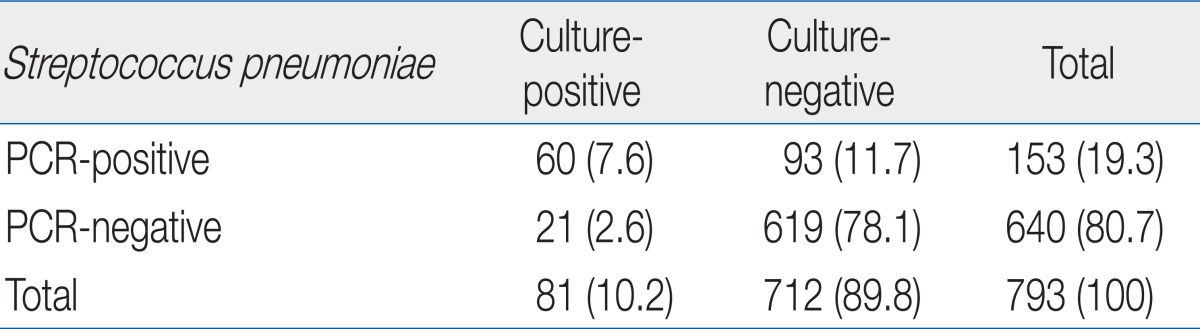
Among the 842 total cases, 793 underwent simultaneous bacterial culture and PCR analysis for pneumococcal isolation, while 49 were only analyzed by PCR. Bacterial culture yielded positive results in 10.2% (81/793) cases and PCR in 19.3% (153/793). Both methods revealed identical results in 85.6% (679/793) of tests. Among 14.4% (114/793) that showed different results, 11.7% (93/793) showed negative results with culture and positive results with PCR, and 2.6% (21/793) showed positive results with culture and negative results with PCR (Table 2).
2. Distribution of pneumococcal serotypes
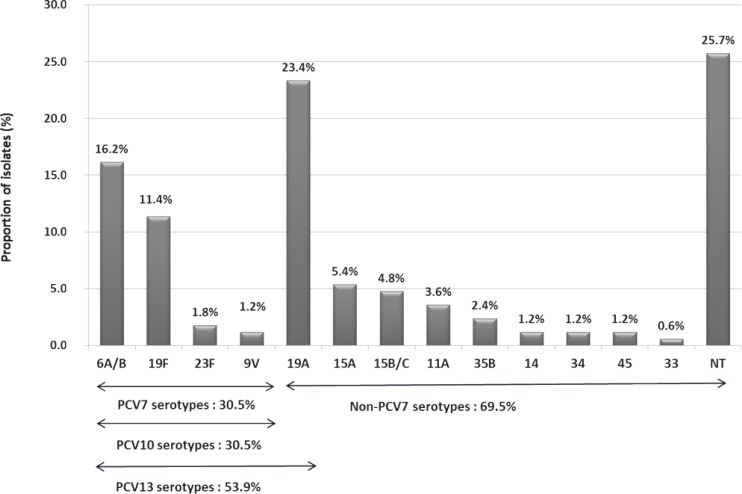
Among the total 842 specimens, 163 were positive by PCR analysis. In total, 163 PCR-positive samples and 4 co-colonization strains were analyzedfor serotyping. A total of 13 different S. pneumoniae serotypes could be identified, and 43 pneumococcal strains were non-typeable (26%). The most frequent serotypes were 19A (n=39, 23%) and 6A/B (n=27, 16%), followed by 19F (19, 11%), 15A (n=9, 5%), and 15B/C (n=8, 5%). These five serotypes together accounted for 61% of overall isolates. Among all isolates, 30.5% were the serotypes included in PCV7, and 69.5% were non-PCV7 vaccine types (Fig. 2).
Discussion
In this study, multiplex PCR was used to detect pneumococci and to determine pneumococcal serotypes among 842 total cases. Of the total samples, 793 underwent simultaneous bacterial culture and PCR analysis, with a concordance of 85.6%. The detection rate of pneumococcal strains by multiplex PCR (19.3%) was higher than that by bacterial culture (10.2%). PCR analysis based on the amplification of cpsA or other pneumococcal genes has been shown to be sensitive and efficient in detecting pneumococcus in clinical samples16,20-23). Virolainen et al.20) found 18% of middle ear fluid specimens to be positive by culture and 30% by culture and PCR. Saha et al.16) showed that sequential multiplex PCR of 127 culture-negative cerebrospinal fluid samples yielded serotypes for 51 additional cases. Our results are consistent with those of previous studies in this field. In the present study, although 2.6% of samples showed positive results in culture but negative by PCR, these are thought to be the result of operator error and will likely be reduced by increased operator experience.
In addition to detection of pneumococci, accurate serotype determination is important for vaccine development. Presently the choice of vaccine strains depends on serotype prevalence patterns. Although serological determination by a quelling reaction of pneumococcal cells with antipolysaccharide sera is the currently used method for pneumococcal serotyping24,25), the high cost of antisera, the requirements for technical expertise, and subjectivity in interpretationof results are major shortcomings of the procedure14,16). Multiplex PCR has the potential to overcome these drawbacks and has been reported to have higher sensitivity and specificity than traditional quelling reaction methods14,16,26,27).
Because the serotype distribution among NP carriage isolates varies by geographic region, time, and age-group, we designed primers and modified the sequential multiplex PCR scheme based on the distribution of serotypes that were frequently isolated in Korea17-19). Among the serotypes identified in our study, the most common serotype was 19A, followed by: 6A/B, 19F, 15B/C, 15A, 11A, and in a small minority 35B, 23F, 14, 9V, 45 and 33. In Korea, PCV7 has been available since November 2003 and PCV10 and PCV13 were introduced in May 2010. Thus, our results, obtained from March 2009 to June 2010, represent the impact of PCV7 on NP carriage of pneumococcus. Several studies conducted in Korea prior to the use of PCV7 demonstrated that the proportion of PCV7 serotypes in invasive and noninvasive isolates, including carried strains, was 54 to 72% and 57 to 83%, respectively17-19,28,29). Our study revealed that PCV7 serotypes decreased to 30.5% of carried serotypes over the course of this study period, indicating a replacement phenomenon in NP carriage after the introduction of PCV7.
As PCV10 or PCV13 have only recently been introduced, there will likely be changes in serotype distribution among pneumococcal carriage isolates in the future. Surveillance of pneumococcal serotypes should be continued in order to monitor changes in serotype distribution necessary for the pneumococcal vaccine policy. To that end, our multiplex PCR system can be used as an accurate and rapid way of isolating and serotyping S. pneumoniae compared to conventional microbiology culturing. However, our study had an important limitation; 26% of total isolates were non-typeable because only 35 primer sets for pneumococcal serotyping were used in the protocol. In the future, new serotype-specific primers will need to be added, so that more serotypes may be detected. This will enhance detection and serotyping of S. pneumoniae when using multiplex PCR.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


