




Introduction
Early childhood is the most important stage of a human’s life because mental and physical developments occur in this time period. Undernutrition in this stage can have irreversible effects on children’s growth and educational performance. Additionally, it could increase the risk of dying from infectious diseases [1]. Although reducing mortality rate among children below 5 years old was one of the main targets of the Millennium Development Goals, child mortality has remained a great concern worldwide especially in developing countries (the rate dropped from 90 to 43 deaths per 1,000 live births worldwide and from 100 to 47 deaths per 1,000 live births in developing countries between 1990 and 2015) [2].
Malnutrition refers to a condition that occurs when the body does not receive nutrients, resulting in acute or chronic deficiency or imbalance in energy, protein, and other nutrients [3-5]. Malnutrition is the main cause of mortality and morbidity among children below 5 years old; furthermore, this condition affects the physical and cognitive developments of children and reduces their academic performance [1]. Wasting and underweight are two main indicators of undernutrition in children [6]. The term underweight in children refers to a child whose weight for age is less than -2 standard deviation (SD) of the World Health Organization (WHO)’s child growth standard median [7]. In addition, the term wasting in children refers to a child whose weight for height is less than -2 SD of the WHO’s child growth standard median. Wasting refers to acute undernutrition, while underweight refers to acute and chronic malnutrition [7]. In 2013, the global prevalence rates of wasting and underweight among children below 5 years old were 8% and 15%, respectively [8]. The prevalence rates of wasting and underweight among Asian children were 10.1% and 19.3%, respectively [9]. The Millennium Development Goals report in 2015 stated that the worldwide prevalence of underweight decreased from 25% to 15% from 1990 to 2015; however, this decrease was not fast enough to reach the target [10]. In 2016, wasting continued to threaten the lives of 52 million children below 5 years old, which accounted for 7.7% of the total children below 5 years old in the world. In the same year, it was reported that over two-thirds of the wasted children were living in Asia [11].
Residing in rural areas, living in large family structure, poverty, low parental education, infections, socioeconomic status (SES), and living in developing countries are the main contributors to malnutrition [7,12,13]. With a population of almost 80 million people, 74% of which are urban dwellers, Iran is the 17th populous country in the world. Majority population of Iran is young. Adolescents below 15 years old account for nearly 25% of the population, while adults over 65 years old account for 6% of the population. The population size of children under 5 years old in Iran is almost 7 million, representing 8% of the population. Furthermore, the average annual population growth rate in the country from 2011 to 2016 was 1.24% [14,15].
Oil and natural gas along with agriculture and other industries are important contributors to Iran’s economy. Iran is the fourth producer and the fifth exporter of oil in the world. Iran is also the fifth producer of natural gas in the globe. Based on the World Bank’s criteria for classification of countries [16], with 1.485 trillion gross domestic product (GDP) per capita (GDP, purchasing power parity [constant 2011 international $]), Iran is considered as one of the upper middle-income countries [16].
To decrease the prevalence of malnutrition among children, a multisectoral nutrition program should be implemented. To evaluate this program and monitor the progress made in reaching the targets, data collection should be performed at national and subnational levels [11]. The prevalence of wasting and underweight have previously been reported in some provincial studies; in these studies, the reported prevalence rates of underweight were 2.3% in West Azerbaijani and 43.1% in North Khorasan, and the prevalence rates of wasting in children were 1.4% in West Azerbaijan and 32.2% in North Khorasan [17,18]. These studies differed in terms of design, geographical region, and age group, making it difficult to estimate the prevalence of wasting and underweight at the national level. This systematic review and meta-analysis aimed to estimate the prevalence of undernutrition at the national level in Iran.
Materials and methods
1. Search strategy
International databases including MEDLINE (PubMed), Web of Science, Google Scholar, Scopus, and CINHAL (Cumulative Index to Nursing and Allied Health Literature), as well as some Iranian databases including Scientific Information Database (www.sid.ir), Iranian Research Institute for Information Science and Technology (Irandoc.ac.ir), Iranmedex (www.iranmedex.com), and Magiran (www.magiran.com) were searched for related original articles. The search was conducted in these databases without any limitations on the language from January 1989 to August 2017. The search was also performed using the seven keywords in the form of English and Persian phrases including malnutrition, protein energy malnutrition, growth disorders, underweight, wasting, weight loss, children below 5 years old, and children. All keywords were searched electronically by two Boolean operators for whom the search strategy is explained separately.
2. Inclusion/exclusion criteria
After performing the search, all the results were reviewed; then, after going through the titles, some articles were excluded from the study. The evaluation of the searched articles was performed individually by 2 reviewers based on the inclusion and exclusion criteria. The structures of the searched articles were appraised using the reconstructed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. This study included (1) cross-sectional studies; (2) articles that contain the estimated prevalence of malnutrition, growth disorders, underweight, wasting, and weight loss; and (3) articles that were conducted among children below 5 years old. The following studies were excluded articles: (1) interventional and other types of research that do not use a cross-sectional design, (2) animal articles, and (3) articles that reported on the prevalence of individuals aged more than 5 years.
3. Quality assessment and risk of bias
The quality of all of the articles was assessed using the Meta-analysis of Observational Studies in Epidemiology [19] and PRISMA checklist [20,21]. After evaluating the articles through the checklist supervised by the reviewing team, we made sure that our checklist includes the following: (1) name of first author; (2) date of publication; (3) date of when the study was performed; (4) total sample size; (5) sampling method; (6) study design; (7) sample size according to sex; (8) type of questionnaire; (9) appraisal tool score; (10) main variable; (11) prevalence of malnutrition, growth disorders, underweight, wasting, and weight loss based on the type of questionnaire; and (12) inclusion criteria.
4. Data extraction
A structured checklist was used to extract information on (1) name of first author; (2) date of publication; (3) date of performing study; (4) total sample size; (5) sampling method; (6) study design; (7) sample size according to sex; (8) type of questionnaire; (9) appraisal tool score; (10) main variable; (11) prevalence of malnutrition, growth disorders, overweight, obesity, and body weight based on the type of questionnaire; and (12) inclusion criteria. Additional information on the results was extracted based on the type of instruments.
5. Statistical analysis
A random effects model was employed to generate a pooled prevalence. The reported prevalence is presented in the form of percent with a 95% confidence interval (CI). The heterogeneity between the included studies was assessed using the heterogeneity statistic I2 and then was reported in the form of percent to indicate the extent of variation between the articles. A forest plot was also used to schematically display the results of the meta-analysis.
Results
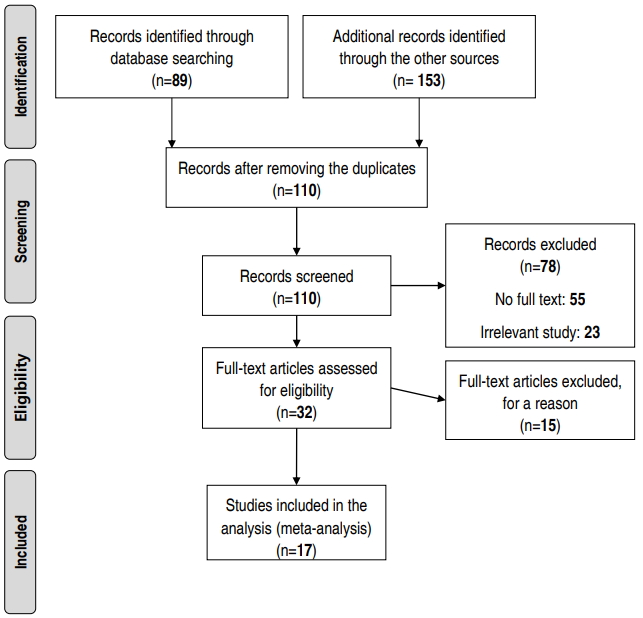
The primary search yielded 242 articles. After reviewing the titles, 132 papers were excluded due to duplication or relatedness. Approximately 110 relevant papers remained that were not duplicated. After reviewing the abstracts, 32 papers were included in the study. Then, the remaining articles were evaluated with accordance to the developed checklist and finally 15 other articles were excluded from the study (Fig. 1, Table 1). Based on the study methods (descriptive or analytical cross sectional), the articles were categorized into 2 groups.
1. Assessment of pooled prevalence
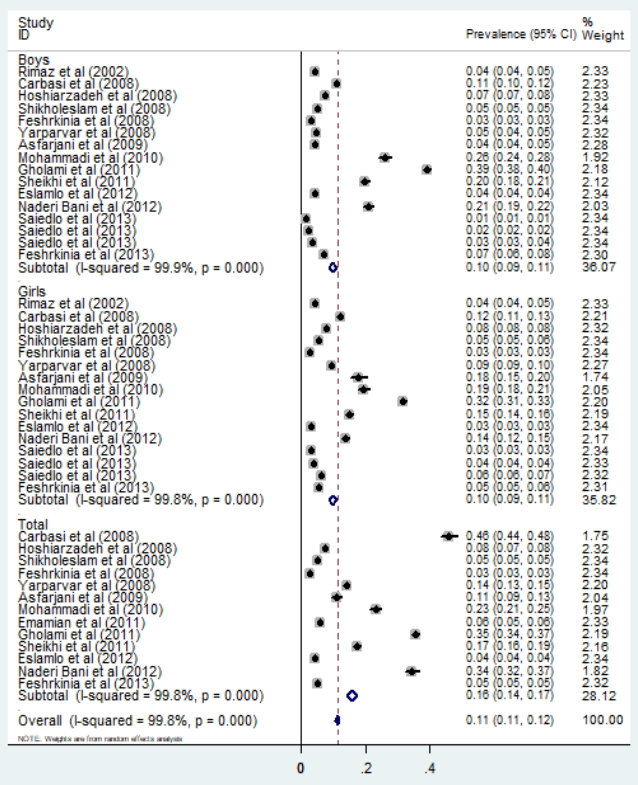
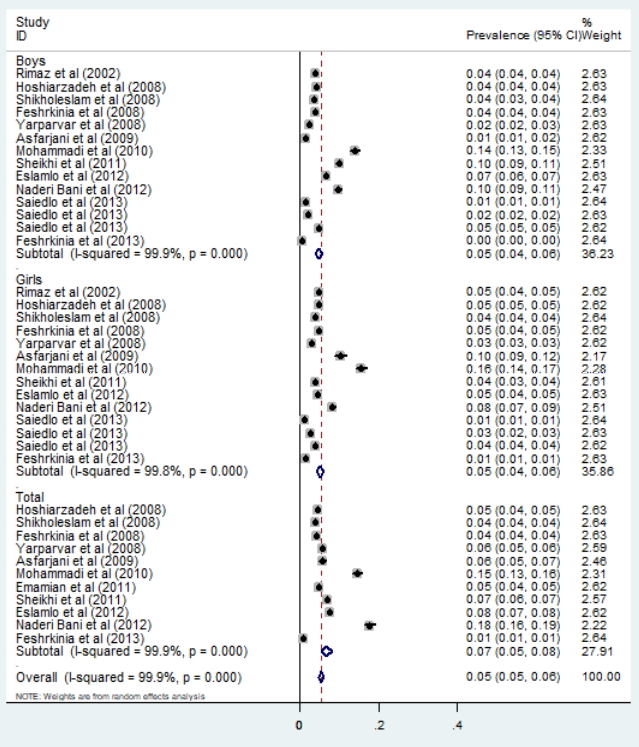
Finally, a total of 17 articles, from different settings, were included in the meta-analysis to obtain a pooled prevalence estimate. The prevalence of underweight in Iranian children was estimated to be 11% (95% CI, 11–12). A subgroups analysis of the sexes showed that the prevalence of underweight in men, women, and both were 10% (95% CI, 9–11), 10% (95% CI, 9–11), and 16% (95% CI, 14–17) respectively (Fig. 2). Moreover, the pooled prevalence of wasting in Iranian children was 5% (95% CI, 5–6) (Fig. 3). The subgroup analysis of the sexes showed that the prevalence rates in men, women, and both were 5% (95% CI, 4–6), 5% (95% CI, 4–6), and 7% (95% CI, 5–8), respectively (Fig. 3).
The results of this study showed that the prevalence rates of underweight among children in the central, western, southern, and northern areas in Iran and at the national level were 24% (95% CI, 7–41), 5% (95% CI, 4–5), 20% (95% CI, 14–26), 17% (95% CI, 4–30), and 6% (95% CI, 4–9), respectively (Table 2). In addition, the prevalence rates of wasting in the central, western, southern, and northern parts of the country and at the national level were 9% (95% CI, 4–15), 4% (95% CI, 1–7), 11% (95% CI, 3–18), 5% (95% CI, 4–6), and 4% (95% CI, 3–5), respectively (Table 2, Fig. 4).
Discussion
The results of this study showed that the prevalence rates of underweight and wasting in Iranian children were 11% and 5%, respectively. However, in another study, the prevalence rates of underweight and wasting were reported to be 5.7% and 3.29%, respectively [22]. An anthropometric nutritional indicator survey conducted on Iranian preschool children in 1998 reported the underweight and wasting to be 10.8% and 4.9%, respectively [23]. A subgroup analysis of this study showed that the prevalence of underweight among children in the central, western, southern, and northern parts of Iran and at the national level were 24%, 5%, 20%, 17%, and 6%, respectively. Furthermore, the prevalence rates of wasting in the central, western, southern, and northern parts of the country and at the national level were 9%, 4%, 11%, 5%, and 4%, respectively. Several studies carried out at national, regional, and provincial levels reported different rates of underweight and wasting among Iranian children; for example, other studies in South Khorasan and Zahedan reported higher rates of wasting and underweight. According to these studies, 43.1% of children under 6 years old in the South Khorasan province were underweight, while 32.2% of them were wasted [18]; Additionally, in the rural parts of Zahedan, 17.3% of children under 6 years old were underweight, while 6.8% of them were wasted [24]. In another study, the prevalence of underweight and wasting in the central region was reported to be higher than that of the northwest and southern parts of the country [25].
The results of the present study showed the same prevalence of overweight and wasting among men and women. These results are also consistent with the those reported in other studies carried out in Iran, indicating that there is no statistical difference in the prevalence of underweight and wasting between sexes [25,26]. However, some studies reported that the prevalence of underweight and wasting in men were higher than that in women [3,27,28].
According to the WHO’s report [7], the prevalence of overweight in the southern region and at the national level in Iran is low, in the central region is medium, and in the western and northern parts of the country is high. Additionally, the prevalence of wasting in the western and central regions is low, in the southern region is high, and in the northern parts of the country and at the national level is scarce. Based on the Millennium Development Goals report published in 2015 [22], the prevalence of overweight at the national level in Iran is lower than the global prevalence and those in developing countries [22]. In this study, the subnational division was performed based on the geographical regions and SES of the parts of the country. Previous studies considered these two factors and employed the principle component analysis method to divide the country into four large regions. In this study, based on SES, Iranian regions were ranked from highest to lowest as follows: central, west, north-northeast, and southeast [29,30]. The prevalence of wasting is in accordance with the SES of these regions. For instance, the central and western regions with the highest SES had the lowest prevalence of overweight, and the southeast region with the lowest SES had the highest prevalence of wasting. However, this association was not observed in the prevalence of overweight.
One of the effective factors in estimating the prevalence of underweight and wasting, in different provinces of Iran, is GDP. GDP is the best indicator for measuring the prosperity in a society. It also shows the total income of the country as well as the total cost of producing commodities and providing services. Therefore, GDP per capita represents the means of income and expenditure for each person. Since most people seek more money and prosperity, GDP per capita can be used as a common indicator for measuring the economic prosperity of an individual. By employing the report published by the Islamic Parliament Research Center of the Islamic Republic of Iran, GDP was estimated for different provinces in the country, and then considering the share of GDP in each province, the total prevalence of underweight and wasting among children below 5 years old in these provinces was estimated and compared. As shown in the figure, the average GDP in the central provinces of Iran is higher than that in other provinces. However, the results of this study showed that the pooled estimates of the prevalence of underweight and wasting in the central and southern regions is higher than that in the other regions (west and east). Although the central areas have a high GDP share, the prevalence of underweight and wasting in the provinces in this region is higher than that in other provinces.
The following may be the reasons behind this contradiction:
Firstly, GDP cannot, at any rate, be employed to measure the level of children's health and educational quality. Secondly, the articles combined in this study to estimate the prevalence of underweight and wasting have high levels of heterogeneity, which can affect the overall results in different regions.
There are other factors that are varied among different regions in Iran and can affect the prevalence of underweight and wasting, including climate, rainfall variability (with the averages of 2,000 mm per year in the northern and western provinces, and 120 mm per year in the central and eastern provinces), and temperature variability (varied from -20°C in the northwest to 50°C in the south) [31]. These climate factors can influence the agriculture industry and the availability of food in the different parts of the country.
Health workforce distribution is a key factor in terms of measuring availability, coverage, and equity of health services. The study by Honarmand et al. [32] showed that in comparison with the other parts of the country, the number of general practitioners, midwives, pediatricians, and gynecologists working in the public sector are lower in the socioeconomically deprived provinces.
The prevalence of wasting and underweight has decreased over the recent years in Iran, and the main reasons behind this decrease are development of healthcare centers and improved access to the health services as well as implementation of primary health care network across the country [22]. According to the results of previous studies, the factors related to underweight and wasting were attributed to prematurity, intrauterine growth retardation, small for gestational age, lack of appropriate and sufficient feeding of infants by mothers’ milk and colostrum, and inadequate health education [33,34].
The results of this study indicated that although the prevalence of underweight and wasting in Iran was low, some regions of the country showed a high prevalence. The main reason for this difference in the prevalence of malnutrition between the regions and provinces is the level of development. Therefore, community-based interventions should be implemented to improve child and mother nutrition in these regions. These interventions improve maternal nutrition before, during, and after pregnancy, along with early initiation of breastfeeding, exclusive breastfeeding, and complementary feeding.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


